


Abstract
Objective To describe the prevalence and geographic distribution of cervical cancer screening, as well as the age groups of those undergoing screening, in Alberta, and to determine if screening practices conform to current guidelines and follow Choosing Wisely Canada recommendations.
Design Descriptive study using data from the Alberta Ministry of Health Analytics and Performance Reporting Branch.
Setting Alberta.
Participants Women who had 1 or more Papanicolaou tests between 2011 and 2013.
Main outcome measures Number of women aged 15 to 20 and those aged 70 and older who had 1 or more Pap tests in a 3-year period; year-to-year trends in screening rates for women in these 2 age groups; trends in screening rates in various geographic regions (ie, cities and zones) in Alberta; and the discipline of clinicians who ordered the Pap tests.
Results Between 2011 and 2013, 805 632 women in the province of Alberta had 1 or more Pap tests for cervical cancer screening. Overall, 25 511 (17.5%) women aged 15 to 20 and 16 818 (10.3%) aged 70 and older were screened contrary to most existing guidelines. Screening rates varied markedly in different geographic regions of the province. Most Pap tests were ordered by family physicians or general practitioners.
Conclusion Within the geographic regions of Alberta, provincial, national, and international guidelines for screening with Pap tests are inconsistently followed. This strongly echoes the need for clinicians and patients to consider the Choosing Wisely Canada recommendations and current guidelines for cervical cancer screening.
The early identification and effective treatment of cervical cancer in women represents a considerable advancement in medical care during the 20th century. Papanicolaou testing (which collects a sample of cells from the cervix) has enabled this advancement and has become a routine part of preventive medicine. Unfortunately, inappropriate screening with Pap tests in women at very low risk of cervical cancer might result in more harm than benefit. Cervical cancer is rare before the age of 20, with no considerable rise in the incidence until age 25 or 30. Pap tests can cause local symptoms and anxiety, and might also reveal false-positive results that might obligate clinicians to suggest more invasive procedures, which might be associated with morbidity in both parous and nonpregnant women, including bleeding, infection, and premature delivery.
Choosing Wisely is a campaign that was started in the United States in 2012 by the American Board of Internal Medicine; it was designed to spark conversations between patients and physicians about the overuse of tests and procedures. Partnering with Consumer Reports in the United States, patient-friendly pamphlets and Web pages were created to help explain not only the rationale for not needing a particular test or procedure but also to present alternate strategies and resources that could help solve the problem at hand. In April 2014, Choosing Wisely Canada (CWC) followed this path by releasing its first set of 41 recommendations from 8 societies. There are now more than 180 recommendations by more than 30 societies. The uptake and effect of these recommendations remains to be seen. While most of the recommendations are well referenced and have been generally accepted to be reasonable by physicians, the scope and incidence of the identified problems on the CWC lists that might require change in Canada have not yet been well defined. In this article, we describe the results of our aggregate analysis of the prevalence and geographic distribution of cervical cancer screening, as well as the age groups of those undergoing screening, in Alberta. Three national physician organizations (Canadian Medical Association Forum on General and Family Practice Issues, the College of Family Physicians of Canada, and the Canadian Association of Pathologists) supported the following CWC family medicine recommendation: “Don’t routinely screen women with Pap smears if under 21 years of age or over 69 years of age.”1 Our analysis was carried out to see if this age-for-screening recommendation was being followed in Alberta.
METHODS
The Analytics and Performance Reporting Branch of the Alberta Ministry of Health is a multidisciplinary team of analysts with access to population-based data on physician billing claims for medical services and procedures for the province of Alberta for the purpose of providing high-quality evidence to inform and evaluate health policies.
We queried the Alberta Health Analytics and Performance Reporting Branch to obtain the discrete number of female patients who had 1 or more Pap tests between 2011 and 2013. Each patient was only counted once, no matter how many Pap tests she had had. Our analysis concentrated on 2 age groups: those aged 15 to 20 and those aged 70 and older. We then used the mid-year population of 2012 from the Alberta Health Interactive Health Data Application as our denominator for each age group of interest to develop a screening rate. The screening rate was calculated for the whole province and then separated into 5 geographic regions (ie, cities and zones) in Alberta: Calgary, Edmonton, and the Central, South, and North zones. We then analyzed year-to-year trends for screening rates for each of the 2 age groups of interest, compared with women aged 21 to 69 years. As the denominator, we used year-specific mid-year population data for each of 2011, 2012, and 2013. Differences in screening rates by year and by geographic region for each age group were examined using a Poisson regression model and described using 95% CIs estimated from the model. Owing to the large sample size, all differences by year and geographic region were highly statistically significant. Therefore, estimates of rates and rate reduction by year were provided with 95% CIs. We used data available only from 2014 to illustrate the proportion of Pap tests performed by family physicians compared with obstetricians or gynecologists.
