


Abstract
Objective To present a practical and evidence-based approach for primary care physicians to the diagnosis and initial management of common pediatric hand injuries, and to identify injuries requiring prompt referral.
Sources of information Clinical evidence and expert recommendations were identified by using MEDLINE and EMBASE for each topic presented.
Main message Pediatric hand injuries are a common reason for physician consultation. The most common and potentially problematic pediatric hand injuries include fingertip injuries, phalangeal fractures, tendon injuries, and hand burns. Management is limited by difficulties in proper assessment of the hand and the paucity of evidence to guide treatment. Nevertheless, outcomes in children are typically excellent.
Conclusion Appropriate assessment, initial management, and, if necessary, timely referral of pediatric patients with hand injuries are paramount given the importance of the hand in function and child development. While some principles from managing adult hand injuries might apply, children often require special considerations.
Injuries to the hand are common in the pediatric population.1 They are a frequent reason for presentation to urgent care clinics and emergency departments; hand fractures account for about 15% of all pediatric fractures and 2.3% of pediatric emergency visits.2,3 Hand injuries can be particularly challenging in the pediatric population, as the history and physical examination might be limited. While some principles from managing adult hand trauma can be applied, injury patterns and management might differ owing to differences in mechanism of injury, the presence of open physes, and patient compliance. Delays in appropriate treatment might carry a considerable risk of long-term morbidity, and the time window for intervention is often shorter in children compared with adults.4 Consequently, accurate assessment, appropriate initial care, and timely referral, if necessary, are paramount to optimize outcomes.
Case description
An otherwise healthy 10-year-old boy is brought to the emergency department by his mother with a painful, bleeding right ring finger after it was stepped on while playing football. On examination, the distal fingertip is bleeding with avulsion of the proximal nail plate from the eponychial fold (Figure 1A). The fingertip is flexed and does not straighten (Figure 1B). Examination is limited. Lateral radiographs demonstrate physeal separation in the distal phalanx with apex dorsal angulation (Figure 1C).

Ten-year-old boy’s right ring finger after it was stepped on while playing football: A) Fingertip injury with avulsion of the proximal nail plate from the eponychial fold; B) fingertip appears flexed and does not actively straighten; and C) lateral radiograph demonstrating physeal separation in the distal phalanx with apex dorsal angulation.
Sources of information
Searches of MEDLINE and EMBASE were conducted to identify literature relevant to each topic presented using the following terms (EMTREE subject heading or MeSH terms were used when available): pediatric hand injuries, pediatric hand fractures, subungual hematomas, nail bed lacerations, mallet finger, central slip avulsion, jersey finger, and pediatric hand burns. Recommendations presented are based on clinical evidence and expert opinion and are graded from levels I to III. Level I evidence is based on data from randomized controlled trials, systematic reviews, or meta-analyses; level II on data from other comparison trials such as non-randomized cohort studies; and level III on expert opinions.
Main message
The clinical approach to examining the pediatric hand is outlined here. We also propose strategies to help you assess hand injuries in children.
History taking.
A hand history follows the general structure of a regular pediatric medical history. It is imperative to obtain an accurate history (sometimes by proxy) of the mechanism of injury including the environment in which the injury was sustained. Associated symptoms might provide clues as to the presence of additional soft tissue damage. For example, paresthesias or weakness might indicate nerve damage. The child’s hand dominance should be documented; it normally develops around age 3.5 Information about the child’s activities, sports, music, and career goals might be relevant in older children. Tetanus status should be elicited and updated if necessary. A developmental history and a history of previous hand injuries should be garnered to better guide the physical examination and treatment goals. The possibility of nonaccidental injury should always be entertained.
Physical examination.
