Article Text

Abstract
Aims: To examine the effect of the daily use of micronutrients (including zinc) or the same micronutrients plus heat inactivated lactic acid bacteria (LAB), on diarrhoea in children compared to placebo.
Methods: A triple blind randomised clinical trial in an urban slum of Karachi, Pakistan. Micronutrients (including zinc), micronutrients (including zinc and LAB), or placebo, were provided daily for two months to 75 young children (aged 6–12 months) identified at high risk for diarrhoea related mortality on the basis of history of at least one episode of diarrhoea in the preceding two weeks. The longitudinal prevalence of diarrhoea was defined as the percentage of days a child had diarrhoea out of the days the child was observed.
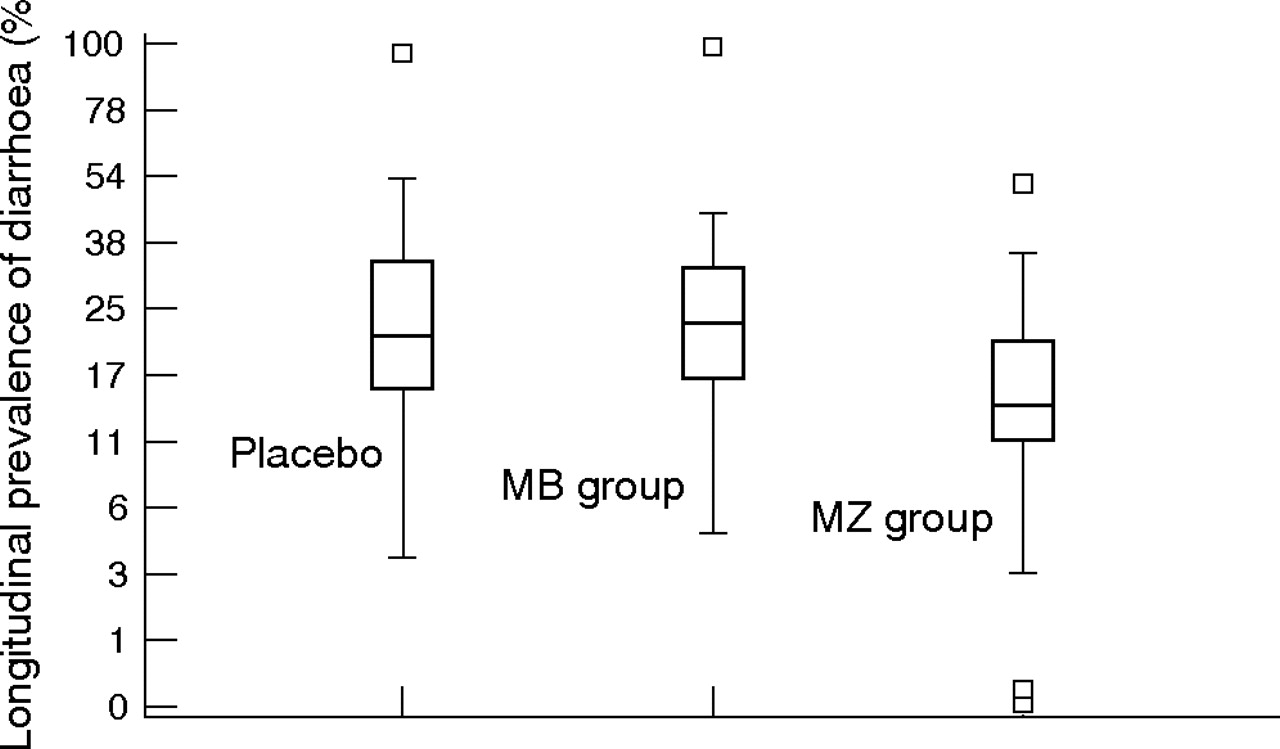
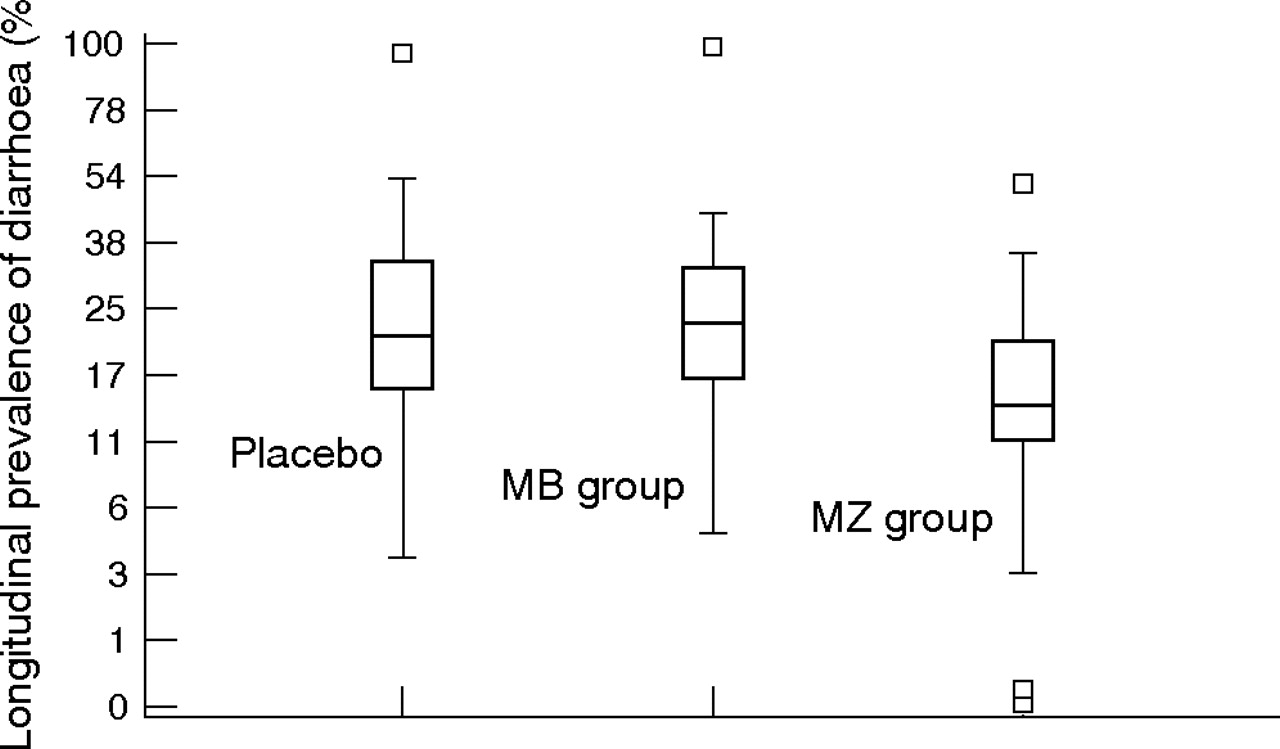
Results: Mean longitudinal prevalence of diarrhoea in the micronutrient–zinc group was 15% (SD = 10%) child-days compared to 26% (SD = 20%) child-days in the placebo group and 26% (SD = 19%) child-days in the micronutrient–zinc–LAB group. The difference between the micronutrient–zinc–LAB and placebo groups was not significant.
Conclusion: The daily provision of micronutrients (including zinc) reduces the longitudinal prevalence of diarrhoea and thus may also reduce diarrhoea related mortality in young children; heat inactivated LAB has negative effects in these children.
