


Article Figures & Data
Figures
- Figure 1.
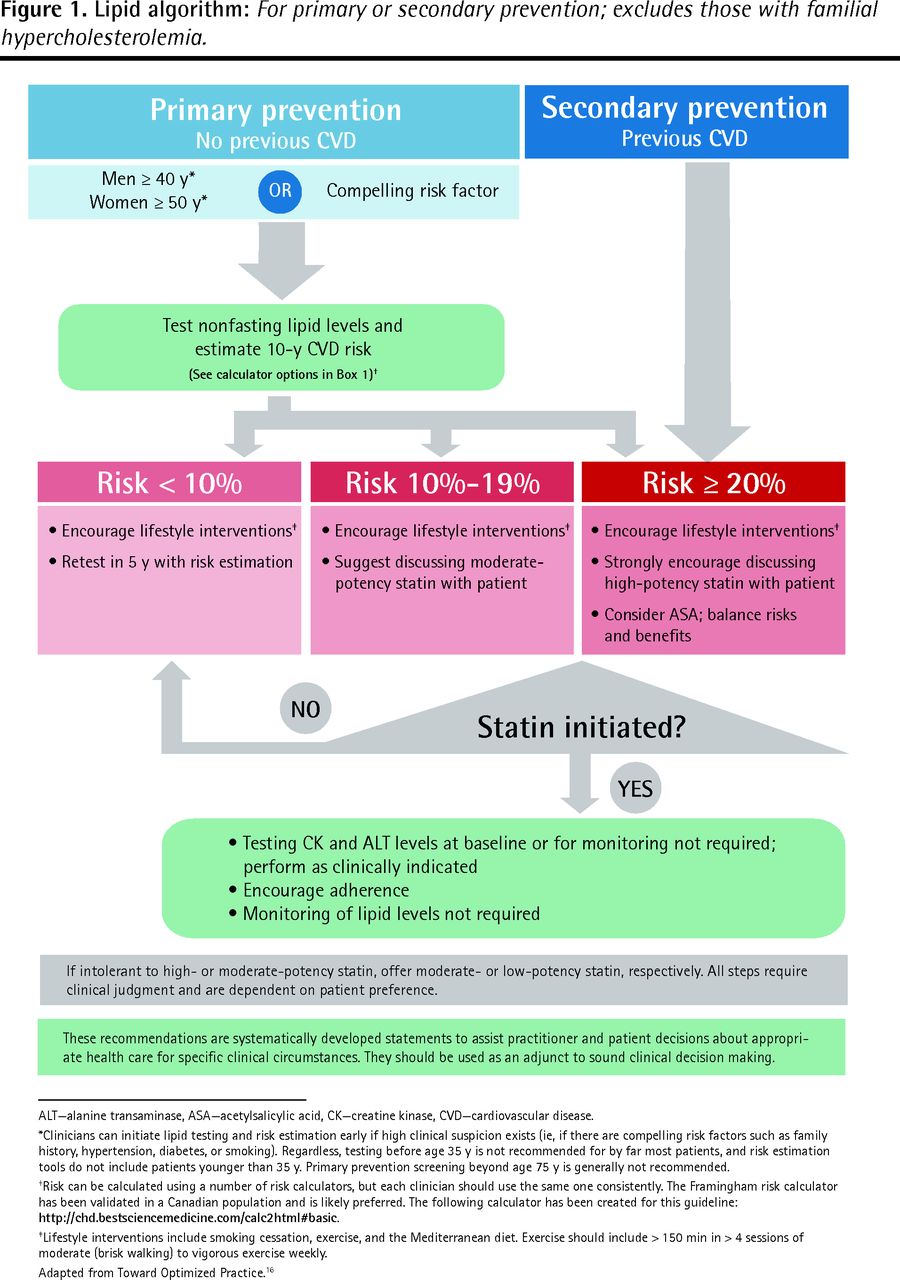
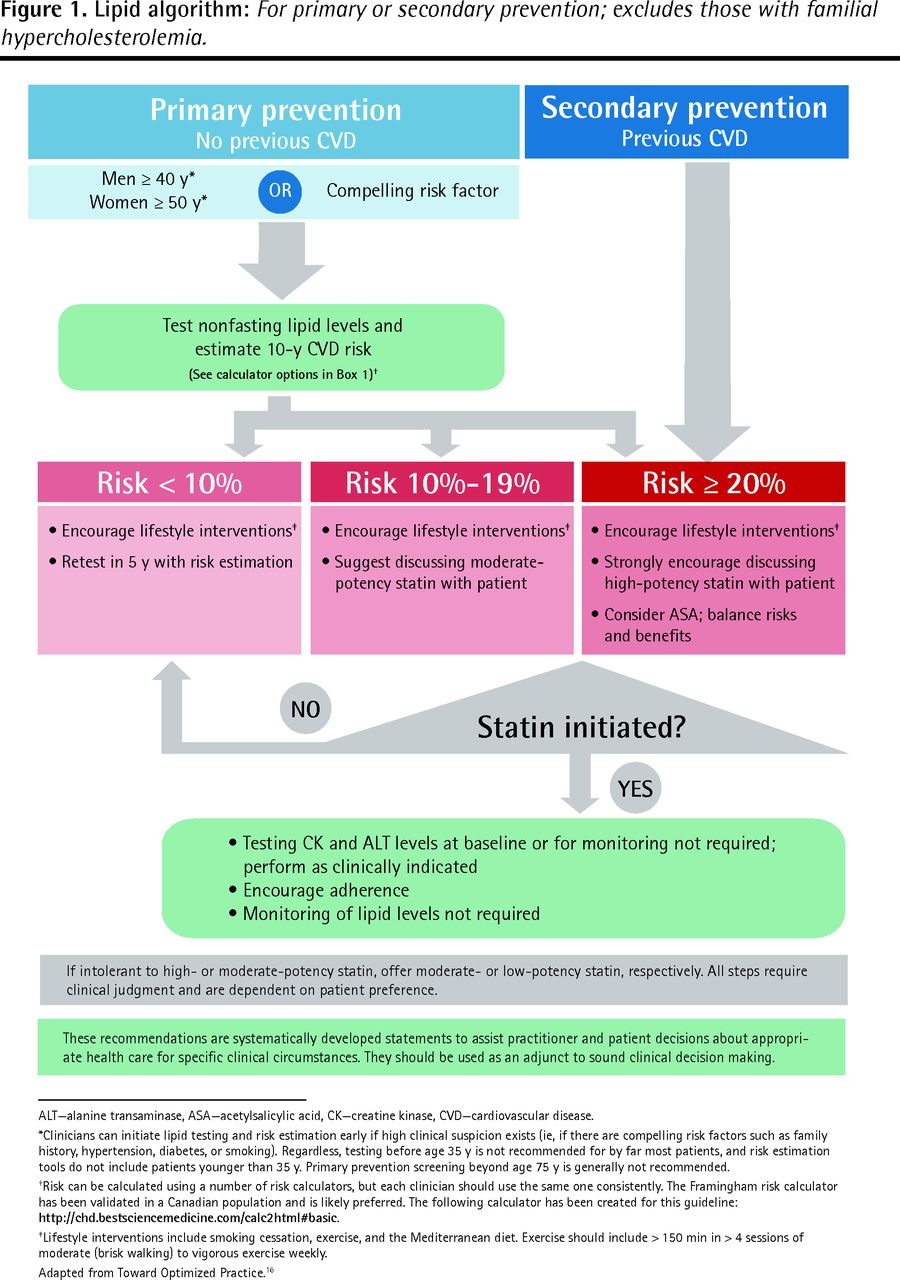
Lipid algorithm: For primary or secondary prevention; excludes those with familial hypercholesterolemia.
ALT—alanine transaminase, ASA—acetylsalicylic acid, CK—creatine kinase, CVD—cardiovascular disease.
*Clinicians can initiate lipid testing and risk estimation early if high clinical suspicion exists (ie, if there are compelling risk factors such as family history, hypertension, diabetes, or smoking). Regardless, testing before age 35 y is not recommended for by far most patients, and risk estimation tools do not include patients younger than 35 y. Primary prevention screening beyond age 75 y is generally not recommended.
†Risk can be calculated using a number of risk calculators, but each clinician should use the same one consistently. The Framingham risk calculator has been validated in a Canadian population and is likely preferred. The following calculator has been created for this guideline: http://chd.bestsciencemedicine.com/calc2html#basic.
‡Lifestyle interventions include smoking cessation, exercise, and the Mediterranean diet. Exercise should include > 150 min in > 4 sessions of moderate (brisk walking) to vigorous exercise weekly.
Adapted from Toward Optimized Practice.16
Tables
Screening and testing Initiating screening: In patients without CVD (primary prevention), we suggest lipid testing as part of global CVD risk estimation in men at age ≥ 40 y and women at age ≥ 50 y (moderate-level evidence).