Ethics approval was received from the University of Calgary Conjoint Health Research Ethics Board. This study is based in part on data provided by Alberta Health. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta. Neither the Government of Alberta nor Alberta Health express any opinion in relation to this study.
RESULTS
From 2011 to 2013, 805 632 women in the province of Alberta had 1 or more Pap tests for cervical cancer screening. When we evaluated young women aged 15 to 20 (female population in mid 2012 was 145 703) over this time frame, we found that 25 511 (17.5%) underwent screening with 1 or more Pap tests despite most existing guidelines suggesting against testing for this group. For women aged 70 and older (female population in mid 2012 was 162 782), we found a similar pattern of testing, with 16 818 (10.3%) having 1 or more Pap tests between 2011 and 2013— which, again, is contrary to recent guidelines (Table 1).
Percentage of women in the province of Alberta undergoing cervical cancer screening with 1 or more Papanicolaou tests over a 3-year period (2011 to 2013)
Statistically significant differences in screening rates compared with the provincial average were observed for each age group (P < .001) and each geographic region (P < .001), as shown in Figure 1. For the 15-to-20 age group, screening rates were lowest in Calgary (14.1%) and the South zone (16.4%), moderate in the Central zone (19.5%) and Edmonton (18.1%), and highest in the North zone (23.7%). None of these CIs overlapped, suggesting a statistically significant difference between each geographic region. For the 70-and-older age group, rates were lowest in the South zone (5.9%), moderate in Calgary (9.7%) and the Central (8.4%) and North (9.0%) zones, and highest in Edmonton (13.4%). The CIs did not overlap in the South zone and Edmonton, suggesting statistically significant differences between both these regions and all others (Figure 1).

Cervical cancer screening rate throughout several geographic areas in Alberta for women aged 15 to 20 and those aged 70 and older over a 3-year period, with 95% CIs: The red horizontal line is the provincial average.
We then looked at screening rate trends in patients aged 15 to 20 years and those aged 70 and older for each of the calendar years from 2011 to 2013 (Figure 2 and Table 2). There was a statistically significant decrease in screening rates by year for both age groups (P < .001 for both). This decline is much sharper for the younger age group compared with the older women.
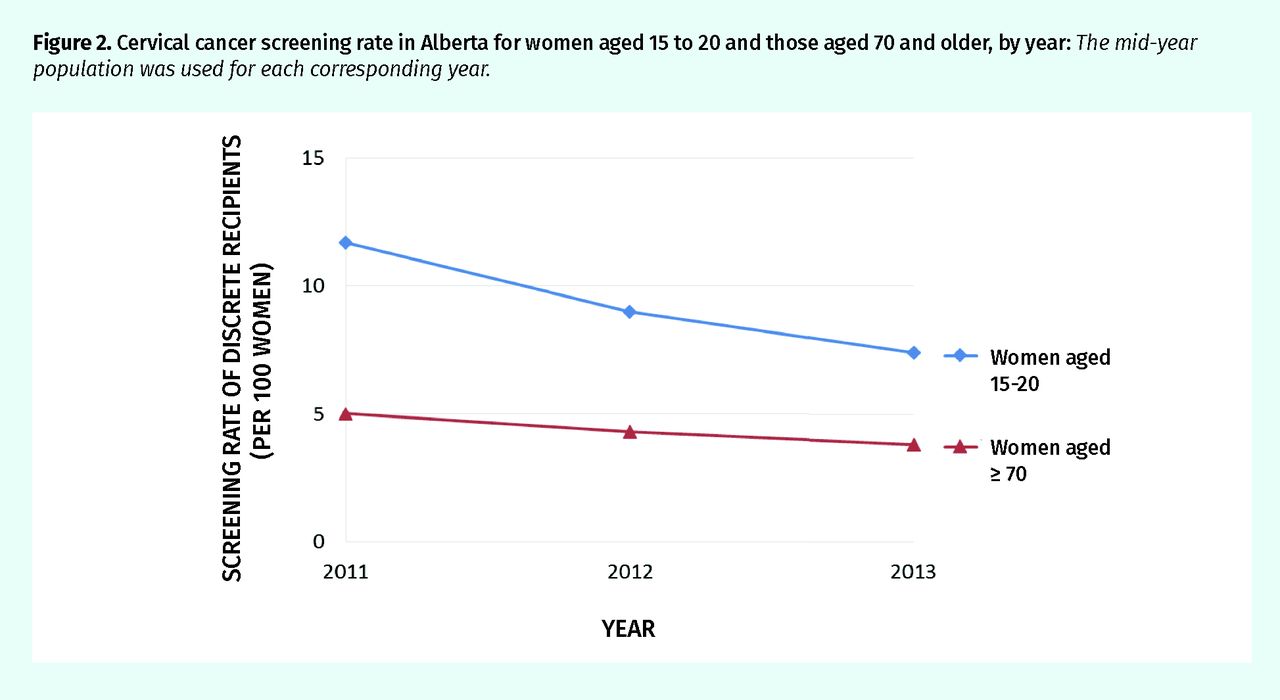
Cervical cancer screening rate in Alberta for women aged 15 to 20 and those aged 70 and older, by year: The mid-year population was used for each corresponding year.
