Article Text

Abstract
Background The health benefits of 150 min a week of moderate-to-vigorous-intensity physical activity (MVPA) in older adults, as currently recommended, are well established, but the suggested dose in older adults is often not reached.
Objectives We aimed to determine whether a lower dose of MVPA was effective in reducing mortality, in participants older than 60 years.
Methods The PubMed and Embase databases were searched from inception to February 2015. Only prospective cohorts were included. Risk ratios of death were established into four doses based on weekly Metabolic Equivalent of Task (MET)-minutes, defined as inactive (reference), low (1–499), medium (500–999) or high (≥1000). Data were pooled and analysed through a random effects model using comprehensive meta-analysis software.
Results Of the 835 reports screened, nine cohort studies remained, totalling 122 417 participants, with a mean follow-up of 9.8±2.7 years and 18 122 reported deaths (14.8%). A low dose of MVPA resulted in a 22% reduction in mortality risk (RR=0.78 (95% CI 0.71 to 0.87) p<0.0001). MVPA beyond this threshold brought further benefits, reaching a 28% reduction in all-cause mortality in older adults who followed the current recommendations (RR=0.72 (95% CI 0.65 to 0.80) p<0.0001) and a 35% reduction beyond 1000 MET-min per week (RR=0.65 (95% CI 0.61 to 0.70) p<0.0001).
Conclusions A dose of MVPA below current recommendations reduced mortality by 22% in older adults. A further increase in physical activity dose improved these benefits in a linear fashion. Older adults should be encouraged to include even low doses of MVPA in their daily lives.
- Elderly people
- Physical activity
- Health promotion
- Public health
- Meta-analysis
Statistics from Altmetric.com
Introduction
It is well established that regular physical activity is an efficient strategy for successful ageing.1–3 It increases life expectancy and improves quality of life.1–3 It has been shown to reduce all cause-mortality.1–7
The Physical Activity Guidelines Advisory Committee Report recommends a minimum of 150 min of moderate-intensity or 75 min of vigorous-intensity physical activity per week, or an equivalent combination of moderate and vigorous physical activity.2 A metabolic equivalent of task (MET), is a unit useful for describing the energy expenditure of a specific physical activity. On the basis of Ainsworth's compendium of physical activity, resting energy expenditure is assumed to be 1 MET. Physical activity of 3–5,9 metabolic units (METs) is defined as moderate, and physical activity ≥6 METs is considered as vigorous.8 ,9 A combination of four METs of physical activity for 15 min and six METs of physical activity for 15 min 5 days a week is equivalent to 750 MET-minutes per week. Total weekly physical activity between 500 and 1000 MET-minutes produces substantial health benefits.10 Indeed, studies showed that achieving these recommendations of 150 min of moderate-to-vigorous physical activity (MVPA) per week (ie, 500–1000 MET-min per week) reduced mortality by 20–30%.2 ,7
Some studies have reported health benefits in older adults (over 60 years of age).11–57 Few of them assessed the MVPA.19 ,29 ,33 ,41 ,45 ,46 ,49 ,50–57 However, most of the physical activity guidelines are the same for middle-aged adults and older adults.2 ,3
It is estimated that over 60% of older adults are not able to achieve 150 min per week of MVPA,58 as it may be too demanding for them. They more often cite poor health as the main barrier to physical activity. The lack of knowledge of the relationship between physical activity and health benefits is also a particularly relevant barrier, especially because physical activity was not recognised as a health enhancing behaviour for much of their lives.47 ,58
Recently, some researchers have documented benefits of physical activity at doses below the currently recommended amount. Wen et al53 reported positive health effects in a non-specific population of individuals aged over 20 years who engaged in physical activity at half the recommended level, 75 min a week, or 15 min of MVPA at least 5 days a week. More recently, Lee et al59 underlined, in The Aerobics Center Longitudinal Study (mean age 44 years), that running even at relatively low doses (5–10 min per day), below the current minimum guidelines of MVPA, was sufficient for substantial mortality benefits (HR: 0.72; 95% CI 0.59 to 0.88 for all-cause mortality). Thus, the question arises as to whether doses of physical activity below the currently recommended dose, which includes notions of intensity, duration and frequency,2 ,10 may benefit older adults. Showing the benefits obtained by engaging in lower doses of moderate-intensity to vigorous-intensity physical activity might encourage this growing elderly population to adhere to physical activity in the long term. This may have a positive impact on public health.