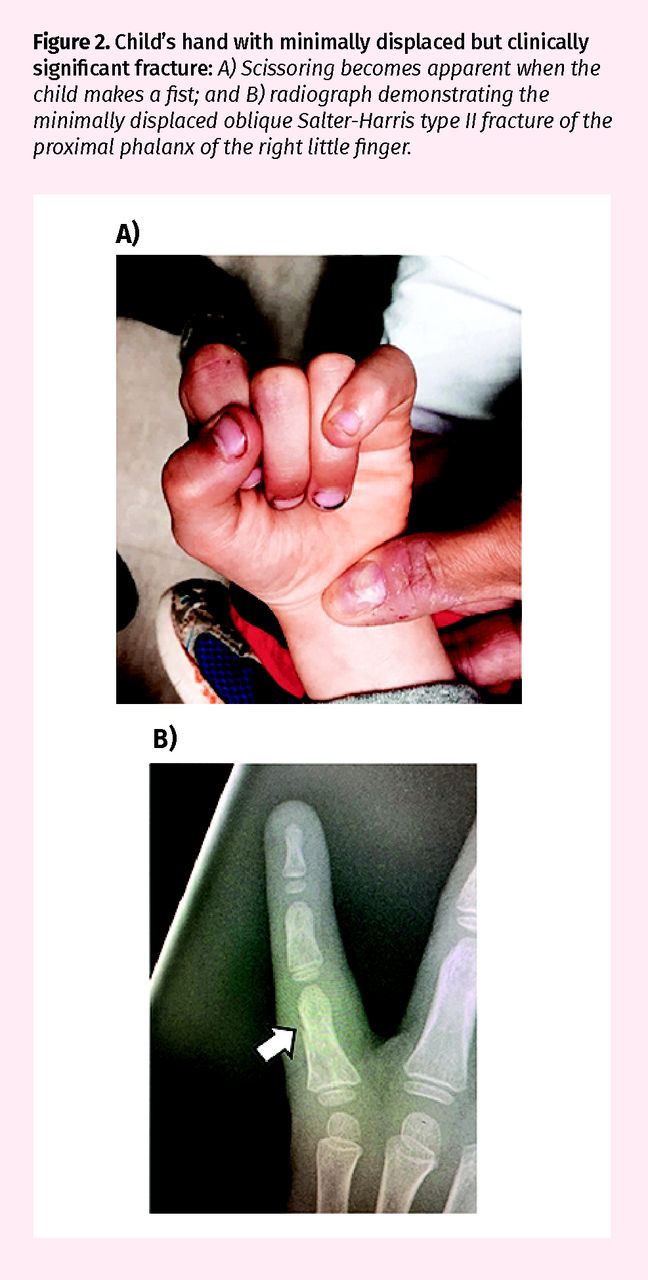
Examination of the hand is similar to that for adult patients, with modifications depending on the child’s age and willingness or ability to cooperate.6,7 Observation of the child’s hand at rest and play can elucidate sources of pain, the presence of underlying fractures, and evidence of tendon or nerve injuries. Bruising, swelling, and systematic palpation of the hand might help localize underlying fractures or ligamentous injuries. Minimally displaced fractures might be clinically significant if they result in scissoring; this might not become apparent until the child makes a fist (Figure 2). Certain familiar gestures such as high fives and fist bumps allow the physician to test the active range of motion in children not capable of following directions. Occasionally, the administration of local anesthetic is required to properly assess for range of motion and scissoring. Wrist tenodesis might also be a useful physical examination tool to determine tendon continuity, independent of nerve or muscle function. With intact tendons and a relaxed or distracted patient, passive extension and flexion of the wrist will result in compensatory finger flexion and extension, respectively. Vascularity can be assessed by colour, temperature, and capillary refill. Anhidrosis and lack of skin wrinkling with submersion in water over a certain nerve distribution suggests damage to that nerve in children incapable of communicating sensation (Figure 3).

Child’s hand with minimally displaced but clinically significant fracture: A) Scissoring becomes apparent when the child makes a fist; and B) radiograph demonstrating the minimally displaced oblique Salter-Harris type II fracture of the proximal phalanx of the right little finger.