- AKU, Aga Khan University
- EPEC, enteropathic E coli
- ETEC, enterotoxic E coli
- HPF, high power field
- HSC, Hospital for Sick Children
- LAB, lactic acid bacteria
- MB, micronutrients which included LAB
- MZ, micronutrients which included zinc
- ORT, oral rehydration therapy
- OTC, over the counter
- SF, serum ferritin
- WBC, white blood cell
- micronutrients
- diarrhoea
- zinc
- probiotic
- lactic acid bacteria
- randomised clinical trial
- Sprinkles
- Pakistan
Statistics from Altmetric.com
- AKU, Aga Khan University
- EPEC, enteropathic E coli
- ETEC, enterotoxic E coli
- HPF, high power field
- HSC, Hospital for Sick Children
- LAB, lactic acid bacteria
- MB, micronutrients which included LAB
- MZ, micronutrients which included zinc
- ORT, oral rehydration therapy
- OTC, over the counter
- SF, serum ferritin
- WBC, white blood cell
Gastroenteritis, a common recurrent symptom complex, is held responsible for 80% of the 2 million deaths among young children in developing countries.1–,3 These same children are also at risk of micronutrient deficiencies and poor nutritional status.4 A meta-analysis of zinc trials has shown a reduction in morbidity and mortality from diarrhoea,5 and several trials with lactic acid bacteria (LAB) have also shown encouraging results.6,7 An impediment to their use, however, has been the absence of a reliable strategy for daily distribution, especially for viable LAB (also called probiotics), which must be kept refrigerated to maintain their viability.8
We recently developed “Sprinkles” as a “home fortification” approach, to provide iron and other micronutrients to children.9–,12 Sprinkles are single dose sachets (like small packets of sugar or artificial sweetener) containing micronutrients in powder form which are easily sprinkled onto complementary (weaning) foods prepared in the household. Any homemade or unfortified food can be thus fortified by Sprinkles to administer once-a-day doses of micronutrients. Given the recent evidence of the efficacy of zinc and a new “heat inactivated” strain of LAB in diarrhoea related morbidity, it became apparent that Sprinkles may also be used as a vehicle to deliver zinc and LAB. Heat inactivated LAB are stable even at high environmental temperature and importantly, they still enhance immune response and inhibit adhesion to invasion of enteropathogens.6,13,14 Reduction in sodium and water secretion and increase in intestinal brush border enzyme activity have also been observed with their use.8 Thus, we examined the effect of micronutrients including zinc, or both zinc and heat inactivated LAB, on longitudinal prevalence of diarrhoea in children at risk of diarrhoea related mortality, compared to placebo.
METHODS
Study design
The study was a triple blind, randomised, placebo controlled trial conducted between January and March 2003 in Bilal Colony, Korangi, Karachi, Pakistan; an urban slum area where the Aga Khan University (AKU) has a community outreach centre. All geographical zones of Bilal colony were included in the trial (total population ∼40 000; young children ∼12 400). Eligibility criteria were: (a) age 6–12 months; (b) ingesting any type of semi-solid weaning food; (c) ⩾1 episode of diarrhoea within the past two weeks; (d) intent to reside in the area for ⩾2 months; and (e) parental consent.
Clinical procedures and baseline assessment
From the registry of the AKU outreach centre, we compiled a list of 6–12 month old children. Field workers accompanied by a physician visited parents of these children at home and explained the purpose, methods, and risks of the study in local language or dialect; they also obtained consent to participate in the study after explaining the consent forms to the parents.
At enrolment, using a standard board and weighing scale, we measured height and weight; these anthropometry measurements were taken twice on each child and the mean was recorded. We also gathered information on sociodemographic characteristics via structured pre-coded questionnaires. In addition, using the training manual of the World Health Organisation (WHO),15 we educated the mothers on how to administer proper home treatment of diarrhoea with oral rehydration therapy (ORT). We asked the mothers to watch for signs of worsening diarrhoea and dehydration and advised them to bring their children to the AKU community outreach facility for proper assessment and treatment, if needed.
Randomisation, blinding, and interventions
Using a computer program, we randomly assigned eligible children from each geographical zone to micronutrients which included zinc (MZ), micronutrients which included zinc and heat inactivated LAB (MB), or placebo, with a 1:1:1 ratio. Micronutrients were provided as Sprinkles and included zinc gluconate (5 mg), encapsulated ferrous fumarate (30 mg), vitamin C (50 mg), vitamin A (300 μg), vitamin D3 (7.5 μg), and folic acid (150 μg). LAB were L acidophilus at a concentration of 1–2×109 CFU per dose; placebo was ground purple rice with maltodextrin. The heat inactivated LAB were donated by the Institut Rosell Lallemand (Montreal, Quebec, Canada).