-Testing can be considered earlier for patients with known traditional CVD risk factors including, but not limited to, hypertension, family history of premature CVD, diabetes, and smoking (low-level evidence).
Repeat screening: For patients not taking lipid-lowering therapy, we suggest lipid testing as part of global CVD risk estimation, performed no more than every 5 y (moderate-level evidence). Global CVD risk estimation can be repeated sooner if other CVD risk factors develop in the interim.
Patients do not need to fast for lipid testing. Nonfasting lipid levels can be used to calculate global CVD risk (moderate-level evidence).
Risk assessmentsPrimary prevention: We encourage risk estimation with a CVD risk calculator (eg, Framingham) every time lipid testing is performed. Testing and risk estimation should be performed starting at age 40 y in men and 50 y in women (or earlier if indicated by other risk factors) until age 75 y (low-level evidence).
-Primary prevention in patients with diabetes mellitus: We encourage risk estimation as above (low-level evidence).
-Primary prevention in patients with CKD: We recommend using a CVD risk calculator (eg, QRISK2) that includes CKD in its estimation of risk (low-level evidence).
We discourage risk estimation for the following patients:
-Those with pre-existing CVD, as they are automatically at high risk (high-level evidence).
-Those < 40 y (without additional risk factors) and those > 75 y, as risk equations are not based on patients in these age ranges (low-level evidence).
-Patients taking lipid therapy, as calculators are not designed to adjust for changes with lipid therapy (low-level evidence). If risk calculation is desired for patients taking lipid therapy, pretreatment lipid levels should be used and risk should be adjusted for known benefits of statin or ASA therapy.
We discourage the use of biomarkers as part of risk assessment until further evidence is available (moderate-level evidence).
Interventions
Lifestyle interventions, including but not limited to smoking cessation, Mediterranean diet, and exercise, should be discussed with all patients (high-level evidence).
Secondary-prevention patients: We strongly encourage clinicians to discuss the risks and benefits of high-intensity statin therapy with patients (high-level evidence).
Primary-prevention patients: We suggest clinicians discuss the risks and benefits of moderate- or high-intensity statins with their patients based on an individual’s risk of CVD (high-level evidence).
-For patients with a 10-y CVD risk of < 10%, we suggest retesting lipid levels in 5 y with risk estimation (moderate-level evidence).
-For patients with a 10-y CVD risk of 10%–19%, we suggest clinicians discuss initiation of statins (preferably moderate-intensity statins) with patients (high-level evidence).
-For patients with a 10-y CVD risk of ≥ 20%, we strongly encourage clinicians to discuss initiation of statins (preferably high-intensity) with patients (high-level evidence).
Patients who are elderly (based on frailty as much as age) or those with renal impairment can be offered lower-intensity statin therapy (low-level evidence).
Primary prevention patients > 75 y: We discourage routinely testing lipid levels, estimating CVD risk, and prescribing statins (moderate-level evidence).
-Some patients > 75 y whose life expectancy and overall health status are good can be offered statin therapy for primary prevention, but this should be left to the clinician and patient’s discretion (low-level evidence).
Secondary prevention patients > 75 y: We strongly encourage clinicians to discuss the risks and benefits of moderate-intensity statins with patients (high-level evidence).
-Patients already taking and tolerating a statin should not have their statin stopped or reduced just because they have aged beyond 75 y (low-level evidence).
In patients ≥ 65 y, pravastatin should likely not be considered first-line therapy until uncertainty surrounding cancer in this subgroup with this drug is resolved (moderate-level evidence).
Patients who do not tolerate a specific statin regimen should be offered a lower-intensity regimen, with either the same or a different statin, or a short drug holiday followed by rechallenge to help clarify if statins are related to the intolerance (low-level evidence).
-Any statin intensity is preferred to non-statin lipid-lowering therapy (moderate-level evidence).
-Alternate daily dosing can be considered if a patient does not tolerate daily dosing (low-level evidence).
-In patients who have severe reactions like rhabdomyolysis, retrial might not be appropriate (low-level evidence).
In primary prevention, non-statin lipid-lowering drugs should not be used as first-line monotherapy or in combination with statins (high-level evidence).
In secondary prevention, ezetimibe can be considered in discussion with patients as add-on therapy to statins, but owing to the higher relative benefit of statins, statin therapy should be maximized first (to high intensity) (high-level evidence).
