


This case illustrates a rare cause of acute coronary syndrome (ACS) in young, healthy female patients without traditional vascular risk factors. For family physicians providing acute care in settings where percutaneous coronary intervention (PCI) is not immediately available, decisions regarding thrombolysis and patient transfer to larger centres might hinge on the likelihood of spontaneous coronary artery dissection (SCAD) being the pathogenesis of ACS. Accordingly, rural acute care physicians’ familiarity with SCAD might have a direct effect on patient outcomes.
Case
A 36-year-old previously healthy woman arrived at the emergency department by ambulance. Her spouse had called for paramedics after she complained of severe retrosternal chest pain of approximately 45 minutes’ duration. When the paramedics arrived, the patient had normal vital signs and was able to give a history. Shortly thereafter she lost consciousness, with seizurelike activity for 1 minute and no pulse at the termination of the seizurelike activity. The monitor showed coarse ventricular fibrillation with intermittent torsades de pointes.
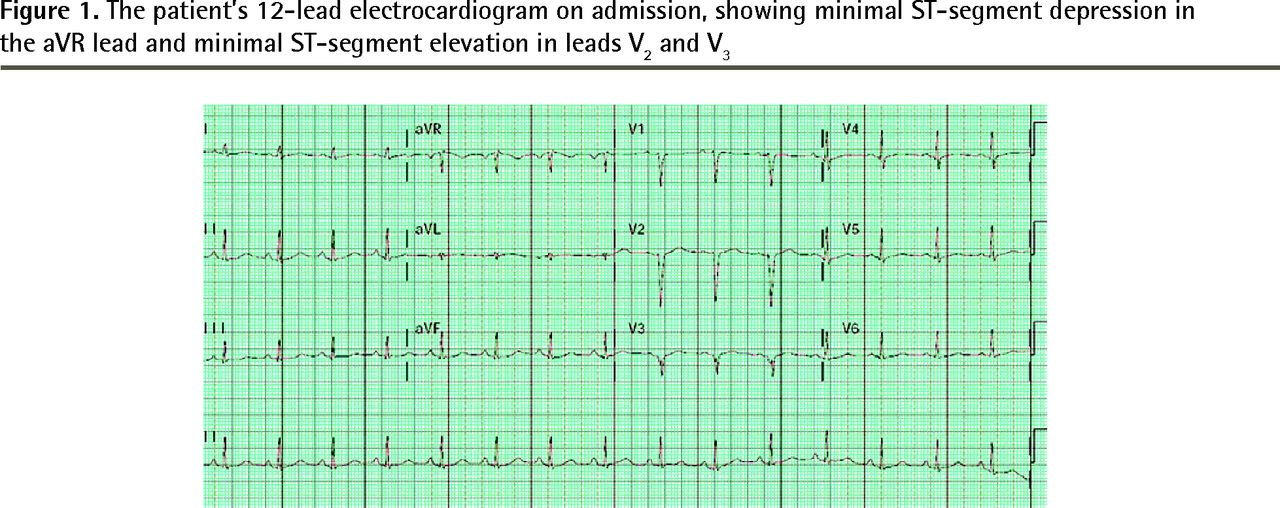
Cardiopulmonary resuscitation was initiated and she was defibrillated twice. On arrival at the emergency department her heart was in sinus rhythm, with a heart rate of 79 beats/min, a blood pressure of 112/79 mm Hg, a temperature of 36.2°C, a respiratory rate of 20 breaths/min, and an oxygen saturation of 100%. She was alert and oriented, with a Glasgow Coma Scale score of 15. Her 12-lead electrocardiogram (Figure 1) showed minimal ST-segment depression in the aVR lead, and minimal ST-segment elevation in leads V2 and V3. Electrocardiogram criteria for ST-segment elevation myocardial infarction (STEMI) were not present. Her corrected QT interval on initial electrocardiogram was 451 milliseconds. There was no evidence of Brugada syndrome.
