


ABSTRACT
OBJECTIVE To apply the recently published Montreal definition of gastroesophageal reflux disease (GERD) in primary care.
SOURCES OF INFORMATION The Montreal definition of GERD was developed by an international consensus group of experts in GERD and primary care physicians using rigorous evidence-based methods along with modern consensus development techniques and a patient-centred approach.
MAIN MESSAGE Gastroesophageal reflux disease can be diagnosed in primarycare based on symptoms alone without additional diagnostic testing. Symptoms reach a threshold where they constitute disease when they are troublesome (cause difficulty) to patients. In addition to the cardinal symptoms of heartburn and regurgitation, people with GERD can also have sleep disturbances, chest pains, or respiratory symptoms. Monitoring patients’ response to proton pump inhibitor therapy can confirm the success of management. Treatment for symptoms of GERD can also heal underlying reflux esophagitis if it is present.
CONCLUSION Primary care physicians can diagnose and manage GERD confidently in most patients by investigating and treating troublesome symptoms without the need for additional investigations or referral to specialists.
The first ever global consensus definition of gastro-esophageal reflux disease (GERD), the Montreal definition, was published recently.1 Developed by an international consensus group of experts and family physicians, the Montreal definition was built using rigorous evidence-based methods along with modern consensus development techniques. The Montreal definition describes a symptom-based, patient-centred approach to diagnosis of GERD. This approach includes a measure of the severity of symptoms by stating that GERD is “a condition that develops when the reflux of gastric content causes troublesome symptoms or complications.”1
Heartburn and regurgitation are the characteristic symptoms of GERD. Heartburn is defined as a burning sensation in the retrosternal area. Regurgitation is defined as the perception of flow of refluxed gastric contents into the mouth or hypopharynx. These symptoms are sufficiently descriptive to be diagnostic. Esophageal and extraesophageal symptoms and syndromes that form part of the framework of GERD also include chest pain, sleep disturbances, cough, hoarseness, and asthma (Figure 1).1 This article aims to encourage physicians to use the Montreal definition to diagnose and manage GERD in primary care. We present an illustrative case description.
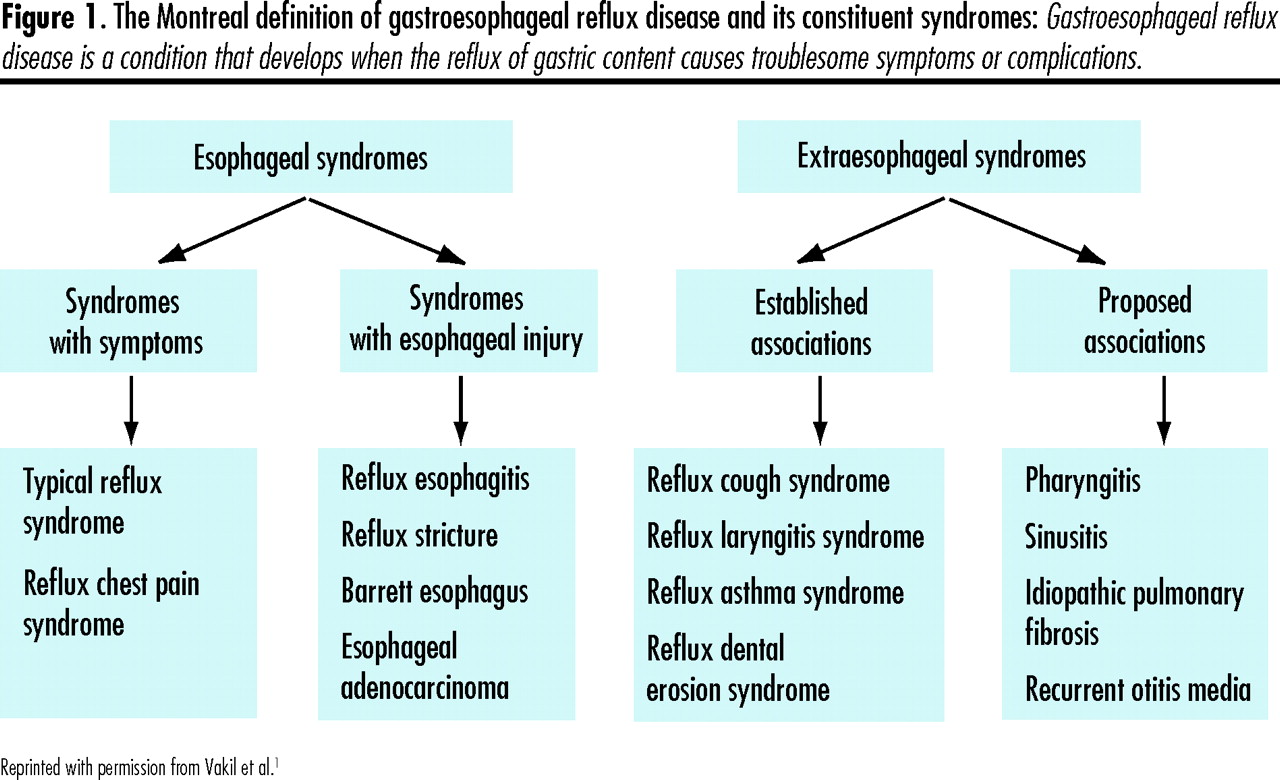
Gastroesophageal reflux disease is a condition that develops when the reflux of gastric content causes troublesome symptoms or complications.