Number of discrete women screened per 100 women during 2011 to 2013
As shown in Table 3, in all age groups, most Pap tests in 2014 were ordered by family physicians or general practitioners, whereas obstetricians, gynecologists, or others ordered the tests for a much smaller number of women.
Women in each age group undergoing Papanicolaou tests in 2014 by discipline of the ordering physician
DISCUSSION
Cervical cancer is the third most commonly diagnosed cancer and the fourth leading cause of cancer death in women worldwide.2 In Canada, cervical cancer is the 13th most commonly diagnosed cancer and the 16th leading cause of cancer death.3 The age-standardized incidence rates fell by an average of 2.2% between 1992 and 2005 in Canada with a stabilization of rates ever since.3 Over the past 60 years in the United States, mortality has been reduced by 70% owing in large part to the highly successful cervical screening program.4
Cervical cancer is rare before the age of 20 with no substantial rise in the incidence until age 25 or 30. Half of all cases of cervical cancer are diagnosed in women who either have never screened before or were last screened more than 5 years previously.5,6 Recently, Canadian researchers found no association between cervical cancer screening and the risk of death from cervical cancer in women younger than 30 years of age.7,8 Indeed in Holland, it is now recommended that women need not start screening until the age of 30.
Harm from inappropriate cervical screening can include vaginal bleeding, pain, anxiety, and infection. False-positive test results might lead to more invasive procedures that have been associated with bleeding, infection, and an increased risk of premature delivery.9–12 Furthermore, the identification of subclinical cervical lesions that might not progress can result in both physical and emotional consequences. Finally, screening is expensive: a 2012 US study reported that the cost estimate for cervical cancer screening and follow-up alone was $6.6 billion.13
Pap test recommendations have changed over time. Clinicians are understandably confused by the heterogeneity of guidelines in reference to both the appropriate age to commence testing and the evidence that informs screening intervals. Work from Canada as early as 1975 questioned the usefulness of annual screening.14 Research by investigators over the past 20 years has called this practice into question.15
In 2012, 2 sets of guidelines were released by the American Cancer Society conjointly with 2 other associated societies and by the US Preventive Services Task Force that for the most part harmonize recommendations for cervical cancer screening.6,16 Furthermore, the National Comprehensive Cancer Network endorsed the guidelines from the American Cancer Society and elected to discontinue its own guidelines. These documents recommend that women begin cervical cancer screening at age 21 and continue every 3 years until the age of 65. Women who have been vaccinated against human papillomavirus should follow the same schedule as their unvaccinated peers.
In Canada, the delivery of health care at the provincial government level has led to a heterogeneous approach to cervical cancer screening and guidelines. Despite this, the participation rate for cervical cancer screening is generally high, ranging from 63% to 71% between 2010 and 2013; however, it falls short of the 85% target set by the Canadian Partnership Against Cancer (CPAC).17
Alberta released guidelines in 2011 advising screening in women between the ages of 21 and 69.18 In 2013, the Canadian Task Force on Preventive Health Care published its cervical cancer screening recommendations. Screening with Pap tests is suggested every 3 years for all women between the ages of 25 and 69 while acknowledging that the supporting evidence in screening women between the ages of 20 and 29 is weak.19
Despite these now mostly unified recommendations, many patients continue to get annual screening and commence testing at ages earlier than is warranted.15 The CPAC recently released a report suggesting that 49% to 90% of women aged 18 to 20 years had at least 1 Pap test between 2010 and 2013.17 Our data show that these cervical screening practices also persist in Alberta. Most Pap tests conducted in the province were performed by primary care physicians.
