

Abstract
Objective To determine family medicine graduates’ professional and personal well-being, general health status, stress levels, coping strategies, and the degree to which they felt supported or isolated in professional life; and to compare findings by sex, practice location, and location of medical school (Canadian medical graduates [CMGs] vs international medical graduates [IMGs]).
Design Retrospective, cross-sectional survey.
Setting University of Alberta in Edmonton and the University of Calgary in Alberta.
Participants A total of 651 graduates who completed one of the family medicine residency programs during 2006 to 2011.
Main outcome measures Using a 5-point Likert scale, graduates rated their general health status, their personal and professional well-being, their level of stress, and the degree to which they felt supported or isolated in professional life. Respondents also identified important life events, their caregiving roles, and stress-coping strategies.
Results Of 651 graduates, 307 (47.2%) responded to the survey. Personal and professional well-being and general health status were rated as very good or excellent by 72.0%, 76.6%, and 74.7% of graduates, respectively. Overall, 39.3% reported high or extremely high levels of stress, with CMGs exhibiting significantly higher stress levels than IMGs (P = .02). Stress scores were inversely related to personal and professional well-being and health status. In terms of coping strategies, a significantly greater proportion of female than male graduates reported talking to colleagues (76.5% vs 64.3%; P = .026) and seeking professional counseling (18.7% vs 6.1%; P = .002). Also, a significantly greater proportion of IMGs than CMGs (52.9% vs 32.5%; P = .003), as well as those in rural (35.8%) or urban (49.3%) practices than those in metropolitan locations (30.1%) (P = .03), turned to spiritual or religious practices for stress management. Of all respondents, 54.8% felt highly or extremely supported and 18.4% felt isolated in their professional lives.
Conclusion While family medicine graduates are primarily healthy and have a strong sense of personal and professional well-being, many experience high levels of stress. Coping strategies generally include social contact with family, friends, or colleagues and differ by sex, whether respondents are CMGs or IMGs, and practice location. Professional isolation appears to be prevalent in both rural and urban practice locations. Physician well-being programs should include a multifaceted approach to accommodate a range of physician preferences.
Most physicians have a rewarding career and enjoy a level of well-being characterized by good to excellent health.1 Unfortunately, a medical career can have adverse effects on some physicians. Medicine is a demanding and high-stress profession characterized by heavy workload, long work hours, limited resources, and high expectations from patients, professional organizations, and health care institutions.2 Physicians also bear witness to emotionally difficult situations such as pain, suffering, and death.3 Moreover, just like other people, physicians experience the personal stresses of everyday life including those associated with marriage, children, family, and personal health.4 All these factors can influence physicians’ well-being.
Studies report that 18% of Canadian physicians are depressed2 and 18% of Canadian medical residents report fair or poor mental health.5 Both cardiovascular mortality6 and suicide6–9 rates have been estimated to be higher for physicians than the general population. Substance abuse issues occur in 6% to 8% of physicians.10 Physician stress is common in primary care,11 with 42.5% of urban Canadian family physicians reporting high stress levels.12 For 43% of physicians, the most stressful aspect of clinical practice is feeling overwhelmed by the workload.2 International data indicate that a third to half of physicians across the globe experience burnout,13,14 and the self-reported burnout rate among Canadian rural physicians was found to be 55%.15 Among US physicians, 45.8% reported at least 1 symptom of burnout, with family physicians experiencing one of the highest burnout rates.16 The stresses experienced by female physicians have been documented,17 with female physicians (36%) being almost twice as likely as male physicians (19%) to report burnout.18 Conflict between work and family has been reported by 86% of female physicians with children.2
The well-being of physicians is important to the health system because physician well-being influences patient care. Studies have shown that a physician’s health and well-being affects the amount and quality of care provided19,20 and overall performance.21 Physicians who lead a healthy lifestyle are also more likely to provide healthy lifestyle counseling to their patients22 and practise healthier medicine.23 Poor physician health has been associated with reduced workload or work effort,24,25 job dissatisfaction,25 medication errors,26,27 and ineffective communication with patients.28 Burnout is associated with decreased productivity.13
In terms of stress management strategies, a Canadian study of academic physicians reported that 33% of participants talked to their spouses and 15% talked to other doctors.2 Lee et al12 found that the most frequently used strategies for coping with stress were eating nutritiously and spending time with family and friends. One study of medical residents in Canada found that 92% spoke with others and 17% used alcohol as coping strategies,5 and another study found that 61.8% of family medicine residents relied on recreational use of alcohol and drugs.29
Studies have revealed that a supportive work and home environment is instrumental in reducing stress and improving the well-being of physicians. Support from co-workers and spouses enhances the well-being of physicians and acts as a buffer against the negative effects of workload, emotional demands, and work-family conflict.2 For female physicians with children, the risk of burnout has been reported to decrease by 40% in the presence of support from colleagues and their spouses for balancing work and home issues.30 A qualitative study of 200 German physicians identified 30 resilience strategies used for successful coping, with the most commonly reported for general practitioners being self-awareness and realism (accepting external realities and holding realistic expectations), leisure-time activity, and gratification from the doctor-patient relationship.31
In recent decades, physician well-being has received increasing attention, with both professional organizations and medical education and clinical training programs placing greater emphasis on physician health and wellness. There is also recognition that physicians have a responsibility for maintaining their own health and wellness. The Canadian Medical Association policy on physician health and well-being states that “Physicians should strive to manage professional stress and maintain their own health and well-being and to maximize their ability to provide quality health care to their patients.”32 This is consistent with the CanMEDS–Family Medicine framework for competencies in family medicine relating to physicians’ professional roles33 and the American Medical Association policy related to physician health and wellness.34
Research on the well-being of Canadian family physicians is scarce. With the focus on primary care reform across Canada, the well-being of family physicians is crucial to a well-functioning health care system. The purpose of this study was to examine how recent family medicine graduates rate their health, life stressors, and stress management strategies. In light of the increasing trend in female family medicine residents, the heavy workload of rural physicians, and the growing number of international medical graduates (IMGs) in family medicine residency programs, analysis of findings by physician sex, physician practice location, and location of study (Canadian medical graduates [CMGs] vs IMGs) was warranted.