Anhidrosis and lack of skin wrinkling of the little finger and ulnar half of the ring finger (dash outline) in keeping with an ulnar nerve injury
Initial investigations.
X-ray imaging is required if a fracture or dislocation is suspected. An ultrasound might be useful to confirm tendon injury.8
Referral.
The time window for intervention might be shorter in children than adults owing to faster healing times.4 Certain fractures (open, displaced, angulated, rotated, intra-articular, or unstable) and nerve and tendon injuries typically require a telephone call to a hand surgeon at the time of presentation.
Differential diagnosis
Fingertip injuries.
Fingertip crush injuries, usually by a car or house door, are a common pediatric hand injury.9 An assortment of injuries, as presented below, might ensue. Nearly half involve an underlying fracture of the tuft of the distal phalanx.9
Subungual hematomas, nail bed lacerations, and tuft fractures: The optimal management of subungual hematomas, nail bed lacerations, and open tuft fractures remains controversial. Options include observation, trephination, and open repair. Trephination involves hematoma evacuation through a hole in the nail plate created by electrocautery, a heated paper clip, or a needle (18-gauge).10 Open repair involves removal of the nail plate and repair of the nail bed under local anesthesia with absorbable sutures or 2-octylcyanoacrylate (“skin glue”).11 Epinephrine is safe to add in digital blocks for control of bleeding and exploration of deep lacerations.12 The removed nail plate can be reinserted under the nail fold to keep it open and protect the repair; however, this is currently under investigation.13,14 If there is an underlying fracture, a fingertip splint with the proximal interphalangeal joint (PIPJ) free is usually sufficient depending on the age of the child (Figure 4). Prophylactic antibiotics (typically 5 days of oral cephalexin) are only indicated following repair of grossly contaminated injuries (level I evidence).15,16
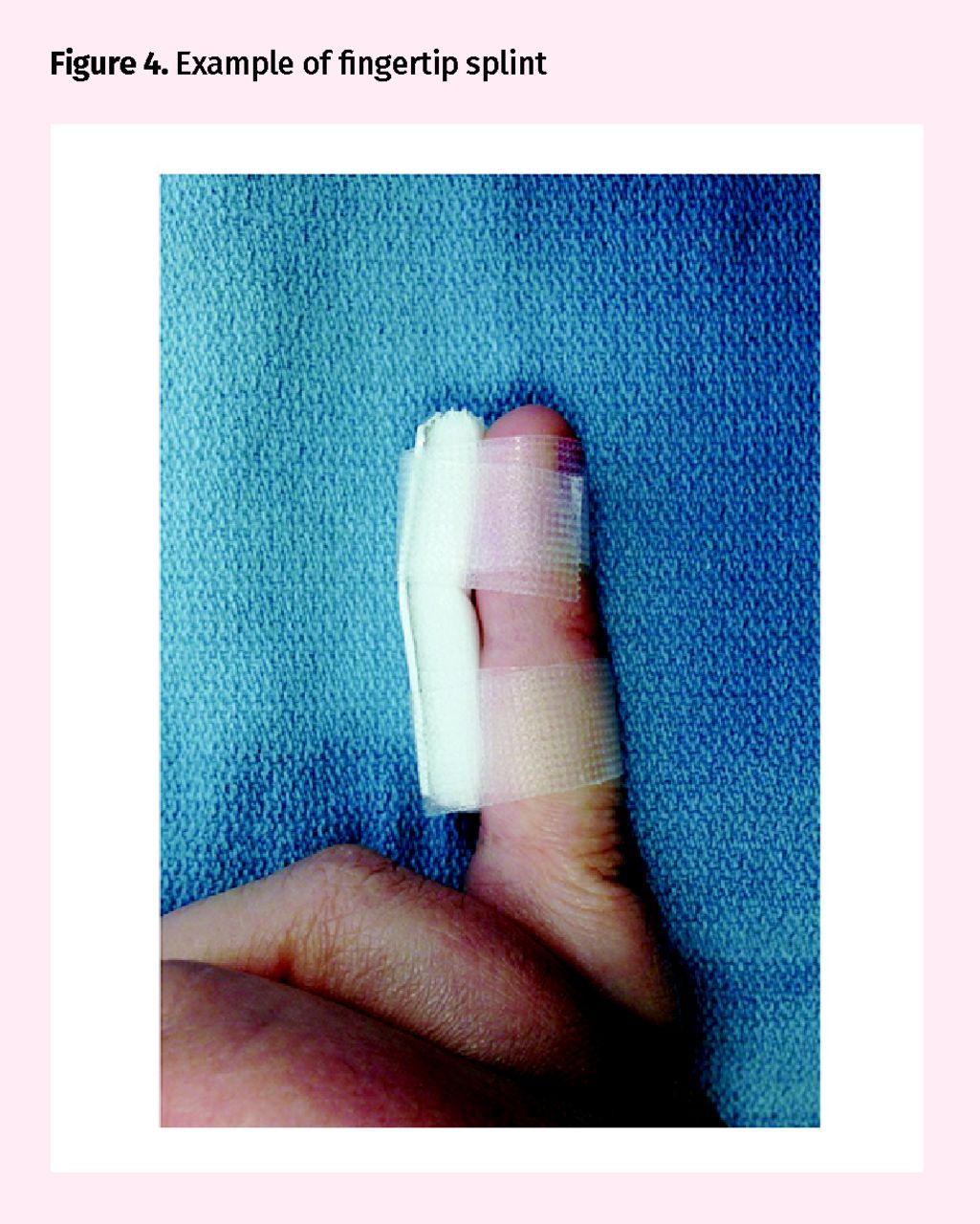
Example of fingertip splint