Case description
George is a 48-year-old computer programmer who enjoys playing squash in a top-tier league 3 times a week. He consults his primary care physician because for a year he has had a persistent cough that wakes him in the night several times a week. The cough is accompanied by regurgitation and is often associated with nonradiating retrosternal pain. George occasionally sips water to try to “settle the cough,” but this gives little relief. The sleep disturbances associated with these symptoms lead to tiredness and difficulty concentrating at work. George also gets retrosternal pain and regurgitation during the day, particularly after a large meal. He worries that the chest discomfort could be a sign of heart disease because of his stress at work, and he hopes treatment will restore his productivity at work.
Sources of information
The Montreal definition and classification of GERD was developed by an international consensus group of experts and family physicians over a period of 2 years.1 A series of statements was drafted based on evidence from systematic reviews of the literature in 3 databases (EMBASE, Cochrane Central Register of Controlled Trials, and MEDLINE). The group went through 4 rounds of voting to modify and approve the statements.
Diagnosis
Symptom-based diagnosis of GERD (level III evidence)
The primary care physicians who contributed to the Montreal definition were convinced of the importance of a symptom-based, patient-centred approach to care of people with GERD. This approach was overwhelmingly accepted by the international experts.
The Montreal definition recognizes that GERD can be diagnosed in primary care on the basis of symptoms alone without additional diagnostic testing.1,2 This approach is appropriate for most patients and does not use unnecessary resources. Symptoms reach a threshold where they constitute disease when they are troublesome to patients and affect their functioning during usual activities of living. This patient-centred approach to diagnosis includes asking patients how their symptoms affect their everyday lives.
Chest pain (level II evidence)
Symptoms of GERD can be experienced in the chest or upper abdomen and might be described as burning or painful. Chest pain induced by GERD can closely mimic ischemic heart pain.1,3,4 In managing such cases, a prudent first step is to exclude heart disease as the cause of the pain.
Gastroesophageal reflux disease is thought to cause the chest pain of nearly half the patients with noncardiac chest pain. Patients are often left untreated once cardiac causes have been excluded; studies show that these people then use more health care resources than they did before and suffer functional impairment that goes unresolved until they are correctly diagnosed and treated.5,6
Serious sleep disturbances (level II evidence)
Patients with GERD frequently wake up at night or are unable to get to sleep because of their symptoms.7 Symptoms can be worse when patients lie down. In fact, GERD is a main cause of unexplained sleep disturbances. Sleep disturbances, as well as nighttime reflux symptoms, improve substantially with proton pump inhibitor (PPI) therapy.8
Uncertainty remains as to whether reflux plays a role in triggering apneic episodes in patients with obstructive sleep apnea.1,9 Obesity is a contributory factor to both GERD and obstructive sleep apnea, but the 2 diseases might not be causally related.
Respiratory problems (level II evidence)
The respiratory syndromes associated with GERD include cough, asthma, and laryngitis.1,10–12 These respiratory symptoms are typically accompanied by the cardinal symptoms of heartburn or regurgitation. There are occasional exceptions to this, particularly among elderly people.12 Respiratory problems can be aggravated by GERD, which usually acts as a cofactor in the multifactorial etiology of respiratory conditions, such as asthma or chronic obstructive pulmonary disease. When patients do not have heartburn and regurgitation, GERD is unlikely to be a substantial cofactor in respiratory conditions.