METHODS
Study design, participants, and procedures
This was a retrospective, cross-sectional survey of graduates who completed family medicine residency training at the University of Alberta in Edmonton or the University of Calgary in Alberta during 2006 to 2011, inclusive. All graduates (N = 651) for whom contact information was available through the Alberta Medical Directory or the Canadian Medical Directory were mailed the survey. The survey package contained the study information letter, the questionnaire, and a postage-paid return envelope. Nonrespondents were mailed a reminder notice and contacted up to 5 times by telephone, fax, or e-mail. The survey was conducted from July 2013 to December 2014, and each university mailed the questionnaire to its own graduates. The study was approved by the Health Research Ethics Board (Health Panel) at the University of Alberta and the Conjoint Health Research Ethics Board at the University of Calgary.
Survey
The purpose of the overall survey was to examine graduates’ educational experiences during residency training and practice patterns after residency training. The well-being section of the questionnaire asked graduates to do the following: rate their general health status and personal and professional well-being; identify strategies used to manage stress; indicate the degree to which they felt supported or isolated in professional life; note their caregiving roles; and identify important life events. Respondents’ answers were subjectively rated using 5-point Likert scales for health status and personal and professional well-being (1 = poor, 2 = fair, 3 = good, 4 = very good, 5 = excellent), stress levels (1 = none, 2 = low, 3 = moderate, 4 = high, 5 = extremely high), and the degree of feeling supported or isolated in one’s personal and professional life (1 = not at all, 2 = slightly, 3 = moderately, 4 = highly, 5 = extremely).
Data analysis
Statistical analyses were conducted using SPSS, version 22. The data were analyzed descriptively (frequencies, cross-tabulations). Comparisons were made for male versus female physicians, rural versus urban versus metropolitan practice locations, and CMGs versus IMGs. Canadian medical graduates included those who graduated from a Canadian medical school. International medical graduates were physicians who graduated medical school in a country outside of Canada. Practice locations were defined as follows: a population of less than 25 000 for rural practice, a population of 25 000 to 200 000 for urban practice, and a population of greater than 200 000 for metropolitan practice. In Alberta, metropolitan areas include Edmonton and Calgary, each with a population of approximately 1 million. Fisher exact and χ2 tests were used to test for association between categorical variables. Differences in mean well-being scores were compared using ANOVA (analysis of variance). Pearson correlations were calculated to examine the relationship between stress and well-being. An α level of .05 was used to test for statistical significance.
RESULTS
A total of 307 (47.2%) graduates responded to the survey. Most respondents were female (61.2%), married with children (68.1%), and CMGs (76.9%). Respondents’ average age was 38.5 years, with 22.5% practising in a rural location (Table 1).
Characteristics of respondents (N = 307): Mean age of respondents was 38.5 y.
Physician well-being.
In terms of well-being, 72.0% and 76.6% of graduates rated their personal and professional well-being as very good or excellent, respectively (Figure 1). Similarly, 74.7% rated their general health status as very good or excellent (Figure 1). There were no statistically significant differences in the mean scores for personal or professional well-being and general health status by sex, age group, or practice location, or for CMGs versus IMGs.