We supplied identical small screw-cap plastic containers filled with micronutrients (with or without LAB) or placebo in powder form which were similar in appearance and taste. Study participants, field staff, and the data analyst were blinded to the random allocation. We instructed mothers or care-givers to open the containers and mix the entire contents with whatever semi-solid meal they served to participating children once each day. Thus, these were single dose supplements.
Monitoring of participants
Field workers visited participants at home twice a week to collect information on the number of diarrhoeal stools, days of diarrhoea, dysentery, vomiting, presence of fever (and its intensity and duration), respiratory symptoms, and drug usage through structured pre-coded questionnaires and a modified Bristol stool form scale (available on the ADCwebsite: http://www.archdischild.com/supplemental). Prior to the commencement of the study, the first author visited the field site and tested these instruments on ineligible participants. Whenever possible, field workers collected stool samples for children with diarrhoea.
At the end of two months, we collected venous blood samples.
Main outcome measures
The primary outcome was longitudinal prevalence of diarrhoea. Diarrhoea for a given day was defined as ⩾3 liquid or loose stools in the past 24 hours, and longitudinal prevalence of diarrhoea as the percentage of the days that the child had diarrhoea over the observation period. Secondary outcomes were febrile days per child, compliance, and haemoglobin (Hb) and serum ferritin (SF) concentrations.
Compliance
Using a structured questionnaire, we collected information on the number of supplements consumed (out of the total assigned for the participating child) and also asked whether supplements were lost or shared with other family members. Compliance was also measured by counting used supplements for each child whose supplements were not shared or lost.
Laboratory investigations
The central laboratory at AKU analysed all samples. For stool samples, the number of white blood cells per high power field (WBC/HPF) was estimated. If ⩾8 WBC/HPF were found, stool was cultured for Salmonella, Shigella, Campylobacter, Yersinia, enteropathic E coli (EPEC) and Vibrio cholera, and ELISAs were completed for enterotoxic E coli (ETEC) and Giardia lamblia. If <8 WBC/HPF were found, ELISAs for rotavirus and Cryptosporidium parvum were performed. Blood samples collected at the end of the study were analysed for Hb and SF concentrations using Coulter MaxM instrument (Beckman Coulter Inc. Fullerton, CA) and ELISA methods, respectively.
Ethical considerations
Approval was granted by the Research Ethics Committee of AKU, Karachi Pakistan, and the Research Ethics Board of the Hospital for Sick Children (HSC), Toronto ON, Canada.
Sample size
Our power calculation was based on detecting differences in longitudinal prevalence of diarrhoea (log transformed) between the three groups. We simulated published values of longitudinal prevalence of diarrhoea,16 log transformed these values (using natural logarithmic scale), and estimated the standard deviation (SD = 0.5; placebo group). Since a 5% absolute increase in longitudinal prevalence of diarrhoea is associated with a 17% increased risk of mortality,16 we considered a 5% difference in longitudinal prevalence of diarrhoea between groups to be clinically meaningful. We thus estimated that 25 children per group would ensure a power of 86% (α = 0.05) to detect “between group” differences for longitudinal prevalence of diarrhoea (log transformed).
Data entry, processing, and analyses
Data forms were checked for completeness and validity before computer entry at AKU. A Fox Pro v6 (Microsoft, Seattle, WA) double entry program was designed to detect numerical and logical inconsistencies. After completion of data entry, data were electronically transferred to HSC.