Follow-upThe use of cholesterol targets for reducing CVD is not required (high-level evidence).
We suggest that the monitoring of repeat lipid levels after a patient begins lipid-lowering therapy is not required (low-level evidence).
-Adherence to statins can be improved with patient reinforcement.
We suggest that testing for baseline CK or ALT levels in healthy individuals before starting statin therapy is generally unnecessary (low-level evidence). The evidence against testing baseline ALT or CK levels is poor and some clinicians might prefer to test one or both.
Routine monitoring of CK and ALT levels should be reserved for those patients who are symptomatic or who are at higher risk of adverse events. Frequency should be determined at the discretion of the attending clinician (moderate-level evidence).
Primary prevention with ASAWe discourage the use of ASA for patients without previous CVD and an estimated 10-y CVD risk < 20% (high-level evidence).
We suggest ASA can be considered in primary prevention if the 10-y CVD risk is ≥ 20% and bleeding risk is low (low-level evidence).
-Use of ASA for primary CVD prevention should be considered after statin therapy has been discussed (high-level evidence).
Patients offered ASA should be informed of the potential benefits and harms of ASA use (low-level evidence).
ALT—alanine transaminase, ASA—acetylsalicylic acid, CT—creatine kinase, CKD—chronic kidney disease, CVD—cardiovascular disease.
QUALITY RATING EVIDENCE High High-quality RCTs: High-quality includes good design, low risk of bias, and confidence in the estimate
Systematic reviews of high-quality RCTs
Moderate RCTs with important limitations: Limitations of RCTs could include inadequate power, poor follow-up, missing quality elements like allocation concealment, per-protocol analysis, etc
High-quality observational studies: High-quality observational studies typically include prospective cohort studies of large populations mirroring Canadian populations and adequate adjustment for confounding
Systematic reviews of RCTs with important limitations or high-quality observation studies
Low RCTs with profound limitations: Profound limitations in RCTs include those listed above but larger and multiple concerns (eg, a trial grossly underpowered for clinical outcomes, CIs that include meaningful harm and benefit, 50% loss to follow-up, etc)
Observational studies with important limitations: Observational studies with important limitations might include retrospective studies, small or specific subpopulations, high-risk confounding, etc
Other lower evidence studies like case series or studies without patient-oriented outcomes (physiologic studies)
Systematic reviews including any of these studies
RCT—randomized controlled trials.
Adapted from Stone et al.2
University of Edinburgh Cardiovascular Risk Calculator: http://cvrisk.mvm.ed.ac.uk/calculator/calc.asp Offers 3 different databases to compare calculated risk; has different display options (some will show statin risk reduction)
Best Science Medicine: http://bestsciencemedicine.com/chd/calc2.html#basicOffers 3 different databases, including Framingham and QRISK2, to compare risks; shows potential benefit of different interventions
QRISK2: www.qrisk.orgIncludes chronic kidney disease in risk estimation
↵* This list is not meant to be all encompassing or to encourage use of one over another. It is simply some suggestions of possible calculators.
THERAPY ESTIMATED BENEFIT (RELATIVE RISK REDUCTION), % EXAMPLE IF BASELINE RISK ESTIMATED AT 20% OVER 10 Y ABSOLUTE RISK REDUCTION, % NUMBER NEEDED TO TREAT NEW RISK ESTIMATE, % Smoking cessation Recalculate risk without smoking 9* 12* 11* Mediterranean diet 30 6 17 14 Exercise 30 6 17 14 Statin intensity • Low 25 5 20 15 • Moderate 30 6 17 14 • High 35 7 15 13 Acetylsalicylic acid 12 2 50 18 ↵* Example used a male smoker, 53 y old, with total cholesterol level of 5.0 mmol/L, high-density lipoprotein level of 1.2 mmol/L, and systolic blood pressure of 128 mm Hg; estimated risk from the Framingham risk assessment tool (from http://cvrisk.mvm.ed.ac.uk/calculator/calc.asp and http://bestsciencemedicine.com/chd/calc2.html) to attain a 20% risk over 10 y.
Adapted from Toward Optimized Practice.16
INTENSITY STATIN OPTIONS Low Pravastatin 10–20 mg; lovastatin 10–20 mg; simvastatin 5–10 mg; atorvastatin 5 mg; rosuvastatin 2.5 mg Moderate Pravastatin 40–80 mg; lovastatin 40–80 mg; simvastatin 20–40 mg; atorvastatin 10–20 mg; rosuvastatin 5–10 mg High Atorvastatin 40–80 mg; rosuvastatin 20–40 mg Adapted from Stone et al.2
- Table 4.