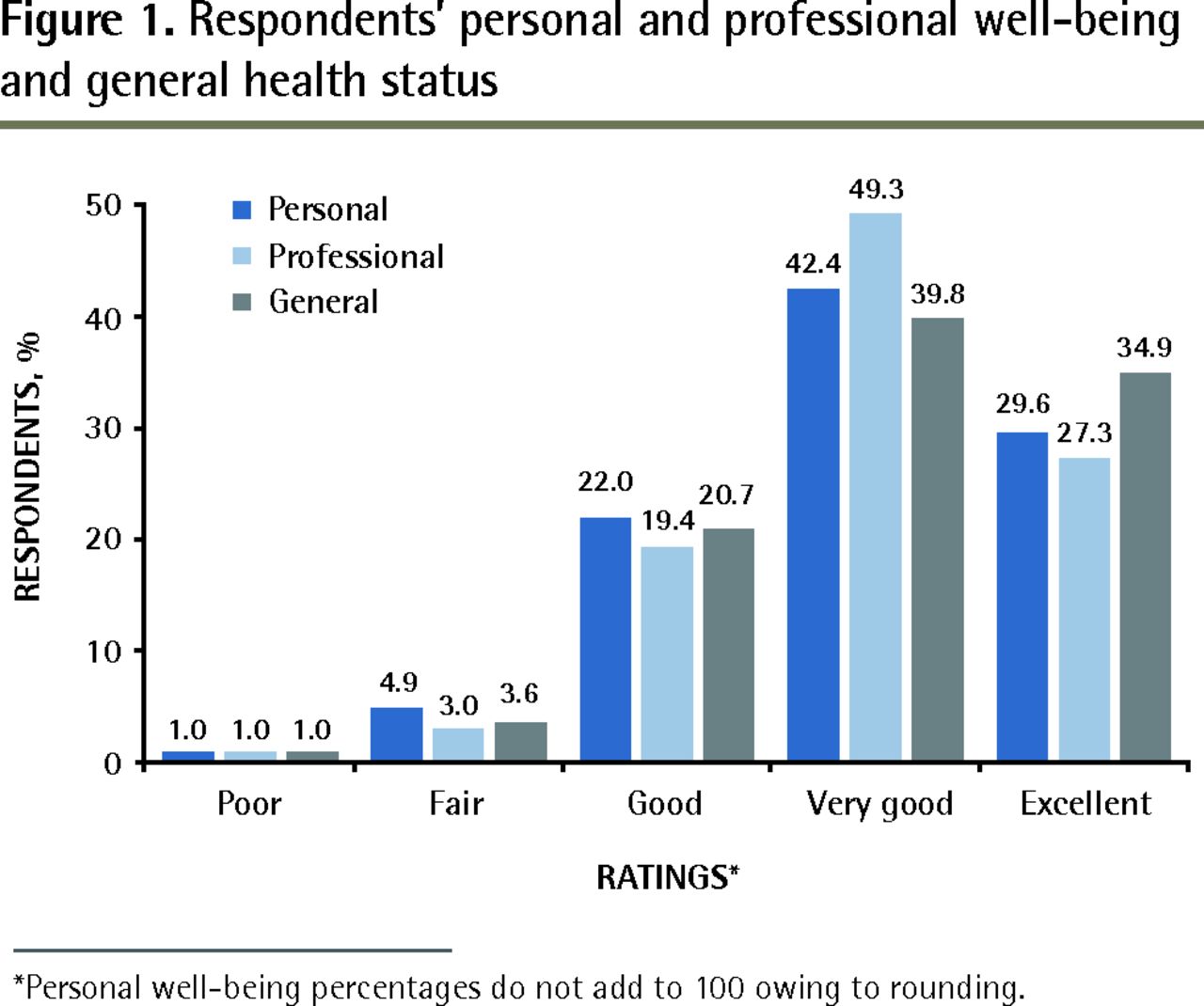
Respondents’ personal and professional well-being and general health status
*Personal well-being percentages do not add to 100 owing to rounding.
Stress levels.
