


Answer to Ophthaproblem continued from page 1307
4. Acute retinal necrosis
Acute retinal necrosis (ARN) is a sight-threatening complication of herpesvirus infection that has been reported in immunocompromised and immunocompetent patients. First described in 1971,1 the incidence is 1 case per 1.6 to 2.0 million people.2 The sequelae include uveitis, retinal detachment, blindness, and bilateral involvement. Rapid diagnosis and management are paramount.3–5
The ARN syndrome results from herpesvirus infections: 50% to 70% of ARN cases are caused by the varicella zoster virus (VZV), 20% to 30% by the herpes simplex virus (HSV), 3% to 17% by the Epstein-Barr virus, and 7% by cytomegalovirus.4,6 The median ages of onset of ARN secondary to VZV, HSV type 1, and HSV type 2 are 57, 47, and 20 years of age, respectively.7 However, ARN caused by HSV type 2 has been reported in a few elderly patients,8 and previous herpes simplex encephalitis is a risk factor for ARN.6,9
Patients with ARN generally present with blurry vision, red eyes, periocular pain, photophobia, and floaters. Unilateral anterior uveitis and mutton-fat keratic precipitates can be identified on slit lamp examination in the initial stages of the infection (Figure 1). Vitreous inflammation develops a few weeks later, causing floaters. Granular lesions then appear on the retina and coalesce into thick, yellow-white necrotic patches, predisposing patients to retinal detachment,10 which occurs in an estimated 75% of cases.11 Inflammation in the optic nerve might cause disk swelling and irreversible blindness.10 Poor visual acuity after ARN results from retinal detachment, optic neuropathy, vascular abnormalities, and inflammatory debris within the vitreous humor.11 Bilateral ocular involvement occurs in an estimated two-thirds of ARN patients,11 as the virus might transmit to the contralateral side via the optic chiasm.12 Bilateral disease can occur from 1 week to 20 years after initial presentation.10,13,14 It is a theoretical possibility that the virus can also transmit to the brain parenchyma and cause encephalitis; however, case reports of encephalitis subsequent to ARN were not found in the literature.

Keratic precipitates in the left eye
Diagnosis
Box 115 lists the American Uveitis Society criteria for the diagnosis of ARN. The diagnosis should be confirmed by polymerase chain reaction (PCR) analysis of vitreous samples.
American Uveitis Society diagnostic criteria for ARN
Standard diagnostic criteria for ARN include the following:
|
ARN—acute retinal necrosis.
Data from Holland.15
Differential diagnoses for ARN include various infectious, autoimmune, traumatic, and neoplastic causes.10 In particular, infectious diseases, including toxoplasmosis, syphilis, and tuberculosis; autoimmune diseases, including Behçet disease and sarcoidosis; and intraocular lymphomas can present similarly to ARN. Cytomegalovirus retinitis and progressive outer retinal necrosis, which affect immunocompromised patients, can also present similarly to ARN. Thus, the patient’s clinical history is important in determining the diagnosis.
The following tests might support the diagnosis: B-scan ultrasonography to assess for retinal detachment, especially if a proper fundoscopic examination (Figure 2) cannot be performed; visual field examination to assess for visual field defects; and computed tomography or magnetic resonance imaging to look for optic nerve and brain involvement (Figure 3). To help rule out other infectious causes, the following tests can be performed: lumbar puncture, HIV serology, chest x-ray scan, tuberculin sensitivity test, blood test for syphilis, and titres to toxoplasmosis, HSV types 1 and 2, VZV, and cytomegalovirus.

Retinal findings of acute retinal necrosis: Retinal photography reveals occlusive vasculopathy, retinitis, and optic cup swelling in a patient with a similar condition. The retina could not be visualized in our patient.