Our data from the current study suggest that provincial, national, and international guidelines might be inconsistently followed in practice. This strongly echoes the need for clinicians and patients to consider the CWC recommendations about cervical cancer screening. Survey data from the United States in a large health maintenance organization reported poor adherence to the 2012 cervical cancer screening guidelines, suggesting our data might reflect practice in other jurisdictions, at least in North America.20
For women outside of the currently recommended target age groups for cervical cancer screening, we do note a statistically significant decrease in the screening rate between 2011 and 2013, particularly in young women aged 15 to 20 years. This suggests that some of the new guidelines and educational initiatives might be influencing practice change. Finally, we do see quite marked regional differences in cervical cancer screening practices within Alberta, suggesting the need for a unified provincial initiative to seek out and address barriers to change in practice that might be unique to some parts of the province. Recent Canadian data suggest that cervical screening practices in Alberta might be similar to those across our country.17
Strengths and limitations
Limitations to our study relate mostly to the limitations encountered when querying any large administrative database. These include reliability of physician coding for procedures, billing, and diagnostic codes; incomplete or missing records that might not be obvious to data analysts; and our inability to mine true clinical indications for tests. The use of mid-2012 Alberta population data might overestimate the proportion of women screened in 2011, but this might be counterbalanced by a possible underestimation of the screening rate for 2013. Regional Pap test screening rate differences might be influenced by intraprovincial mobility for which we cannot account. A final but important limitation is that we are unable to assess from administrative data whether there might truly have been a strong clinical indication for the screening test at the extremes of ages. The absence of direct clinical data prevents us from identifying older women who have never been screened previously, those with previous abnormal Pap test results, immunocompromised women, and those women who were exposed in utero to diethylstilbestrol. The CPAC reports that 30% of all women in appropriate age categories are still not screened for cervical cancer and this report should in no way distract clinicians from the benefits of screening these patients.17
The main strengths of our study include the high number of cervical cancer screening tests, the capture of most if not all Pap tests during this time frame and the 2011 publication of Alberta provincial guidelines18 about this practice that coincides with our first year of analysis. Our data also suggest that some clinicians are early adopters of the 2011 guidelines. Hopefully this trend for more age-appropriate screening will continue. This report also allows physicians to reflect upon regional differences in clinical practice within the province that might have broader ramifications for system-based interventions and continuing professional development.
Conclusion
Cervical cancer screening with Pap tests is a valuable and potentially lifesaving tool. However, its broad application to women at very low risk of cervical cancer might result in both harm and unnecessary expenditure of valuable health care resources. Local Canadian data from Alberta suggest that there is ongoing inappropriate screening of younger and older women at very low risk; however, this practice seems to be improving over time. This study also shows that there are substantial regional variations in screening rates throughout the province. Our analysis supports the implementation of the CWC Pap test age-for-screening recommendation and updated cervical cancer screening guidelines.1 We hope this study might provide the impetus for further evaluation of cervical cancer screening practices and identification of barriers to change.
Acknowledgments
We thank Larry Svenson and his team at the Analytics and Performance Reporting Branch of the Alberta Ministry of Health for their contributions.
Notes
Editor’s key points
▸ One of the Choosing Wisely Canada recommendations is to not screen women with Papanicolaou tests if they are younger than age 21 or older than age 69. This article describes the geographic distribution of cervical cancer screening, as well as the age groups of those undergoing screening, in Alberta. The analysis was conducted to determine if this age-for-screening recommendation was being followed in Alberta.
▸ This study found a statistically significant decrease in the screening rate between 2011 and 2013 for women in Alberta outside of the currently recommended target age groups, particularly in young women aged 15 to 20 years. This suggests that some of the new guidelines and educational initiatives might be influencing practice change.
▸ There were regional differences in cervical cancer screening practices within Alberta, suggesting the need for a unified provincial initiative to seek out and address barriers to change in practice that might be unique to some parts of the province.
Points de repère du rédacteur
▸ Une des recommandations de Choisir avec soin au Canada est d’utiliser le Pap test uniquement chez les femmes de moins de 21 ans ou de plus de 69 ans. Cet article décrit la distribution géographique de cet examen pour dépister le cancer du col utérin ainsi que les groupes d’âge de celles à qui on prescrit cet examen en Alberta. Les résultats ont été analysés afin de déterminer si les recommandations concernant l’âge des patientes étaient respectées en Alberta.
▸ L’étude a observé qu’entre 2011 et 2013, il y avait eu une diminution statistiquement significative du taux de dépistage chez les Albertaines qui n’appartenaient pas aux groupes d’âge recommandés, et ce, particulièrement chez les femmes entre 15 et 20 ans. Cela suggère que certaines des récentes recommandations et séances de formation pourraient avoir entraîné des changements dans la pratique.
▸ Il y avait des différences régionales dans la façon de prescrire le dépistage du cancer du col utérin en Alberta, ce qui suggère qu’il faudrait une intervention provinciale unifiée pour déterminer ce qui empêche les médecins de certaines parties de la province de modifier leur pratique.
Footnotes
Contributors
Dr Symonds prepared the manuscript and background literature search. Ms Chen managed the project and performed data analysis. Dr Rose performed the statistical analysis. Dr Cooke reviewed and approved the data, analysis of the data, and data conclusions. All authors read and approved the final version of this manuscript.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}