Searching for symptoms of GERD will often be helpful to patients whose respiratory symptoms are poorly controlled despite usual management. Gastroesophageal reflux disease might lead to extraesophageal symptoms if patients aspirate refluxed gastric contents or might stimulate the vagus nerve and bring on reflex broncho-constriction.13,14
Management: the next step
Endoscopy is a poor guide to management (level II evidence)
When large groups of patients are evaluated, a correlation can be seen between the severity of symptoms and the severity of underlying esophageal damage caused by GERD, such as reflux esophagitis. Unfortunately, for individual patients with GERD, the correlation between severity of symptoms and endoscopic findings is poor.1,15 Also, most patients with GERD have no visible evidence of esophagitis at endoscopy, making endoscopic appearance a poor guide to diagnosis and management of GERD. Negative endoscopic findings in the presence of troublesome heartburn or regurgitation are entirely consistent with GERD.1 Patients in these cases are said to have nonerosive reflux disease. Other tests to diagnose GERD, such as esophageal pH monitoring, will not outperform symptom-based diagnosis. Esophageal pH monitoring is not highly sensitive; results of a second test are positive in about one-quarter to one-third of patients whose first test results were negative.16,17 The implication for primary care physicians is that only a few patients need referral for endoscopy or other diagnostic testing for GERD. The few requiring referral include those with long-standing (longer than 5 years) symptoms or symptoms that are unresolved by PPI therapy and those with alarm features. Alarm features include vomiting, gastrointestinal bleeding or anemia, abdominal masses or unexplained weight loss, and progressive dysphagia.2
Acid suppression therapy can guide management (level III evidence)
Regurgitation of gastric acid into the lower esophagus is by far the most common cause of GERD. This is why PPI therapy is effective.1,18 Monitoring patients’ response to PPI therapy is an ideal way to assess the success of management. A few patients will be unresponsive to PPI therapy because they have symptoms caused by reflux of bile containing duodenal contents through the stomach and into the esophagus.1
Serious complications (level II evidence)
The spectrum of reflux disease runs from nonerosive reflux disease through to esophageal complications, such as esophagitis, hemorrhage, and stricture, and to Barrett esophagus and esophageal adenocarcinoma.1 These complications are thought to be due to prolonged and repeated esophageal exposure to acid. Treatment for symptoms of GERD can also heal esophagitis.19 When the diagnosis has been made based on symptoms and a PPI has been chosen for treatment, clinicians can be confident that such treatment is the most effective choice for both the symptoms and the underlying esophagitis, if it is present. Symptom resolution with PPI therapy provides added reassurance about the initial symptom-based diagnosis.
Dysphagia is progressive in a few GERD patients (level II evidence)
Symptoms of GERD can at times lead to some difficulty swallowing food and liquids, and this can cause patients to worry about progressive disease, such as esophageal cancer. Nonprogressive dysphagia is common in patients with GERD, however, and resolves in most patients following treatment with a PPI.20 Dysphagia that gets progressively worse, especially regarding solids, is far less common and represents an alarm feature that warrants further investigation to search for esophageal malignancy or peptic stricture.21 A careful history can identify patients with worrisome symptoms of dysphagia. Referral for contrast studies and endoscopy should not be a reflex response because treatment with a PPI will resolve the nonprogressive dysphagia commonly associated with GERD in most patients.
