



Volunteering is popular in many countries. Many people, from high school students to retirees, take the opportunity to use their spare time to serve society. Some volunteer just because they want to do something good. Others do it because volunteer experience is required on applications for certain schools and scholarships. Some classes require that students volunteer as part of the course-work. Sometimes, kids are told by their parents to volunteer.
In Japan, volunteering jobs exist, but volunteering is not nearly as common as in some other countries. Unlike in Canada and the United States, for example, volunteering is not an organized activity, nor a requirement at school or on scholarship applications. Therefore, in Japan, volunteering is for people with very warm hearts and strong wills. In fact, in Japanese university hospitals, essential work is done by volunteers, although they are not formally recognized as such. This article will introduce the mysterious Japanese medical system, and how volunteers fit within it, which even the Japanese people hardly know.
Essential work
I am a Japanese physician. I applied to medical school without knowing anything about physicians’ work. Instead, like every other Japanese student applying to medical school, I spent all of my time studying for the entrance examination. I have often thought to myself, Would it not be more beneficial for students to volunteer at the hospital to have an idea of what they are getting into? Volunteering would also benefit the hospital, especially as Japanese hospitals are constantly short-staffed. At the Shands Hospital at the University of Florida (UF) in Gainesville, for instance, every year 3000 people do volunteer work, which is equivalent to the work done by 80 full-time workers. If Japan could employ volunteers as efficiently as the United States does, it could save a great deal of money within the health care system. However, there are some notable differences in volunteering as practised at UF compared with my university.
Where I work, at Juntendo University hospital in Tokyo, there are more than 400 volunteers. Compared with UF’s 3000 people a year, Juntendo’s number seems paltry. However, while the volunteers at UF are only allowed to work up to 8 hours a week, the volunteers at Juntendo are working far more than 8 hours a day, 5 to 7 days a week. What is interesting here is that some of these volunteers do not even know that they are “volunteering,” and most of them are helping out because they have no choice.
In Japanese university hospitals, some physicians are paid while others are not. In university hospitals, paid doctors are being paid not as physicians but as educational staff of the university. These academic positions are limited; in my department, there are only 6. Academic salaries compensate physicians for their research and teaching activities, but not for the hours they work as physicians. Every other full-time physician working at the hospital (apart from the residents, whose modest salaries are paid by the government) works as a volunteer.
Even the few physicians with academic positions receive salaries that do not keep up with the cost of living. For example, as a physician in Tokyo, after 2 years as a resident and 3 years working for free, I got an academic position, similar to that of a full-time assistant professor in the United States, but at a fraction of the pay. My wage at that time was 200 000 yen, about $2000 (US), a month. The cost of living in Japan is comparatively high; a bestseller called How to Live on Only 3 000 000 Yen a Year (about $30 000 [US]) illustrates that it is possible but challenging to live on such a wage.
Accordingly, in most places, physicians are allowed to take on part-time jobs (except for those with academic positions in the public university hospitals; they are considered to be civil servants, and in Japan civil servants are not allowed to do part-time work). They can use their “academic time,” usually an allowance of 1 to 1.5 days per week, to moonlight at small hospitals that are under-staffed, or to conduct healthy patient checkups (a system well established in Japan that helps to detect early disease; for example, gastric and lung cancers).
However, most of the part-time work physicians take on to supplement their full-time income is worked in nighttime shifts and weekend hours in emergency departments (EDs). The Japanese ED system is different from those in the US and Canada. We have 3 types of EDs: first line, second line, and third line. Third-line EDs are like EDs in North America and are located in certain hospitals and staffed by physicians with specialized expertise in ED services. The first and second lines are done in regular hospitals with beds. The first line has limited resources. They can do only limited blood tests and x-ray studies. The second line can do more blood tests and computed tomography scans. These 2 types of EDs are staffed by part-time workers, most of whom are not trained for ED work. In some unlucky cases, between their regular full-time day jobs (officially “part time”) and weekend and nighttime extra jobs, these physicians can end up working 36 hours (3 shifts) straight without breaks.
Gods or volunteers?
There are 4 major differences between UF volunteers working in the hospital and Japanese “volunteers.” First, the working time is not restricted for the Japanese volunteers. Second, if a Japanese physician has an incident or accident, he or she has to take care of the costs; at UF, unless a volunteer commits an intentional infraction, the responsibility for the problem would rest with the hospital. Third, at UF, people are not allowed to volunteer where they work because it could lead to a conflict of interest between paid work and volunteer work—which is exactly what happens in Japanese university hospitals. Finally, ordinary people in Japan do not know that the university doctors are essentially doing their jobs as volunteers. They think physicians are wealthy.
So why do Japanese physicians not quit and work at private hospitals? I suggest that there are 3 possible reasons. For one, most of the physicians think their situation is normal and do not realize that physicians are treated differently in other countries. When all the physicians are in the same situation and you are the only person complaining, it appears that you are too weak to work as a physician. Second, Japanese physicians are highly revered and must act like gods. Do gods complain about salary, hours, or working conditions? Do gods make terrible mistakes? Are gods cranky and therefore mean? Finally, it has traditionally been difficult in Japan to move from a university job to private practice. In the past, one needed to have a recommendation from the university hospital when applying for another position. In 2004, the government introduced a residency matching system that partially mimicked the US system. Medical school graduates are matched with hospitals, not departments, and choose their specialties after finishing their residencies. As a result, the problem now is that most new residents are flocking to the large, private hospitals, which leaves university hospitals with a dearth of physicians. Those physicians who stay do so not for lack of opportunity elsewhere, but for concern for their patients. If the doctors leave, who will take care of their patients?