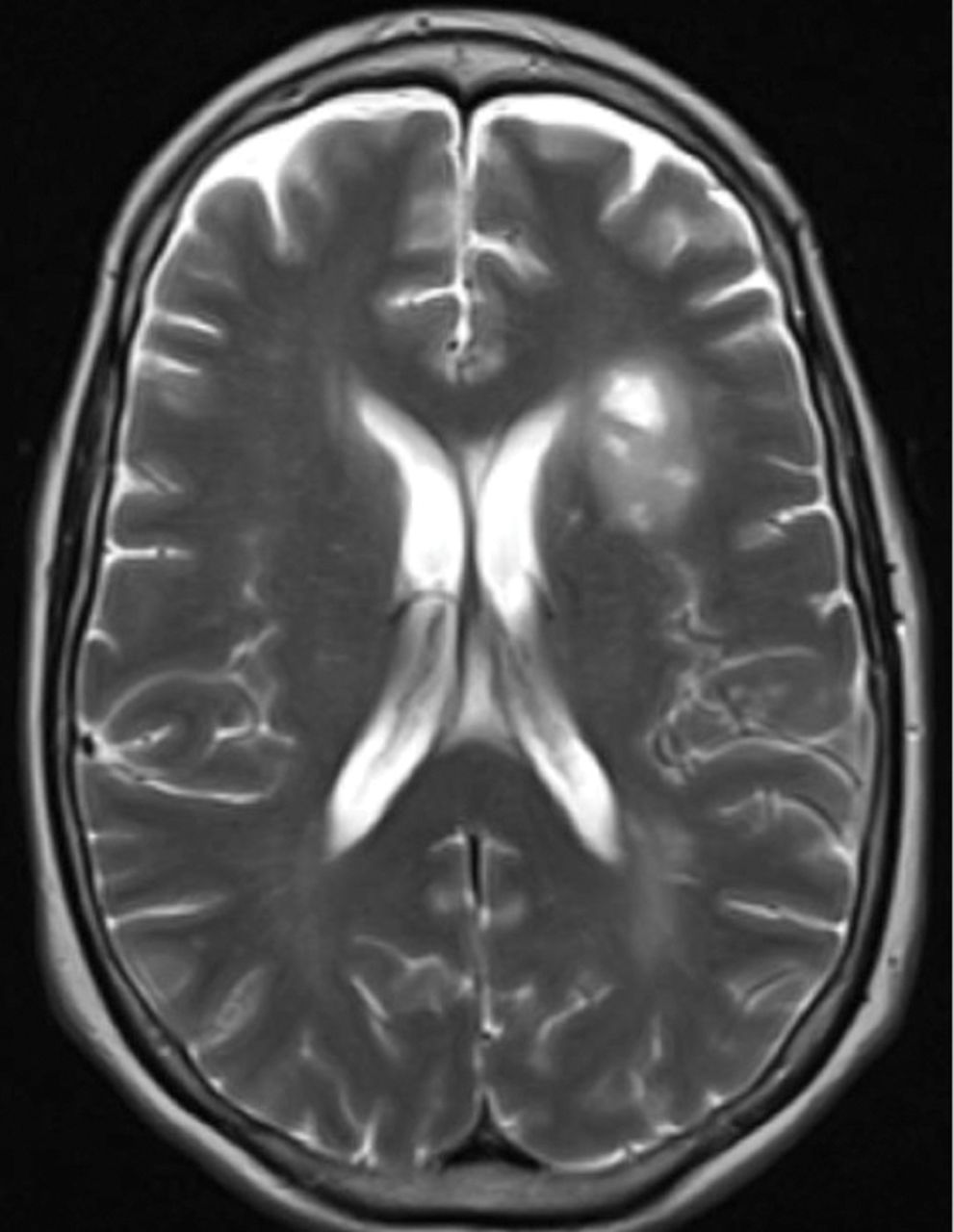
T2-weighted magnetic resonance image showing involvement of the left frontal and parietal lobes:This image was taken 2 months after the patient initially presented with herpes simplex encephalitis.