Generally, it is accepted that if the nail plate or fold is disrupted or if there is a displaced tuft fracture, the nail should be removed and the nail bed repaired (level III evidence).9,17 For an intact nail and nondisplaced fracture, controversy exists. Some authors have advocated guiding treatment based on the size of the hematoma.18,19 However, some studies have demonstrated that no matter the size of the hematoma or even the presence of a nondisplaced fracture, favourable results can be obtained with trephination or expectant management alone (level II evidence).9,20–22
Seymour fractures: A Seymour fracture is an injury unique to children and requires prompt attention. Following crush injury or axial load, an angulated Salter-Harris type I or II fracture of the distal phalanx with an associated nail bed injury might result. The nail plate is typically avulsed proximally from the nail fold, and soft tissue (often the germinal matrix of the nail) might become interposed in the fracture preventing reduction and healing. The typical presentation is a swollen, ecchymosed, and painful finger, flexed at the distal interphalangeal joint (DIPJ). Lateral view x-ray scans confirm the diagnosis. If untreated, osteomyelitis, malunion, and premature closure of the physis might occur.23 Injuries can be treated with closed or open reduction followed by 2 to 4 weeks of splinting (level II evidence).24–26 More substantive injuries require open reduction and nail bed repair. Surgical fixation with Kirschner wires (or K-wires) is rarely required.
Distal digit amputations: The most commonly amputated body part in a child is a fingertip.27 Amputations distal to the DIPJ can be treated with reattachment of the amputated fingertip as a composite graft, healing by secondary intention, or revision amputation.28
Replantation in children is generally limited owing to the distal level and the usual crush nature of the injury. Further, outcomes with conservative therapy are typically excellent especially with amputations distal to the germinal matrix.29 Conservative therapy consists of wound healing by secondary intention with standard wound care including daily cleansing and nonadherent dressings. However, if there is any possibility of replantation, consultation with a hand surgeon should be sought immediately.
Fractures.