Barrett esophagus can be diagnosed only on the basis of esophageal histology (level III evidence)
Barrett esophagus is an important marker for changes in the lower esophagus that are associated with increased risk of adenocarcinoma of the esophagus. The proportion of GERD patients in primary care who have Barrett esophagus is unknown but is estimated to be only a few of those with long-standing GERD. The Montreal definition of GERD provides a revised global consensus definition of Barrett esophagus. Endoscopically suspected endothelial metaplasia is the new agreed-upon term for endoscopic findings consistent with Barrett esophagus.1
When biopsies of endothelial metaplasia show columnar epithelium, the condition should be called Barrett esophagus and the presence or absence of intestinal-type metaplasia specified.1 The revised terminology will help primary care physicians to understand the endoscopic and histologic reports they receive and the rationale for including some patients in cancer surveillance programs. Patients with long-standing (more than 5 years) and frequent symptoms, particularly obese men older than 50 years, should be considered for endoscopy to search for Barrett esophagus.1,2
Treatment recommendations (level I evidence)
Important treatment choices for GERD include PPIs and histamine H2 receptor antagonists. There is strong evidence in the literature to support using PPIs because they have superior efficacy compared with histamine H2 receptor antagonists, and this effectiveness comes with equivalent safety. Cost and availability of treatment options are important considerations and will require difficult decisions to be made based on individual and local factors. The emphasis on treatment with PPIs is consistent with recommendations from the current Canadian Consensus Guidelines on Treatment of GERD. This article reports the results of a comprehensive review of the literature and makes recommendations based on a Delphi consensus process. Clinicians reviewing this article will find clear and concise statements to guide their therapeutic choices when treating patients with GERD.22
Case resolution
George’s family doctor reassured him that his chest pain was very unlikely to have a cardiac cause because he was able to play squash at a high level 3 times a week without any chest discomfort. He was diagnosed with GERD based on his symptoms. He has been taking a PPI for 1 month, and his symptoms have improved substantially. He is sleeping well because his cough no longer wakes him. George now feels reassured that his chest pain is not a sign of coronary artery disease, especially as he has not experienced any further chest pain since completing a month of treatment with a PPI. He notices his concentration and work productivity have improved since he has been sleeping better and feeling more rested. He no longer worries about his symptoms, and his quality of life has returned to normal.
Conclusion
The Montreal definition provides a patient-centred, symptom-based approach to diagnosis and management of GERD that will fit well with the care plans of most family physicians. Most patients can be confidently diagnosed based on troublesome symptoms that can be attributed to GERD. Primary care physicians can diagnose and manage most GERD patients without the need for additional investigations or referral to specialists. The Montreal definition can assist primary care physicians in providing safe and effective care for most patients who have GERD.
Levels of evidence
Level I: At least one properly conducted randomized controlled trial, systematic review, or meta-analysis
Level II: Other comparison trials, non-randomized, cohort, case-control, or epidemiologic studies, and preferably more than one study
Level III: Expert opinion or consensus statements
Notes
EDITOR’S KEY POINTS
-
Gastroesophageal reflux disease (GERD) can be diagnosed based on symptoms alone without additional diagnostic testing. The Montreal definition of GERD describes a symptom-based, patient-centred approach to diagnosis of GERD.
-
Response to acid suppression therapy—proton pump inhibitors and histamine H2 receptor antagonists—can guide management. In individual patients, the correlation between endoscopy findings and symptom severity is poor.
-
Endoscopy should be considered in those with longstanding (more than 5 years) and frequent GERD symptoms to search for Barrett esophagus, as well as in those with alarm features (vomiting, gastrointestinal bleeding, anemia, abdominal masses, unexplained weight loss, or progressive dysphagia).
POINTS DE REPÈRE DU RÉDACTEUR
-
Le reflux gastro-œsophagien (RGO) peut être diagnostiqué à partir des seuls symptômes, sans test diagnostique additionnel. La définition de Montréal du RGO décrit une approche fondée sur les symptômes et centrée sur le patient.
-
La réponse à un traitement suppressif—inhibiteurs de la pompe à protons et antagonistes des récepteurs histaminiques H2—permet de diriger le traitement. Pour un patient donné, la corrélation entre le résultat de l’endoscopie et la gravité des symptômes peut être faible.
-
Une endoscopie devrait être envisagée chez ceux qui ont symptômes de RGO fréquents et de longue durée (plus de 5 ans) afin d’éliminer un œsophage de Barrett, ainsi que chez ceux qui présentent des signes inquiétants (vomissements, saignements digestifs, anémie, masse abdominale, perte de poids inexpliquée ou dysphagie progressive).
Footnotes
-
Competing interests
Dr Flook has been involved in continuing medical education or consensus development, received speaker fees or research grants, or been an advisory board member for Altana, AstraZeneca, Bayer, GlaxoSmithKline, Janssen-Ortho, Merck, Pfizer, and Wyeth. Dr Jones has received consultancy and speaking fees from AstraZeneca and Pfizer that involved giving presentations on various aspects of upper gastrointestinal disorders, providing advice on trial design, and taking part in the development of the Montreal definition of gastroesophageal reflux disease.
-
Cet article a fait l’objet d’une révision par des pairs.
-
This article has been peer reviewed.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.