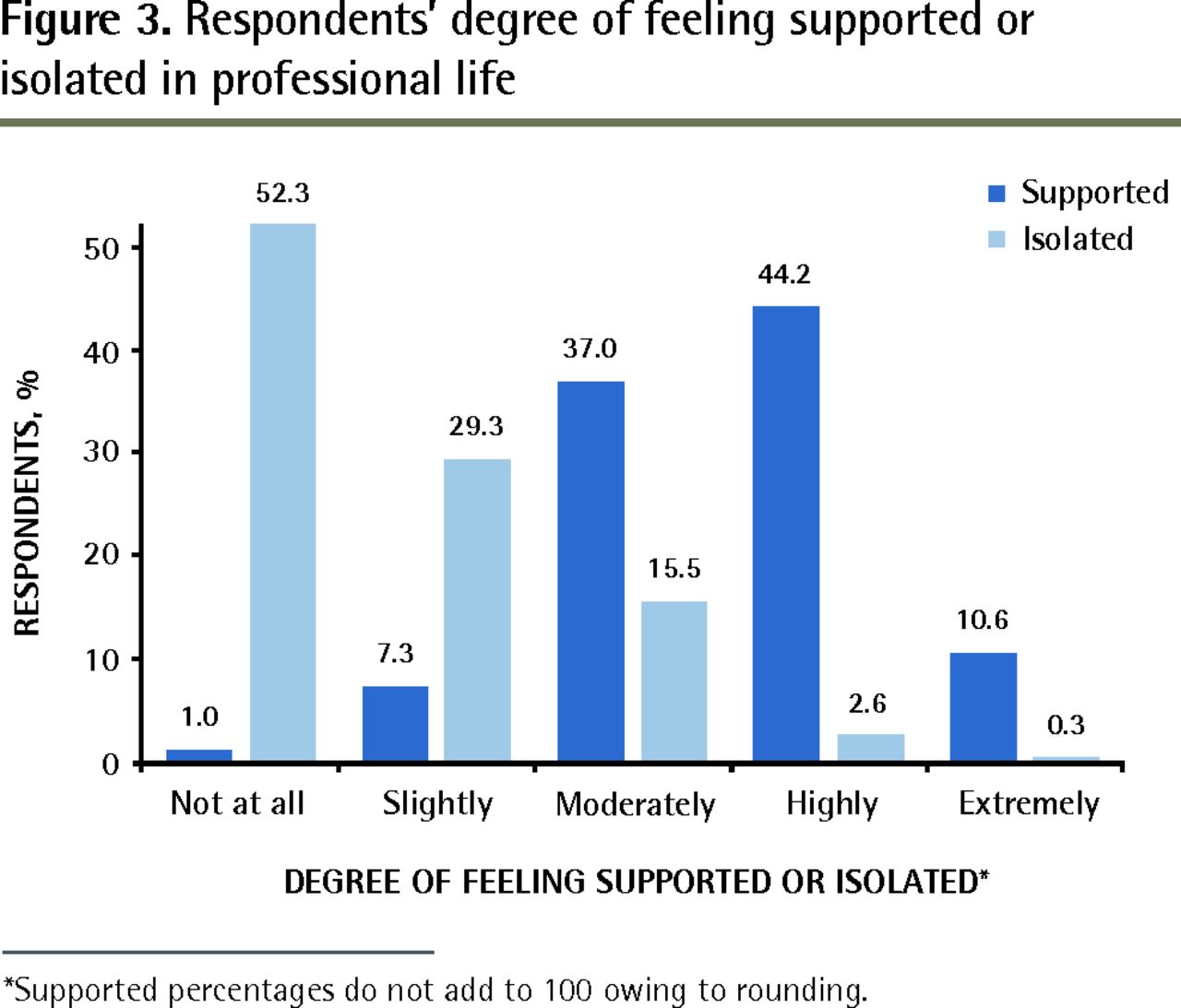
The overall mean (SD) level of stress of 3.31 (0.85) was in the moderate range; however, high or extremely high levels of stress in the 12 months preceding the survey were reported by 39.3% of family physicians (Figure 2). Stress scores demonstrated an inverse relationship with personal well-being (r = −0.38), professional well-being (r = −0.33), and health status (r = −0.33).

Respondents’ overall stress levels in the past 12 months
The top 5 stressors included illness in the family (27.3%), personal health problem (17.6%), professional discord between colleagues (14.4%), death of a family member or friend (13.3%), and other important life events such as the birth of a child, marriage, legal issues, professional issues, moving, or environmental disaster (flooding) (24.8%) (Table 2). A significantly greater proportion of graduates in rural practice (23.3%) experienced professional discord between colleagues than those in urban (7.7%) or metropolitan (13.6%) practice (P = .04). A significantly greater proportion of IMGs (22.2%) than CMGs (10.8%) experienced the death of a family member or friend (P = .03). In contrast, a significantly greater proportion of CMGs (30.8%) than IMGs (7.7%) reported other important life events (P = .001). The mean stress level score for CMGs (3.36) was significantly higher than the mean stress level score for IMGs (3.09) (P = .02), but there was no significant difference in mean stress levels among all respondents’ practice locations.
Life stressors and coping strategies
Caregiving role.
Overall, 61.6% of respondents were primary caregivers for young or school-aged children, with 72.4% of female respondents having this responsibility. While 53.6% reported not having the role of caregiver in the preceding 12 months, 25.7% were caregivers of children and 15.8% of parents who were sick, in poor mental health, or were physically disabled. A significantly greater proportion of IMGs (24.2%) than CMGs (12.9%) had cared for a parent in the past 12 months (P = .03). There was no significant association between caregiving and physician sex or practice location.
Coping strategies.