Raw data included information on stool forms and stool counts for each observed day on each child as well as duration and intensity of fever and drug usage for each week. After applying the criteria for the presence of diarrhoea on each day (based on stool forms and counts), we counted the number of diarrhoea days for each child and divided it by the child’s number of observed days; thus we obtained a single value of longitudinal prevalence of diarrhoea for each child. We excluded children who were not observed for at least seven days; this was because all children were included with recent history of diarrhoea and too few days of observations would grossly overestimate longitudinal prevalence of diarrhoea. Again, we created a single variable for febrile days by counting the number of days of fever given that the child’s mother had reported a high grade fever. Data for drug usage included proprietary names of several antipyretic, analgesic, antidiarrhoeal and antibiotic drugs. We reduced these data to two categories: (a) over the counter (OTC) drugs; and (b) antibiotics. We coded OTC drug usage as a count of the number of days any of these drugs were used for each child; we coded antibiotic usage as a binary variable which indicated whether the child ever took an antibiotic, or the child never took an antibiotic during the study.
Preliminary analyses involved examining the data with histograms, box plots, and descriptive statistics. To compare groups for primary and secondary outcomes, we used general linear models when data were normally distributed (or could be normalised by transformation) and Kruskal-Wallis test otherwise. These analyses were based on the intention-to-treat principle. Thus, longitudinal prevalence of diarrhoea was normalised by transforming each child’s longitudinal prevalence of diarrhoea using the following formula:

SF concentrations were normalised by taking natural logarithm of the SF values. However, febrile days could not be normalised. In the general linear model, we step-wise included age, sex, weight, socioeconomic factors, and drug usage as covariates to adjust for any confounding effects. All data processing and statistical analyses (including sample size calculations) were carried out using SAS (version 8.2; SAS Institute, Inc., Carey, NC); p < 0.05 was considered significant for hypothesis testing. After completing all statistical analyses, we broke the code for group assignment.
RESULTS
Baseline and follow up rates
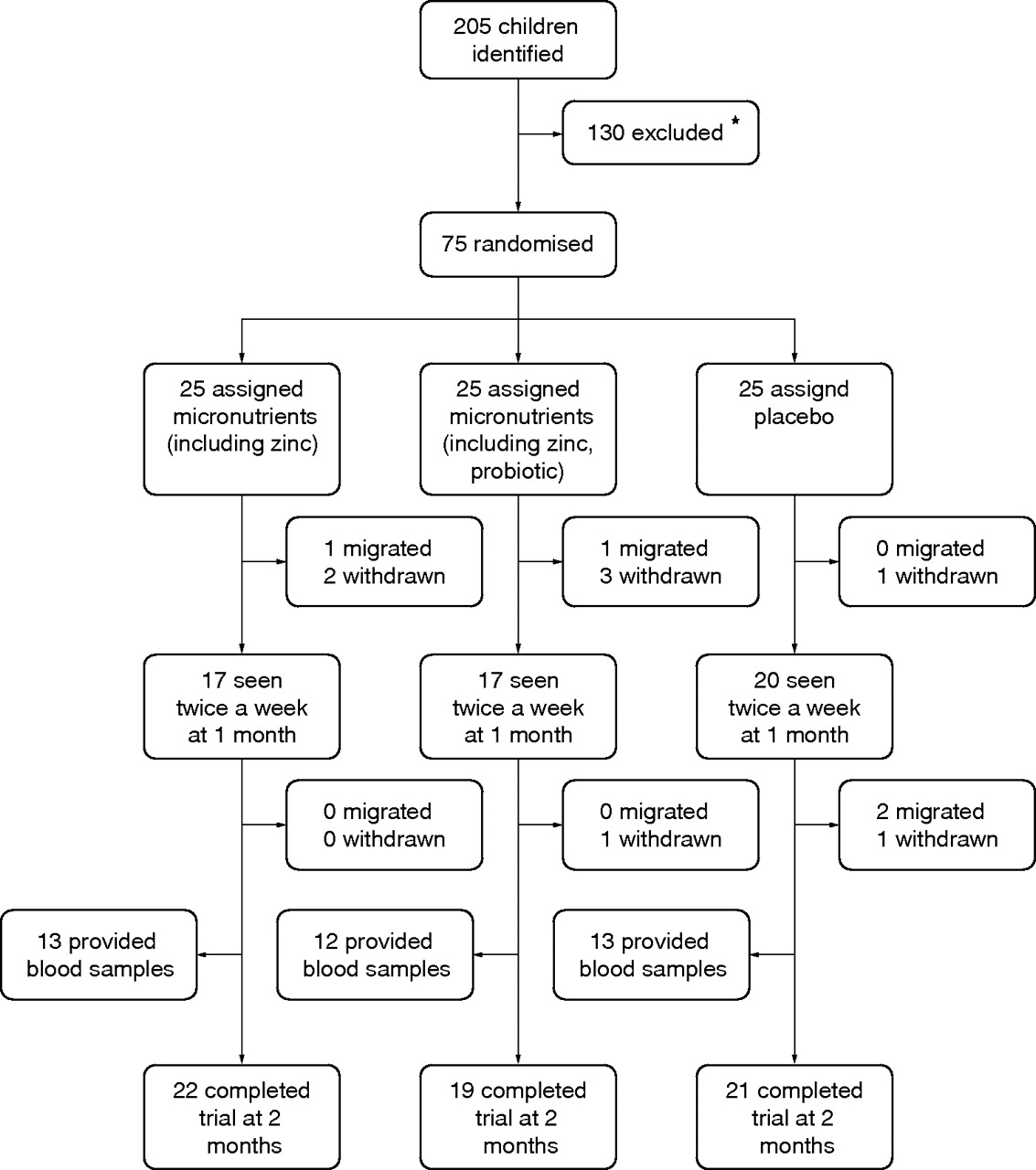