Approximately one-fifth of hand injuries in children are fractures.1 Nondisplaced fractures are generally treated with immobilization; however, patient age might dictate the type and duration of immobilization. Figure 5 presents examples of common immobilization techniques. If displaced, closed reduction is performed. Potentially unstable fractures should have close follow-up to ensure reduction is maintained. Fractures that fail closed reduction might require surgical management. Open fractures require irrigation, debridement, antibiotic treatment, and surgical referral.

Examples of common immobilization techniques for hand injuries: A) Thumb spica splint, B) ulnar gutter splint, C) volar resting splint, and D) above-elbow cast (young children might require an above-elbow cast to minimize the risk of accidental slippage or removal).
Differences between the pediatric and adult hand contribute to different injury patterns and considerations in management. Open physes are a point of inherent weakness, and injury might result in premature closure and abnormal growth. However, open physes also offer the possibility for digit remodeling following injury. Physeal fractures are classified by the Salter-Harris classification (Figure 6). Children also have a robust periosteum resulting in improved fracture stability and faster healing.30
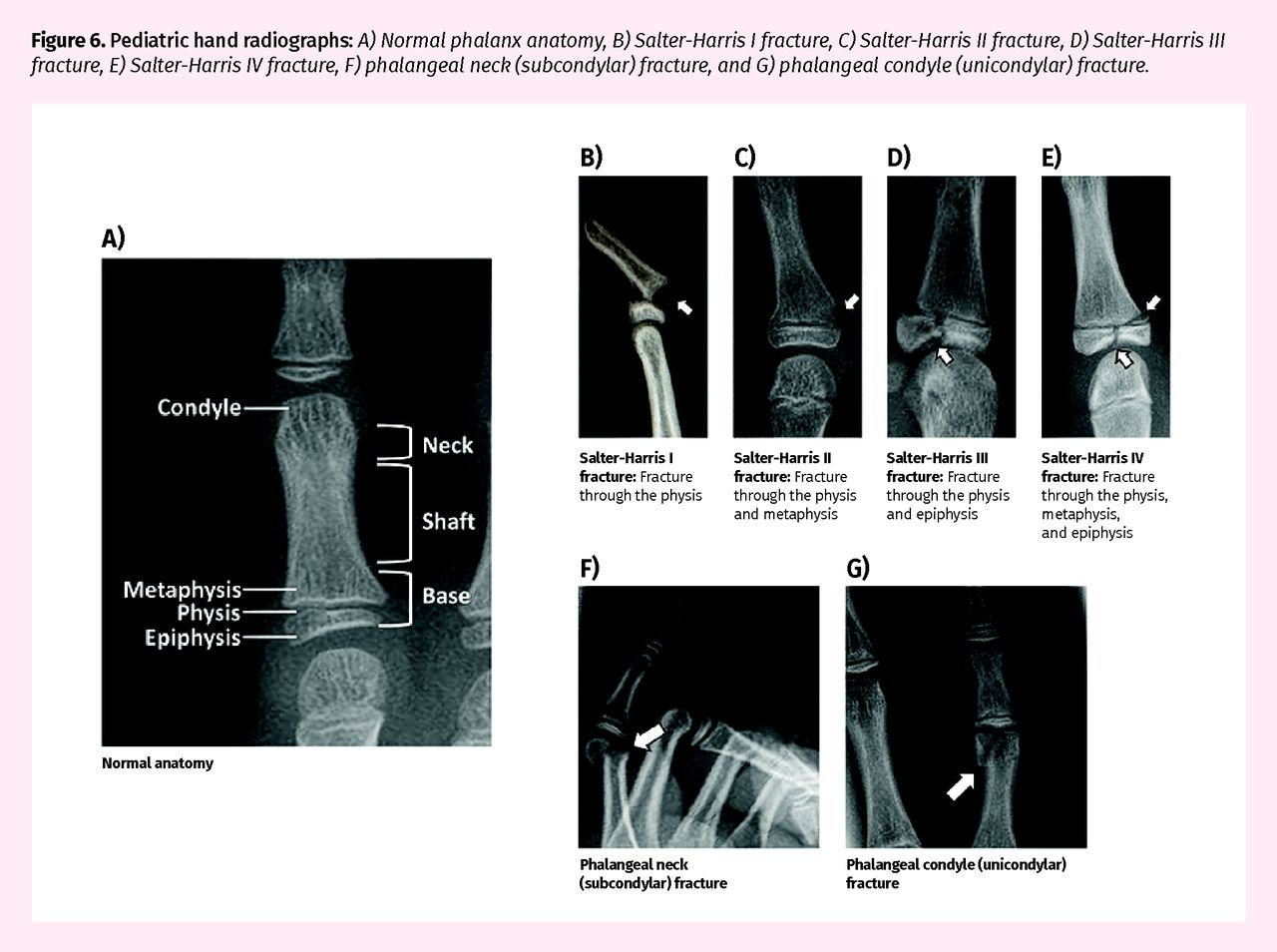
Pediatric hand radiographs: A) Normal phalanx anatomy, B) Salter-Harris I fracture, C) Salter-Harris II fracture, D) Salter-Harris III fracture, E) Salter-Harris IV fracture, F) phalangeal neck (subcondylar) fracture, and G) phalangeal condyle (unicondylar) fracture.
However, a shorter time window for fractures requiring intervention might exist.4 Fractures requiring special consideration or seen more commonly in children are presented below.
Phalangeal base fractures: Phalangeal base fractures are the most common pediatric hand fracture pattern. The proximity of the physis assures a high degree of remodeling (Figures 6A and 6C), thus closed reduction followed by 3 to 4 weeks of immobilization suffices for most of these fractures (level II evidence).31 Severely displaced or unstable fractures might require surgical intervention. A common pitfall that might contribute to difficulty or inability to obtain a closed reduction is failure to recognize the location of the fracture in relation to the surface anatomy of the hand. The base of the proximal phalanx is considerably more proximal than the web space of the digit. Failure to properly anesthetize and stabilize the proximal aspect of the fracture might result in difficulty achieving an adequate reduction.