When radiation oncologist and researcher Dr Ritsuko Komaki from the University of Texas MD Anderson Cancer Center visited Japan in June 2006, the local media interviewed her. She remarked that “Japanese physicians are still gods, whereas U.S. physicians are servants of the patients” (unofficial translation).1 That age-old system is slowly changing; Japan is in transition now. A physicians’ union was launched in Japan in January 2008 and its first demonstration, called Doctors’ Walk, was held on November 20, 2011 (2500 people joined the walk, and 800 of them were medical professionals). Participants in this event rallied for administrative reforms in the Japanese medical community. The union requested sufficient public health expenditures, to a level at least as high as the average reported among countries in the Organisation for Economic Co-operation and Development’s health data reports.2 Specifically, the union demanded sufficient staffing of health care providers; because Japan restricts the number of people who attend medical school, becoming a physician is unbelievably competitive, which has resulted in a paucity of physicians relative to other countries’ health care systems (Figure 1).2 The Doctors’ Walk demonstrated the desire Japanese physicians have for improvements in the country’s health care administration. The public is starting to question the Japanese system of health care, despite its high performance ranking by the World Health Organization.3,4
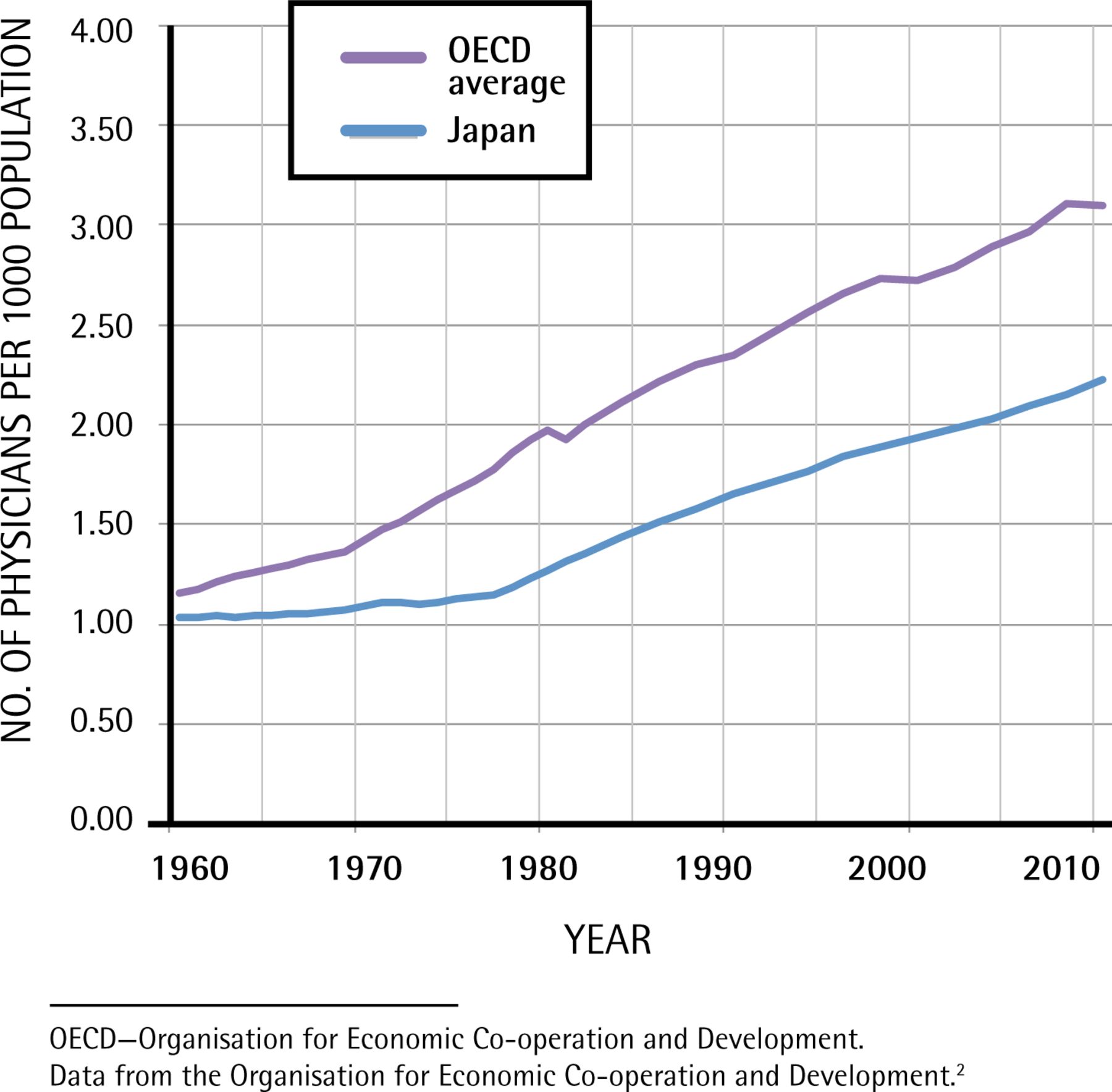
Number of practising physicians per 1000 population: Japan versus OECD member countries’ average by decade,1960–2010.
OECD—Organisation for Economic Co-operation and Development.
Data from the Organisation for Economic Co-operation and Development.2
Conclusion
The medical profession has always been a calling to serve others, with warm hearts and strong wills. Perhaps in Japan it would be more fitting to acknowledge that we are not gods, but here to serve our patients. As such, we should be paid respectfully for our expertise, time, and service. Perhaps, too, as the workings of health care in Japan lose some of their mystery, we will move to a system of true choice, where the lines between paid work and volunteer work are more clearly drawn.
Footnotes
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.