The most frequently reported strategies for managing stress included talking to family or friends (90.5%), taking part in physical activity (78.9%), taking time off or vacation (78.0%), and talking to colleagues (71.4%) (Table 2). In the “other” category of coping strategies, respondents included having hobbies, listening to music, playing board games, fishing, hunting, shopping, taking medication, and drinking “exactly the right amount.” A significantly greater proportion of female than male respondents reported talking to colleagues (76.5% vs 64.3%; P = .026) and seeking professional counseling (18.7% vs 6.1%; P = .002). Moreover, a significantly greater proportion of IMGs (52.9%) than CMGs (32.5%) (P = .003), as well as those in rural (35.8%) and urban (49.3%) practices compared with metropolitan (30.1%) locations (P = .03), turned to spiritual or religious practices for stress management. Overall, 27.4% indicated taking a leave of absence from practice in the preceding 12 months (33.3% of females), with the average duration of the leave of absence being 4.3 months. Reasons for the leave of absence included maternity or parental leave, health issues, illness in the family, travel or vacation, legal issues, or working or volunteering overseas.
Support and isolation in professional life.
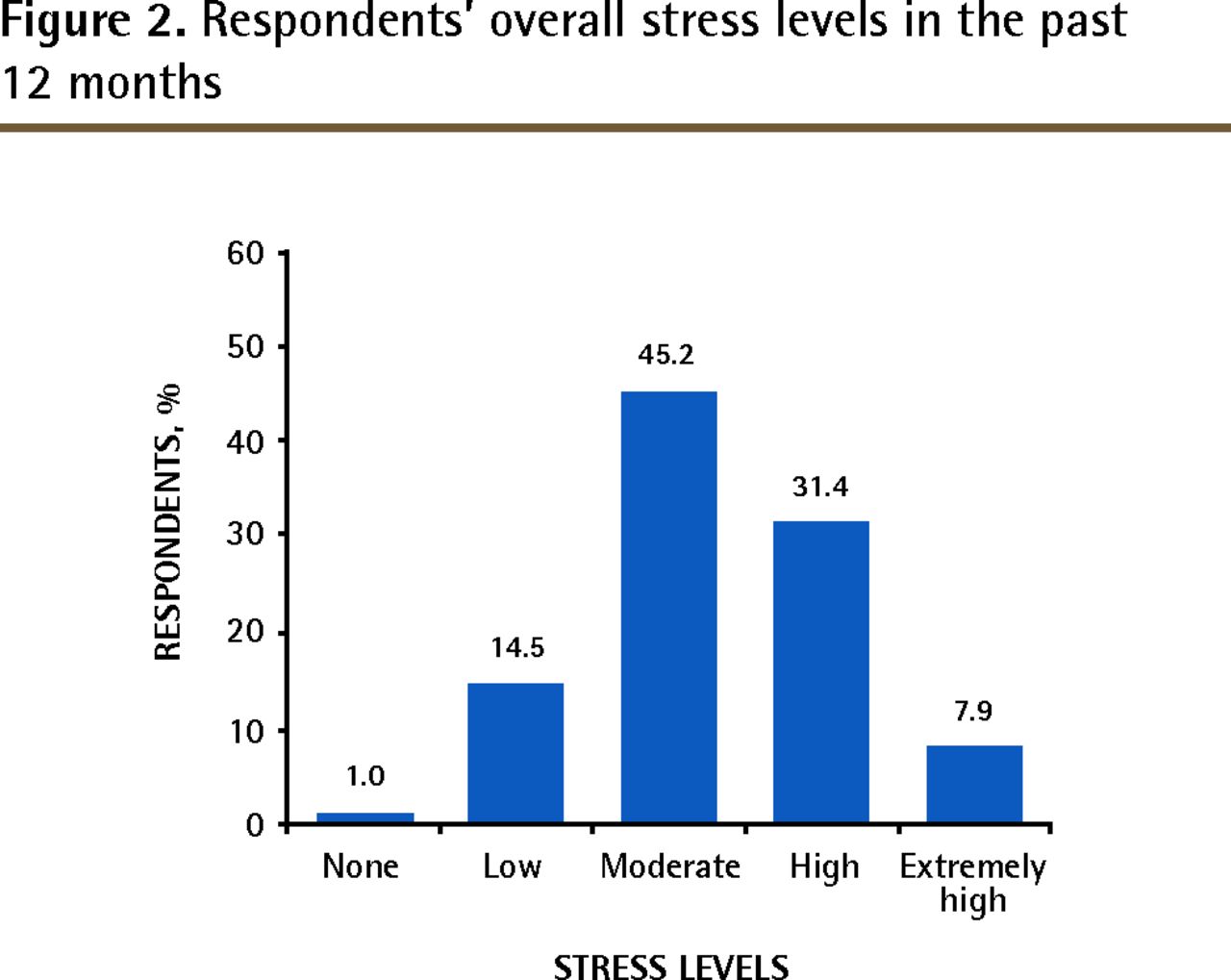
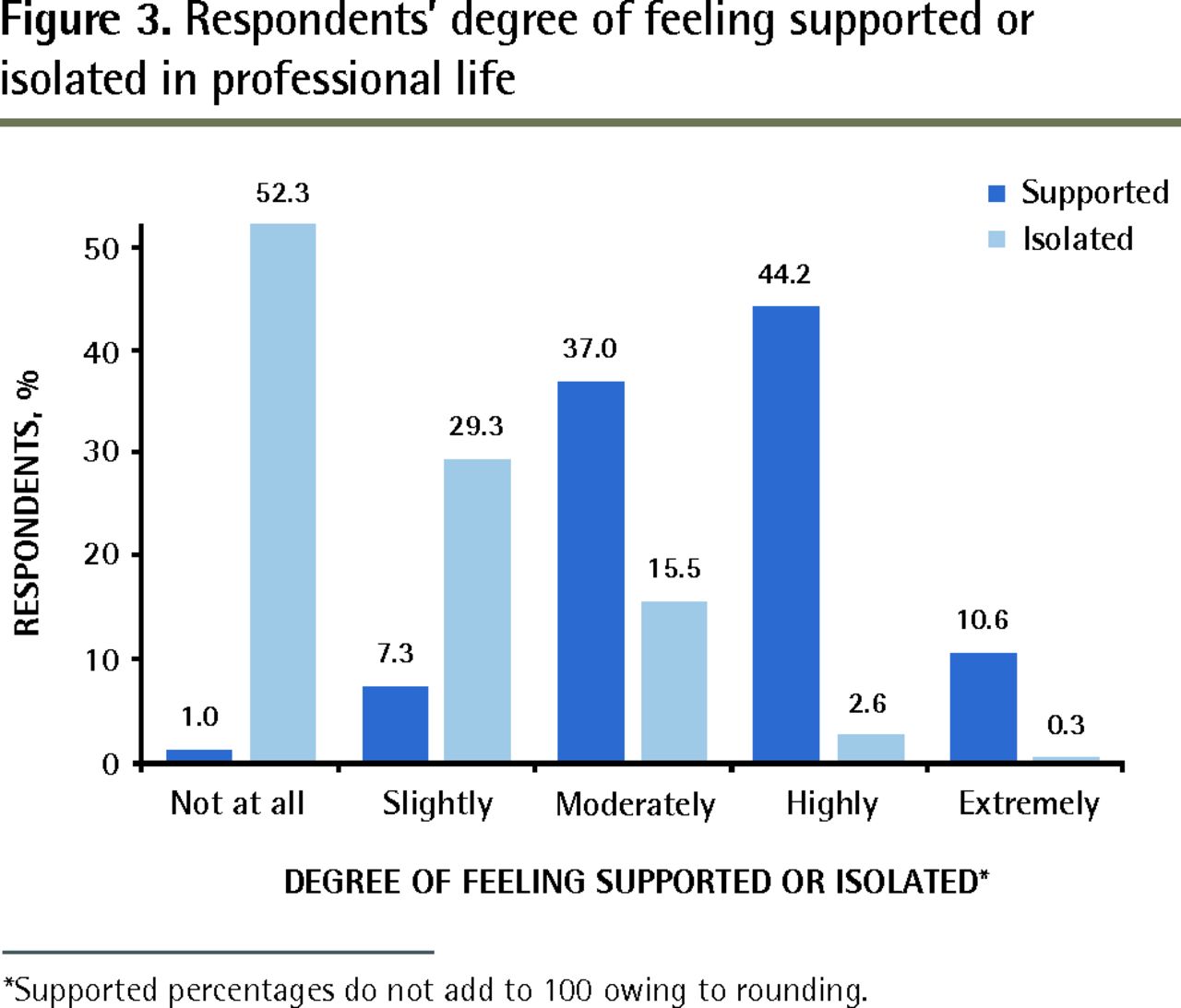