Phalangeal neck fractures: Neck fractures of the proximal and middle phalanges are classic pediatric injuries, rarely seen in adults.32 Most result from a crush injury to a finger caught in a closing door or window. Given the distance from the physis (Figures 6A and 6F), there is poor remodeling potential. Surgical consultation is recommended for any displaced neck fracture, as these are particularly unstable and require close follow-up (level II evidence).33–35
Otherwise, nondisplaced fractures respond well to 3 to 4 weeks of immobilization.34
Condylar fractures: The condyles are a pair of tuberosities that form the distal articular surfaces of the proximal and middle phalanges (Figure 6A). Condylar fractures are intra-articular in nature and often unstable (Figure 6G). Surgical consultation is recommended, as these fractures require meticulous reduction to ensure proper joint congruity (level III evidence).3,4
Tendon injuries.
Tendon injuries result in the loss of active but not passive range of motion. Observation of the hand and finger position at rest and with passive tenodesis of the wrist might give clues to suggest underlying tendon injury (Figure 7). Closed tendon injuries such as mallet fingers, central slip injuries, and jersey fingers should not be missed, and they might be associated with an avulsion fracture. Mallet fingers are extensor tendon injuries at the distal phalanx resulting from sudden flexion of an extended DIPJ. They present with a DIPJ flexion deformity (Figure 8). Central slip injuries are extensor tendon injuries at the middle phalanx resulting from forced flexion of an extended PIPJ. These 2 injuries are generally treated with uninterrupted splinting of the affected joint in extension for 6 weeks.36 Jersey fingers, which result from sudden hyperextension of a flexed DIPJ, present with inability to flex the DIPJ owing to flexor digitorum profundus avulsions at the distal phalanx. They require prompt referral for surgical management. Open tendon lacerations can be managed with initial wound care, skin closure, and temporary immobilization followed by surgical referral for definitive repair within 1 to 2 weeks (level III evidence).36,37 Nerve and vascular injuries should be considered with lacerations to the volar surface of the finger or hand.