She denied any relevant personal medical history, was taking no medications, and denied illicit drug use. Her initial cardiac troponin I level was 4.8 µg/L. Initial treatment included acetylsalicylic acid, amiodarone, and magnesium. There was no recurrence of arrhythmia in the emergency department. She was admitted to the cardiology service for observation and further investigation, with a working differential diagnosis of myocarditis, non–ST-segment elevation myocardial infarction (NSTEMI), or stress cardiomyopathy. Echocardiography on day 1 after admission showed apical akinesia of the left ventricle and a left ventricular ejection fraction of 41%. Her troponin I level peaked at this time, with a value of 5.2 µg/L. She underwent coronary angiography on day 4 of her admission (Figure 2), which showed an isolated, irregularly contoured 70% stenosis of the distal left anterior descending coronary artery without other atherosclerotic changes. The reporting interventional cardiologist favoured a diagnosis of SCAD. Because the patient had no ongoing ischemic symptoms at the time of angiography and acceptable blood flow distal to the dissection (as measured by TIMI [Thrombolysis in Myocardial Infarction] score), she was managed conservatively. Medical management at the time of discharge consisted of dual antiplatelet therapy with 81 mg of acetylsalicylic acid and 75 mg of clopidogrel daily, β-adrenergic blockade with 25 mg of metoprolol twice a day, and 20 mg of atorvastatin daily. She was discharged home, with outpatient cardiac follow-up scheduled in 1 months’ time.
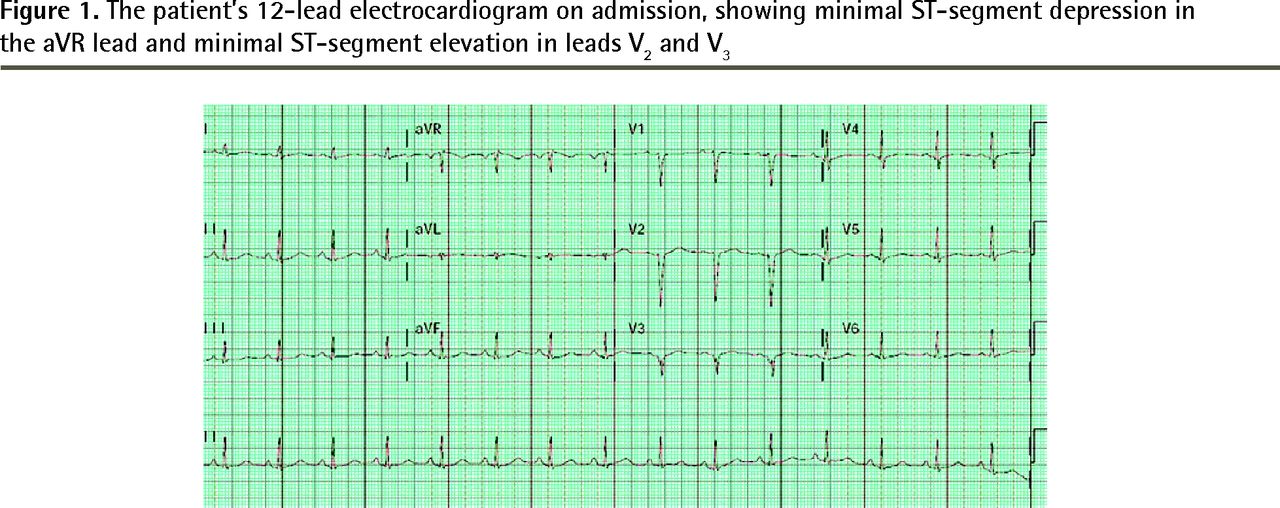
The patient’s 12-lead electrocardiogram on admission, showing minimal ST-segment depression in the aVR lead and minimal ST-segment elevation in leads V2 and V3
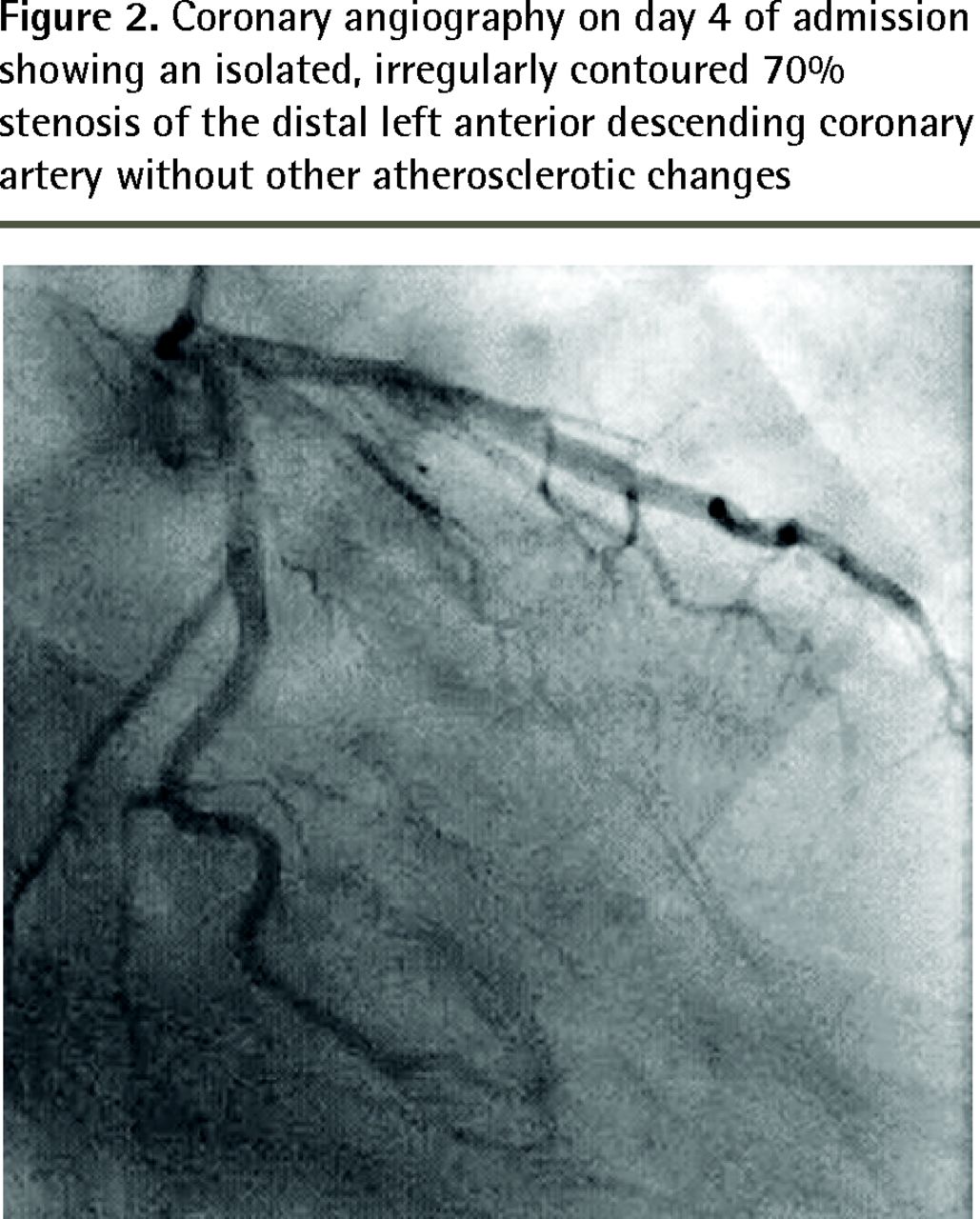
Coronary angiography on day 4 of admission showing an isolated, irregularly contoured 70% stenosis of the distal left anterior descending coronary artery without other atherosclerotic changes
Discussion
A literature search was conducted using PubMed access to the MEDLINE database and the MeSH supplementary concept spontaneous coronary artery dissection among articles published since 2005. This yielded 64 abstracts, of which 5 review articles and larger case series applicable to this case were selected for inclusion.