Overall, 54.8% of family medicine graduates reported feeling highly or extremely supported in their professional lives (Figure 3). The primary support mechanisms came from colleagues and co-workers, friends, spouses or family members, and the Alberta Medical Association’s Physician and Family Support Program, as well as from participation in continuing medical education activities.
{kind=link}
{kind=link}
{kind=link}
Respondents’ degree of feeling supported or isolated in professional life
*Supported percentages do not add to 100 owing to rounding.
Of the respondents, 18.4% felt moderately to extremely isolated in their professional lives (Figure 3). The following factors were reported as contributing to isolation: being busy and not having enough time to socialize; the age gap between colleagues; difficulty discussing concerns with colleagues for fear of being labeled a “whiner” or “failure”; a prevailing culture of “mind your own business”; not belonging to the “old boys club”; feeling alone owing to work atmosphere, as physicians at clinics work independently (working solo in group practice); believing that others do not understand how you feel; and self-imposed isolation owing to one’s own personality. There was no significant difference in the proportion of respondents who felt professionally supported or isolated by sex, practice location, whether the respondent was a CMG or IMG, or practice type (solo vs group practice). Overall, 82.8% of family medicine graduates worked in a group practice setting. A statistically significant correlation was observed between stress level and professional isolation (r = 0.21, P < .001).