Flexor tendon lacerations resulting in loss of natural cadence of long, ring, and little fingers at rest

Example of DIPJ flexion deformity
DIPJ—distal interphalangeal joint.
Dislocations.
In young patients, finger dislocations are relatively rare, as the ligamentous joint structures in children are stronger than immature developing bone.38 Following reduction, the injured finger is protected to prevent re-injury. Depending on the stability of the joint and patient compliance, the finger can be immobilized or buddy taped. Early range of motion and edema control should be considered. Dislocations that are irreducible require surgical consultation.
Burns.
The hand is frequently involved in burn injuries in children.39 Scald burns are more frequent in younger children while flame burns become more common with age.40 The hand dorsum is typically more vulnerable, but the volar surface is susceptible to contact burns during children’s exploration of household appliances such as fireplaces, stovetops, and hair irons.39,40 Initial management includes cooling of the burned area with cool water (or soaked gauze) for at least 20 minutes, cleansing, and pain management (level II evidence).41 Obviously necrotic debris and broken blisters should be debrided and the burn can then be dressed with the fingers separated. There is emerging evidence supporting the use of silver-impregnated and non-silver dressings; these novel dressings have been associated with decreased pain, fewer dressing changes, and lower overall costs when compared with traditional dressings with silver sulfadiazine (level I evidence).42–45 Circumferential burns causing vascular compromise requiring escharotomy are rare but should not be missed.46 Burn centre referral is recommended for all burns that involve the hands.47,48
Case resolution
The 10-year-old boy presents with a Salter-Harris type I Seymour fracture. His mother is informed of the risks of scarring, infection, malunion, nonunion, growth disturbance, and nail loss and irregularity. In the emergency department, a digital nerve block is administered for local anesthesia (in younger children, procedural sedation might also be considered). Fracture reduction requires reflection of the eponychial fold to expose the fracture and the interposed germinal matrix (Figure 9A). The fracture is then thoroughly irrigated, debrided, and reduced under direct vision. Postreduction x-ray scans are obtained (Figure 9B). The nail matrix and eponychial fold are repaired with fine absorbable sutures (sizes 5-0 and 6-0 plain gut sutures) (Figure 9C). A fingertip splint preventing DIPJ flexion but allowing PIPJ motion is applied (Figure 4). In younger children, a well secured volar forearm splint or above-elbow cast can be added to ensure proper immobilization (Figures 5C and 5D). A short course of oral antibiotics and follow-up in 1 to 2 weeks are arranged. At 4 weeks, the splint is discontinued and return to normal activity is permitted.