Spontaneous coronary artery dissection is a rare, potentially fatal condition. It is characterized by an intramural coronary artery hematoma compressing the true lumen in the absence of any iatrogenic cause such as recent catheterization. With an estimated prevalence within angiographic series of 0.1% to 1.1%1 and an incidence of 0.26 per 100 000 in the US population,2 SCAD is thought to account for 0.1% to 4% of all ACS pathologies.3 However, many experts believe the true incidence might be higher.1,3 Among women younger than 50 years with ACS, the prevalence of SCAD is estimated to be as high as 8.7%.3 The “classic” patient demographic is younger women without typical atherosclerotic risk factors, with an average age of 41 to 52 years.1–4 While associations with both oral contraceptive pill use and pregnancy have been described, recent case series suggest these account for a minority of cases.3 For SCAD in the absence of underlying atherosclerosis, there is a strong association with fibromuscular dysplasia.5 Emotional stress, physiologic stress, and stimulant use have been described as precipitating factors.1,5
The clinical presentation of SCAD varies from asymptomatic to fatal. Most cases present as ACS. Meta-analyses of case series including both atherosclerotic and nonatherosclerotic SCAD suggest it presents as STEMI in 48% of cases, NSTEMI in 36%, and unstable angina in 6.5%. Stable angina, congestive heart failure, and ventricular arrhythmia comprise the remaining presentations; 8% to 14% of cases present with life-threatening arrhythmia.2 In a case series of nonatherosclerotic SCAD, STEMI was present in 26.1% of cases, ST depression or T-wave inversion in 29.7%, normal ST segments in 22.0%, and ventricular arrhythmia in 3.6%.5
A diagnosis of SCAD should be suspected in any case of ACS or ventricular arrhythmia in a younger female patient without risk factors. Coronary angiography remains the cornerstone of diagnosis1–3 and is required to rule out thrombotic causes of ACS. A double lumen flap is characteristic of the condition, but subtler forms might be difficult to distinguish from vasospasm or atherosclerosis.1,2 In cases of diagnostic uncertainty, intravascular ultrasound has demonstrated good capability at delineating true from false lumens and establishing a diagnosis.1–3 Endovascular optical coherence tomography has the additional advantage of allowing visualization of the point of intimal tearing and is considered the criterion standard technique.2 Cardiac computed tomography angiography is thought to be nonsensitive, and is not a first-line diagnostic technique.1,2 Similarly, the role of cardiac magnetic resonance imaging is unclear in diagnosing SCAD.1 When SCAD needs to be differentiated from other possible diagnoses, invasive imaging is required and should be done promptly.3 In rural settings, suspicion for SCAD might mean the difference between rapid transfer to a PCI-capable facility and standard NSTEMI or unstable angina care.
Conservative, percutaneous, and surgical management options have all been explored. A balance must be struck between allowing acute thrombus formation within the false lumen to limit progression of the dissection, limiting the risk of plaque rupture of accompanying atherosclerosis, and limiting false-lumen thrombus burden and increasing true-lumen patency.3 There is concern that intravenous thrombolysis might be ineffective, as the primary issue is mechanical occlusion and not thrombosis. Some case series suggest worse cardiac outcomes when thrombolytics are used.1,2 Expert opinion favours revascularization with PCI when necessary, with anticoagulant, antiplatelet, antihypertensive, and lipid-lowering medications forming the core of long-term medical therapy.1–3 Current estimates of 1- and 10-year survival rates are 98.9% and 93.3%, respectively.2
Conclusion
Spontaneous coronary artery dissection is a rare and poorly understood cause of ACS in young patients without risk factors. Physicians providing care in non–PCI-capable centres should be aware of SCAD as a possible cause of ACS.
Notes
EDITOR’S KEY POINTS
Spontaneous coronary artery dissection is a less common cause of acute coronary syndrome that should be suspected in younger female patients without traditional vascular risk factors.
Intravascular techniques are required for diagnosis and treatment, and early transfer to a facility with percutaneous coronary intervention capability is a high priority for presentations with both ST-segment elevation myocardial infarction and non–ST-segment elevation myocardial infarction, particularly in young patients with few cardiovascular risk factors.
The role of thrombolysis in the treatment of spontaneous coronary artery dissection is unclear. Expert opinion favours revascularization when necessary, with anticoagulant, antiplatelet, antihypertensive, and lipid-lowering medications forming the core of long-term medical therapy.
Footnotes
This article is eligible for Mainpro+ certified Self-Learning credits. To earn credits, go to www.cfp.ca and click on the Mainpro+ link.
This article has been peer reviewed.
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro de décembre 2016 à la page e721.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}