A total of 205 children were identified to be within 6–12 months of age and whose parents were willing to participate in the study; 130 were excluded (125 for no recent history of diarrhoea, two for not starting weaning foods, and three for families planning to move out of the study area). Seventy five children were randomised to the three groups. Cross sectional follow up rates for mid-study and end of study were 54 of 75 (72%) and 62 of 75 (83%), respectively, which were similar for all groups. During the trial, eight children dropped out and five moved out of the study area. For twice weekly community based case surveillance including baseline and final visit (17 visits), 873 of 1275 (68%) planned child contacts were made. However, 38 of 62 (61%) agreed to provide a blood sample at the end-of-study. The trial profile is shown in fig 1⇓.

Trial profile. *125 excluded for no recent history of diarrhoea, 2 for not starting weaning foods, and 3 for families planning to move out of the study area.
Baseline characteristics
At baseline, groups were similar for age, anthropometric measures, feeding and vaccination history, and morbidity indicators (table 1⇓). They also had similar sociodemographic characteristics (table 2⇓).
Baseline characteristics
Sociodemographic characteristics
Effect on diarrhoea and fever
Figure 2⇓ shows the distribution of longitudinal prevalence of diarrhoea in the three groups. After adjusting for differences in age which was the only significant variable (p = 0.03) out of the variables tested in the general linear models, mean longitudinal prevalence of diarrhoea was significantly lower in the MZ group compared to the placebo (p = 0.009) and MB groups (p = 0.007); the difference between the MB and placebo groups was not significant (p = 0.28). A similar pattern was observed for febrile days per child (table 3⇓). Five children were excluded from the analysis because they were not observed for at least seven days: four from the MB group and one from the MZ group. All but one had three days of diarrhoea out of three days of observation; the one child did not have diarrhoea on any of the three days that he was observed.
Outcomes at the end of study
{kind=link}
{kind=link}
Box plots of longitudinal prevalence of diarrhoea. MB, micronutrients (including zinc) and lactic acid bacteria; MZ, micronutrients including zinc. Data in box plots are on a log transformed scale; lower edge, line, and upper edge of the box represent the 25th, 50th, and 75th centiles, respectively; distance between upper and lower edge is the interquartile range (IQR); endpoint of lower whisker is located 1.5 times the IQR below the lower edge of the box and endpoint of upper whisker is located 1.5 times the IQR above the upper edge; values beyond the endpoints of upper and lower whiskers are outliers represented by squares.
Diarrhoea pathogens
A total of 31 stool samples from 30 children were collected. Eight samples had ⩾8 WBC/HPF; two were positive for Giardia lamblia. Of the 23 stool samples with <8 WBC/HPF, two were positive for rotavirus.