Incidence rates per 100 000 person-years for muscle- and liver-related adverse effects with statins
ADVERSE EFFECT INCIDENCE PER 100 000 PERSON-Y DIFFERENCE (95% CI) STATIN PLACEBO Elevated ALT level (> 3 times ULN) 300 200 100 (64 to 140) Liver failure ∼0.5 NA NA Elevated CK level (> 10 times ULN) 83 60 23 (−4 to 50) Myalgia (muscle pain, tenderness, weakness) 5150 4960 190 (−38 to 410) Myopathy (muscle pain, tenderness, weakness severe enough to stop pills; CK level not always specified) 97 92 5 (−17 to 27) Rhabdomyolysis (poorly defined, except for CK > 10 times ULN) 4.4 2.8 1.6 (−2.4 to 5.5) CK—creatine kinase, NA—not applicable, ULN—upper limit of normal.
Data from Law and Rudnicka.34
CFPlus Additional Information
This data supplement contains the evidence review document, a patient handout, the full disclosure of competing interests and an easy-to-print algorithm.
Files in this Data Supplement:
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence and management of dyslipidemia in primary care practices in Canada
- Lignes directrices simplifiees de PEER sur les lipides : actualisation 2023: Prevention et prise en charge des maladies cardiovasculaires en soins primaires
- Canadian dyslipidemia guidelines for family doctors
- Influenza vaccination for the prevention of cardiovascular events
- PEER simplified lipid guideline 2023 update: Prevention and management of cardiovascular disease in primary care
- Risk of muscle symptoms while taking statins
- Risque de symptomes musculaires avec la prise de statines
- Guideline evolution in family medicine
- Cardiovascular risk factor documentation and management in primary care electronic medical records among people with schizophrenia in Ontario, Canada: retrospective cohort study
- Prise en charge du diabete de type 2 en soins primaires durant la pandemie de la COVID-19
- Managing type 2 diabetes in primary care during COVID-19
- La hausse du facteur dimpact du MFC
- The rise of CFPs impact factor
- Rethinking screening during and after COVID-19: Should things ever be the same again?
- Update to the Preventive Care Checklist Form(C)
- Reforming disease definitions: a new primary care led, people-centred approach
- Acetylsalicylic acid for primary prevention of cardiovascular events
- Prise en charge du trouble de consommation dopioides en premiere ligne: Lignes directrices simplifiees de PEER
- Managing opioid use disorder in primary care: PEER simplified guideline
- Diabetes Canada 2018 clinical practice guidelines: Key messages for family physicians caring for patients living with type 2 diabetes
- Lignes directrices de pratique clinique 2018 de Diabete Canada: Principaux messages a lintention des medecins de famille qui traitent les patients atteints de diabete de type 2
- Nonfasting lipid testing: the new standard for cardiovascular risk assessment
- Do PCSK9 inhibitors reduce cardiovascular events?
- The hidden curriculum and continuing professional development for family physicians
- Simplified guideline for prescribing medical cannabinoids in primary care
- Lignes directrices simplifiees en matiere de prescription de cannabinoides medicaux en soins de premiere ligne
- Statin-prescribing trends for primary and secondary prevention of cardiovascular disease
- Complete blood count for screening?
- Cost effectiveness of case-finding strategies for primary prevention of cardiovascular disease: a modelling study
- Refutation : Les lignes directrices en soins primaires devraient-elles etre redigees par des medecins de famille?: OUI
- For family physicians, by family physicians?
- Les lignes directrices en soins primaires devraient-elles etre redigees par des medecins de famille?: OUI
- Rebuttal: Should primary care guidelines be written by family physicians?: YES
- Lhumour en cote a cote avec les meilleures donnees probantes: Les medecins de famille changent didee a propos des outils, du savoir, de la pratique et de la medecine
- Should primary care guidelines be written by family physicians?: YES
- Laughing alongside the best of evidence: Family physicians change ideas about tools, knowledge, practice, and medicine
- SPRINT to evidence for specific blood pressure targets
- Etude SPRINT : Donnees probantes sur les cibles precises de la tension arterielle
- Lecologie de lengagement des medecins de famille dans la recherche
- Ecology of family physicians research engagement
- Is family medicine ready to look where it is heading?
- Simplified lipid guidelines: Prevention and management of cardiovascular disease in primary care