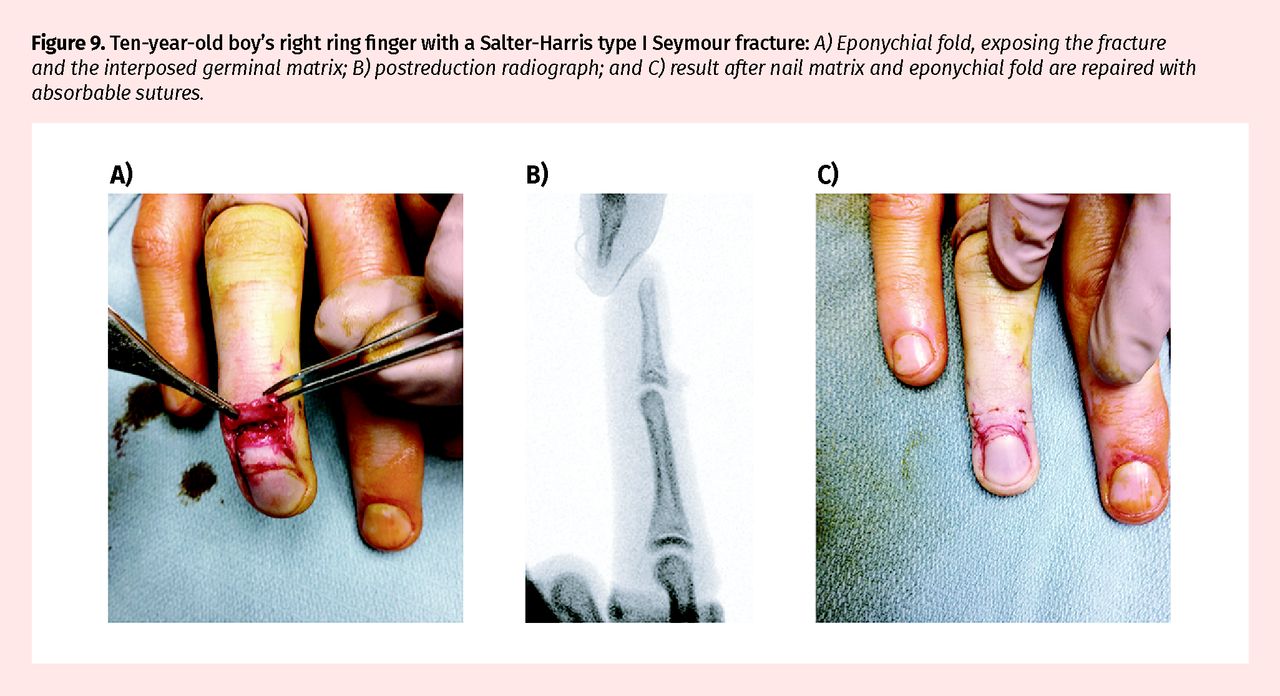
Ten-year-old boy’s right ring finger with a Salter-Harris type I Seymour fracture: A) Eponychial fold, exposing the fracture and the interposed germinal matrix; B) postreduction radiograph; and C) result after nail matrix and eponychial fold are repaired with absorbable sutures.
Conclusion
Management of pediatric hand injuries is limited by difficulties in proper assessment of the hand and the paucity of evidence to guide treatment. Nevertheless, outcomes in children are typically excellent.
Notes
Editor’s key points
▸ Assessment of hand injuries can be challenging in the pediatric population. Injury patterns and management might be different than for adult trauma owing to differences in mechanism of injury, the presence of open physes, and patient compliance.
▸ Delays in appropriate treatment might carry a risk of long-term morbidity. The window for intervention might be shorter in children compared with adults owing to faster rates of healing.
▸ A Seymour fracture is an injury unique to children and requires prompt attention. The typical presentation is a swollen, ecchymosed, and painful finger that is flexed distal to the distal interphalangeal joint. Lateral x-ray views confirm the diagnosis. Treatment includes closed or open reduction followed by 2 to 4 weeks of immobilization.
Points de repère du rédacteur
▸ L’évaluation d’une blessure à la main peut se révéler difficile dans la population pédiatrique. Les types de blessures et leur prise en charge peuvent différer de ceux des traumatismes chez l’adulte en raison des mécanismes différents des blessures, de la présence de plaques épiphysaires (de croissance) ouvertes et de l’observance du patient.
▸ Des retards dans l’administration d’un traitement approprié peuvent entraîner un risque de morbidité à long terme. Les délais d’intervention peuvent être plus courts chez l’enfant que chez l’adulte en raison de la plus grande rapidité de guérison.
▸ Une fracture de Seymour est une blessure exclusive aux enfants qui exige une attention rapide. Elle se présente habituellement sous la forme d’un doigt enflé, douloureux et porteur d’ecchymoses, qui est fléchi en position distale par rapport à l’articulation interphalangienne distale. Des clichés radiologiques latéraux confirment le diagnostic. Le traitement comporte une réduction fermée ou ouverte, suivie par 2 à 4 semaines d’immobilisation.
Footnotes
Contributors
Both authors contributed to the literature review and interpretation, and to preparing the manuscript for submission.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.