Effect on iron status
At the end of the study (table 3⇑), Hb and SF concentrations were higher in MZ and MB groups compared to placebo, although the differences between groups were not significant.
Measure of compliance
All children received at least 20 doses (one third of maximum total), 91% received at least 30 doses (one half of maximum), 9% received at least 40 doses, and no child received all 60 doses. The mean number of supplements taken per child was 36 (SD = 6) and was similar in all groups; 36 (SD = 7) supplements were taken in the MZ group, 36 (SD = 4) in the MB group, and 38 (SD = 7) in the placebo group. There was a strong correlation between the two measures of compliance: count of used supplements and self-report (r = 0.84). Eight (0.2%) supplements out of the total 4500 assigned for all children were lost and sharing was reported twice. No adverse events were reported during the study.
DISCUSSION
Principal findings
We studied the effect of micronutrients including zinc and heat inactivated LAB on longitudinal prevalence of diarrhoea in young children (most of whom were still being fed with breast milk in addition to complementary foods) because it is correlated with mortality.16 In the current study, there was an absolute mean reduction of 11% in longitudinal prevalence of diarrhoea in the MZ (micronutrients–zinc) group compared to the placebo group. In addition, children in this group also had fewer febrile days compared to placebo. However, in the MB (micronutrients–zinc–LAB) group, children had more days of diarrhoea and fever, although the differences were not significant in relation to placebo.
Comparison with other related research
The observed effect of zinc on longitudinal prevalence of diarrhoea in the MZ group is consistent with patterns observed in other studies of zinc supplements;5,17 however, the effect is not directly comparable because of the differences in analytical algorithms—we used longitudinal prevalence of diarrhoea and others have used cross-sectional prevalence or episodic prevalence of diarrhoea. The lack of effect in the MB group is also not comparable to previous research since to the best of our knowledge, the current study is the first to examine zinc and a heat inactivated LAB in combination.
Meaning of the study: possible explanations and implications for clinicians and policymakers
There is little doubt that nutritional status influences immune function and resistance to disease.18 Immuno-modulating nutrients in proper combinations may act synergistically to lower morbidity and mortality in children. It is known that vitamin A,19 LAB,20 and zinc21 have immuno-potentiating effects and their daily use may enhance acquisition of immunity after pathogen exposure. Recently, the WHO and the United Nations Children’s Fund (UNICEF) have recommended zinc supplements for young children to prevent diarrhoea related mortality.22 However, the ratio among nutrients might be important for optimising their beneficial effects. Baqui and colleagues reported lower rates of diarrhoea and respiratory tract infections with the use of a combination of zinc (20 mg) and iron (20 mg); however, Hb and ferritin concentrations were lower in this supplemented group compared to the control group.23 Our results with the use of a combination of zinc (5 mg) and iron (30 mg) do not support a negative effect on iron indices.
Recently, adverse gastrointestinal symptoms and diarrhoea with the use of heat inactivated LAB in young children have been reported in a trial which necessitated premature termination.24 The authors suggested that one possible explanation for these negative effects was that the heat inactivation process may cause denaturation of surface peptides and expression of heat shock proteins. These heat inactivated LAB would induce inflammatory responses and consequently increase gut permeability. The authors questioned the use of heat inactivated LAB in young children. In the current study, it appears that heat inactivated LAB induced inflammation in children which neutralised the effect of zinc in the MB group—thus, there was no difference in diarrhoea and febrile days between MB and placebo groups. Another possible explanation for the observed results is that higher rates of febrile episodes in the MB and placebo groups led to greater consumption of antibiotics that induced diarrhoea and thereby increased the longitudinal prevalence of diarrhoea. We believe however, that this is unlikely, since the mean longitudinal prevalence of diarrhoea in the placebo group was similar to literature based estimates of diarrhoea burden in developing countries,25 and antibiotic use was reported in two participants only. These two children were assigned to placebo and had longitudinal prevalence of diarrhoea values of 22% and 30% with two and six days of fever, respectively; excluding these two individuals from the analysis did not change our conclusions. Thus, we believe that diarrhoea and febrile episodes in the MB group were related to the ingestion of heat inactivated LAB.