DISCUSSION
This study revealed that recent Alberta family medicine graduates are primarily healthy and have a strong sense of personal and professional well-being. The relatively good health of these family physicians is reassuring to the health care system given that good health has a positive influence on physician supply and productivity.
Almost 40% of family medicine graduates in our study reported experiencing high to extremely high levels of stress from various sources in the preceding year. These findings are consistent with other Canadian data.35 Medicine is known to be a high-stress profession, one that has a high level of responsibility and little control over outcomes. The daily demands of medical practice (patient care demands, administrative requirements and paperwork, limited resources, etc) coupled with personal life stressors (personal or family illness, child care responsibilities, financial issues, separation or divorce, etc) can result in mental fatigue, exhaustion, stress, burnout, depression, or impairment, affecting the physician’s ability to cope. Higher mean stress scores for CMGs than IMGs could be attributed to differences in age, with Canadian graduates being younger and at a stage in life when they are getting married, having children, and juggling clinical practice and family life. These competing demands are bound to generate work-life conflicts and produce stress, which is “the result of an imbalance between the demands of the workplace and an individual’s ability to cope.”36
Our finding that personal strategies for managing stress typically include social contact with family, friends, or colleagues is consistent with the published literature.5,35 The finding that more female than male physicians manage stress by talking to colleagues and seeking professional counseling is also supported in the literature. A study of gastroenterologists found that women were more likely to use problem-focused coping strategies that included actions such as seeking social support, positive reframing, planning, and active coping to solve or alter the source of stress.37 These findings imply that physician support programs or informal wellness initiatives within the practice setting aimed at female physicians should include elements of social contact and support groups.
More IMGs and those in rural and urban practices turned to spiritual or religious practices (classified as emotion-focused coping strategies)37,38 to manage stress than did CMGs and those in metropolitan locations. Some IMGs have immigrated to Canada from many different countries steeped in traditional cultures; therefore, religious beliefs and practices would be expected to provide a source of strength and play an important role in their lives. One study found that religion was the most frequently used adaptive stress-coping strategy by medical residents in Saudi Arabia.39 Spiritual practices to cope with stress might include spiritual support from a higher power, performance of rituals, support from a religious institution or clergy, or reframing a stressful situation into one of meaningful importance. In contrast, Canadian graduates have been raised in a Western culture that is perhaps more secular and individualistic in nature and generally less reliant on spiritual or religious practices. Generally, churches and religious organizations tend to play an important role in rural communities as a focal gathering point for individuals, which can provide a source of empowerment and optimism in difficult times. In multi-cultural societies, physician wellness initiatives should accommodate individual spiritual or religious practices as a means of coping with stress.
Our finding that 18.4% (almost 1 in 5) of family medicine graduates felt moderately to extremely professionally isolated is somewhat disconcerting, although not surprising. Professional isolation was also found to be positively correlated with stress. Professional isolation denotes a feeling of separation or dissociation from one’s professional peers. Family physicians often work one-on-one with their own patients, which might result in a reluctance to ask for assistance and decreased interaction with colleagues, creating feelings of isolation. Within a group practice setting, the physical association of physicians working together in the same suite of offices might be presumed to mitigate professional isolation; however, our findings support the notion that professional isolation “is not about distance” but “about lack of professional networks and contact.”40 Professional isolation can be a challenge in family practice and, to date, strategies aimed at reducing professional isolation have been targeted primarily at physicians practising in rural and remote locations. It would be remiss to overlook professional isolation in urban areas and in large group practices. Strategies aimed at reducing professional isolation of family physicians might lower stress levels, thereby enhancing physician well-being and patient care. These strategies can include developing professional networking or interest groups, finding a mentor, attending continuing professional development activities, or introducing initiatives to increase social and professional contact with other family physicians and other health professional team members. These can be face-to-face or using online technologies.