Treatment
Acute retinal necrosis is an ophthalmic emergency: prompt diagnosis and treatment are the cornerstones of its management. The goals of treatment are to control disease in the affected eyes, to prevent spread of the disease to the contralateral eye and to the central nervous system, and to prevent recurrence. Hospital admission might be necessary to administer intravenous (IV) antiviral therapy while awaiting possible surgery, and frequent outpatient follow-up is crucial to assess for any further complications. Coordination with an infectious disease specialist is recommended, given the need to administer systemic antiviral medications and to evaluate patients for encephalitis. More important, empiric institution of antiviral therapy should not await PCR confirmation of herpesvirus infection.
Medical management of the disease consists of using IV acyclovir, oral valacyclovir, or intravitreal foscarnet to control the virus, as well as consideration of systemic corticosteroid therapy. Several small case studies support patients starting 10 to 15 mg/kg of IV acyclovir 3 times a day while in hospital, and switching to 1 g of oral valacyclovir 3 times a day for at least 8 weeks, if not longer, once they are discharged.16 In one case series in which patients were prescribed oral valacyclovir for 2 to 8 months, visual acuity improved in 60% of eyes, and there was no evidence of contralateral spread over the course of 72 weeks.17 Despite the lack of long-term trials to define the duration of therapy, the indefinite use of valacyclovir should be considered, especially given reports of recurrences or progression of the disease years after diagnosis.
Intravitreal foscarnet is a newer adjuvant for ARN management. It ensures rapid drug delivery to the infected eye, but systemic antiviral drugs are still necessary to prevent brain and contralateral eye involvement. There have been no prospective, randomized clinical trials conducted to assess the effectiveness of intravitreal foscarnet. However, one study reported that foscarnet adjuvant therapy conferred a 67% lower risk of retinal detachment compared with standard acyclovir treatment.3
The use of systemic corticosteroids also has not been studied to a satisfactory degree and remains controversial. A few case reports suggest corticosteroids can precipitate ARN owing to immunosuppression.18,19 Given the high frequency of optic nerve involvement in ARN, some recommend administering high-dose systemic corticosteroids along with antiviral therapy at the onset of disease and tapering over the course of 2 to 6 weeks.16 Until higher-quality studies are conducted, the decision to use corticosteroids is a clinical judgment.
A vitrectomy is indicated when ARN results in retinal detachment. However, vitrectomies have also been performed for patients who are poorly responsive to medical therapy and have no signs of detached retina; one study shows an improvement in visual acuity in 72% of eyes receiving prophylactic vitrectomy.20 Prophylactic laser photocoagulation is another promising approach to preventing retinal detachment; in one study, the incidence of retinal detachment in those who underwent laser photocoagulation was 35% compared with 80% in those who did not.21
Conclusion
Acute retinal necrosis is a devastating manifestation of herpesvirus infection. If the retina is obscured on fundoscopic examination, B-scan ultrasonography can rule out retinal detachment; visual field tests, computed tomography, and magnetic resonance imaging can reveal the extent of optic nerve involvement. The diagnosis of herpesvirus infection should be confirmed by PCR analysis while excluding other causes of ARN via blood tests.
Treatment options have improved since ARN was first described more than 40 years ago: IV acyclovir, oral valacyclovir, and intravitreal foscarnet are potent mainstays of modern therapy. Systemic administration of corticosteroids is controversial, and various prophylactic and restorative surgeries are sometimes required. Confirmatory tests, such as PCR analyses on vitreous samples, are helpful in determining the causative virus. However, when a clinician suspects ARN, empiric antiviral therapy should be initiated immediately given the severe and progressive nature of this infection.
Despite advancements in ARN treatment, many patients will develop retinal detachment and lose sight permanently. Suspected ARN cases should be referred immediately to an ophthalmologist and monitored indefinitely for encephalitis or disease in the contralateral eye. As our case demonstrates, patients with herpetic encephalitis are at risk for developing ARN, including bilateral disease. Patients with encephalitis should be monitored for ARN and long-term antiviral prophylaxis should be considered.
Footnotes
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.