Reducing mortality among young children through prevention of gastroenteritis in the developing world is a daunting task. To be effective, the approach should include multiple strategies such as provision of safe water, improvements in housing, sanitation, and health care, and promotion of breast feeding. An inexpensive and effective food “supplement” designed to control micronutrient deficiencies and prevent diarrhoea could be important to such programmes where resources are limited. Sprinkles could be readily integrated with other public health programmes such as use of treated mosquito nets, chemoprophylaxis, rapid case detection and treatment for malaria, and future vaccines. In fact, the authorities in Pakistan have already decided to incorporate Sprinkles into their rural public health programmes.26
Limitations
The current study recruited 6–12 month old children with a recent history of diarrhoea, and observed these children over the supplementation period only. Thus, the study does not directly answer the question whether similar effects would be observed in older children, in children without a recent history of diarrhoea, and beyond the supplementation period; although meta-analysis of zinc prevention trials support that the effect of zinc may not be restricted to a narrow sub-group of the population or time interval.5
The negative results observed in the MB group should be interpreted with caution. We studied a heat inactivated strain of LAB, and thus our results are not generalisable to other strains of LAB. The ability of viable strains of LAB to inhibit infection by microbial pathogens and promote recovery from infection has been documented in several studies,27–,32 and shown to induce increased production of antibodies specific to Salmonella, E coli, Vibrio cholera, Shigella spp., and rotavirus.33
This study was not designed to demonstrate efficacy on iron indices for which a larger sample size and baseline blood sampling is required. Given the small number of individuals with available Hb and SF concentrations, there was more variability in the estimated measures of central tendency (means, medians). Nonetheless, Hb and SF concentrations were higher in the two intervention groups compared to placebo, although the differences were not statistically significant.
The less than ideal (100%) follow up rate in the current study should be judged within the context of the study design and setting. This was a community based study that required many data points per child. Thus, the chances of having lower follow up rates were high and not uncommon in these situations. Nevertheless, the pattern of missing data was random (fig 1⇑) and we had some level of data for 70 (93%) of 75 children (table 3⇑). Hence, it is unlikely that our conclusions would have changed had we achieved a 100% follow up rate.
Conclusion and future research
This study suggests that Sprinkles may be an effective and programmatically practical intervention for control of morbidity (and perhaps mortality) in children with diarrhoea and other infections. Further large studies are needed to evaluate their effectiveness and cost effectiveness in different health system settings.
What is already known on this topic
Of the micronutrient deficiencies which are common in developing countries, zinc deficiency is associated with diarrhoea related morbidity and mortality, and iron deficiency is associated with impaired cognitive development
Sprinkles is a home fortification approach to deliver micronutrients and is effective against iron deficiency in young children. There is evidence that several strains of lactic acid bacteria (live or heat inactivated) are effective in the treatment and prevention of diarrhoea in young children
What this study adds
Home fortification with Sprinkles (including zinc and iron) reduces diarrhoea related morbidity as well as iron deficiency
Heat inactivated lactic acid bacteria have negative effects in infants
Acknowledgments
We acknowledge Dr Ayesha Mirza and other staff of AKU for their help in conducting this study.
REFERENCES
Supplementary materials
Files in this Data Supplement:
- view PDF - Pictorial tool to collect information on stool patterns.
Footnotes
Published Online First 23 March 2006
Funding: The study was supported in part by grants from Canadian Institutes of Health Research, HJ Heinz Foundation, and Institut Rosell Lallemand. The sponsors had no role in study design, data collection, data analysis, and data interpretation, or in writing the paper.
Competing interests: S Zlotkin owns the intellectual property rights to micronutrient Sprinkles. Any profit net of expenses generated from licensing agreements for the production of Sprinkles is donated to the Hospital for Sick Children Foundation.
Linked Articles
- Précis
- Atoms