Limitations
Our study has some limitations. The retrospective, cross-sectional nature of the survey provided an examination at a point in time and did not assess well-being or stress prospectively at discriminate intervals. Our study examined self-reported measures and neither defined nor objectively assessed well-being, stress, or professional isolation; therefore, respondents might have interpreted these concepts differently. Respondents might have had a tendency to accentuate the positive and provide the socially desirable response for well-being or for stress management strategies, not wanting to convey ill health or socially undesirable ways of dealing with stress. For example, a few respondents indicated “drink exactly the right amount” as a means of handling stress. Physicians might also be comfortable with or used to a high level of stress; therefore, they might say that they have lower stress than they actually do, thereby actively masking their own stress levels. It is also possible that they might have overstated their health issues as a way of conveying that more initiatives are needed to address physician well-being issues. This study did not use a standardized tool to measure physician stress or well-being. Although the correlations between stress and well-being were in the expected direction, further validation work is required. Within the scope of our study, we were not able to assess the effect that stress or ill health had on the physician or on her or his clinical practice. We also do not know the effectiveness of the various stress-coping strategies employed. The 47.2% survey response rate is considered to be good for mailed surveys to physicians41; however, it is lower than the 62% to 72% we obtained from similar surveys of 1985 to 1995, 1996 to 2000, and 2001 to 2005 cohorts of family medicine graduates previously conducted. Those surveys did not include questions on well-being; therefore, comparison across the studies is not possible. Survey fatigue might also have contributed to the lower-than-expected response rate. Given the increasing interest in physician health, the questionnaire might have been more relevant to those with an interest in physician well-being. To test for nonresponse bias, we compared the proportion of respondents and nonrespondents on 2 variables (school and sex) and found no differences (P > .05); however, the 2 groups might have differed on other variables that we could not compare.
Conclusion
Although Alberta family medicine graduates report high levels of well-being, stress is an issue for many. Illness (family and personal) is a notable stressor and CMGs report higher levels of stress compared with their IMG colleagues. To manage stress, female physicians tend to communicate with colleagues and seek counseling more so than male physicians do. Studies on the effectiveness of stress management strategies should take into account such sex differences. International medical graduates and rural and urban physicians tend to rely on spiritual or religious practices and stress management programs should be cognizant of this. Nearly one-fifth of family physicians report professional isolation; this does not appear to vary according to practice type or location. Research on the prevalence of professional isolation in urban settings, regardless of practice type, along with identifying the factors that contribute to professional isolation, appears warranted. In light of considerable variation in stress coping strategies, programs aimed at facilitating physician well-being should be multifaceted in order to support a range of physician preferences.
Acknowledgments
Funding for this project was provided by The Alberta Rural Physician Action Plan.
Notes
EDITOR’S KEY POINTS
Recent Alberta family medicine graduates are primarily healthy and have a strong sense of personal and professional well-being. This is reassuring for the health care system given that good health has a positive influence on physician supply and productivity.
Almost 40% of family medicine graduates in this study reported experiencing high to extremely high levels of stress from various sources. Strategies for managing stress typically included social contact with family, friends, or colleagues. Physician support programs or informal wellness initiatives within practice settings should include elements of social contact and support groups.
This study found that 18.4% (almost 1 in 5) of family medicine graduates felt moderately to extremely professionally isolated. Professional isolation was also found to be positively correlated with stress. Because family physicians often work one-on-one with their patients, this might result in decreased interaction with colleagues, creating feelings of isolation. Strategies aimed at reducing professional isolation can include attending continuing professional development activities or introducing initiatives to increase social contact among family physicians and other health professional team members.
POINTS DE REPÈRE DU RÉDACTEUR
Les diplômés récents en médecine familiale sont généralement en bonne santé et ils éprouvent un fort sentiment de bien-être personnel et professionnel. Cela est rassurant pour le système de santé étant donné qu’une bonne santé favorise la disponibilité et la productivité des médecins.
Dans cette étude, près de 40 % des diplômés en médecine familiale déclaraient subir un stress très ou extrêmement élevé, et ce, pour diverses raisons. Les stratégies généralement utilisées pour gérer ce stress comprenaient des contacts avec la famille, les amis ou les collègues. Les programmes de soutien aux médecins ou les initiatives informelles instaurées dans le milieu de pratique devraient inclure des contacts sociaux et des groupes de soutien.
Cette étude a constaté que près de 1 diplômé en médecine familiale sur 5 (18,4 %) se sentait modérément à extrêmement isolé sur le plan professionnel. L’étude a montré que ce sentiment est en corrélation directe avec le stress. Le fait que le médecin de famille travaille souvent seul avec son patient pourrait réduire les interactions avec les collègues et susciter un sentiment d’isolement. Parmi les stratégies visant à réduire cet isolement, mentionnons la participation à des activités de formation médicale continue ou la création d’un plus grand nombre d’occasions de contacts sociaux entre les médecins de famille et les autres professionnels de la santé membres de l’équipe.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
Ms Szafran contributed to the concept and implementation of the study, data analysis, and interpretation of the study findings, and drafted the manuscript. Dr Woloschuk contributed to the concept of the study, data analysis, interpretation of the study findings, and critically reviewing the manuscript. Dr Torti was involved in the implementation of the survey, data entry, interpretation of the study findings, and critically reviewing the manuscript. Dr Myhre contributed to the concept and interpretation of the study findings and critically reviewing the manuscript.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.