The prescription of physical activity for older adults needs to be clarified: what ‘dose’ of physical activity is required? Is a lower dose sufficient for older adults, as demonstrated by Wen et al,53 in the general population? The main objectives of this systematic review and meta-analysis were to determine whether a dose of MVPA below the recommended level was effective in reducing mortality in older adults.
Methods
Data sources and eligibility criteria for selecting studies
Studies were selected from the PubMed and EMBASE databases in February 2015 following the Cochrane strategy (http://www.chmg.cochrane.org/resources-review-authors) and using the combination of keywords: (“Mortality”[Mesh]) AND (“Motor Activity”[Mesh] OR “Leisure Time” OR “Physical Activity)” AND (“Cohort Studies”[Mesh] OR “Prospective Studies)”, limited to articles dealing with humans and written in English. In addition, the references of the selected studies and available reviews were screened for cohort studies missed out in the computerised search. The criteria for inclusion in our study were: (1) prospective cohort study; (2) participants aged 60 years and above; (3) absence of any known neurodegenerative disease at the start of the cohort study; (4) evaluation of MVPA of participants at the time of inclusion in the cohort; (5) reported deaths (all causes) during follow-up; (6) follow-up of at least 3 years; (7) relative risks (RRs) of mortality calculated according to the statistical method used with CIs at 95%; and (8) sufficient methodological quality of the study (see below). Exclusion criteria were: (1) evaluation of a low-intensity (1.6 to 2.9 METs) of physical activity; and (2) over 15% of loss to follow-up or incomplete data (mostly CIs or insufficiently defined cohorts, lack of accurate definitions of duration, intensity and frequency of physical activity). The authors of this study had no research, professional or personal contacts with the authors of the published studies. Two investigators (DH and PE) selected the studies independently. Any disagreements were resolved by discussion and a consensus was accepted.
Assessment of the methodological quality of studies
The methodological quality of each study was assessed using two methodology checklists: The Scottish Intercollegiate Guidelines Network (SIGN)60 and the Centre for Evidence Based Medicine (CEBM).61 The combination of these two methodology checklists led to the inclusion of only studies with high-quality methodology, standardised the reading of the articles and minimised potential bias without loss of information. Studies were excluded as soon as they were not considered of high quality by both checklists (eg, SIGN: yes to all items for internal validity and high (++) or acceptable (+) quality for the overall assessment of the study; and CEBM: yes for each item assessing the internal validity of the study). Studies of high methodological quality but for which the dose was unquantifiable (no intensity data or duration, or frequency), were excluded.
Data extraction
The following data from each study were checked and recorded: country and size of population sample, mean age (±SD) and age range of participants, duration of study follow-up in years, total mortality, evaluation tools to evaluate physical activity and RR ±95% CI with adjustment for confounding variables (such as age, sex, overweight, smoking, elevated blood pressure, type 2 diabetes, plasma cholesterol level, cardiovascular and chronic diseases, cancer, depression, educational level and self-reported health).
‘Dose’ of physical activity
The ‘dose’ was determined by three components of physical activity: intensity, duration and frequency. Intensity was assessed in MET2 ,10: 3–5.9 for moderate (eg, brisk walking) and ≥6 for vigorous (eg, running). Duration was estimated in minutes per week or per day, and frequency was measured in days per week. The ‘dose’ was quantified according to the data collected in each study. We defined threshold values for each unit to classify older populations in four classes depending on MVPA dose2 ,10: 30 of MVPA 5 days a week as recommended by international societies1–3 for chronic disease prevention, corresponds to an average time of 150 min/week and to an average energy expenditure of 1000 kcal per week.2 ,10 We converted exposure measures from each study into MET-min of MVPA per week using the compendium of activities.8 ,9 Based on the MET-min cut-offs used in the 2008 Physical Activity Guidelines for Americans, we grouped the weekly MVPA into four categories: physical inactivity such as no activity beyond baseline activities of daily living (0 MET-min), low physical activity (1–499 MET-min), medium physical activity (500–999 MET-min) and high physical activity (≥1000 MET-min).2 ,10
Statistical analysis
The studies included in this meta-analysis all used proportional hazards models or logistic regression models. In multivariate-adjusted studies, RRs were reported with corresponding CIs. D’Agostino et al62 investigated the relationship between the estimation of RRs from proportional hazard models and from logistic regression models. They concluded that pooling estimated RRs from these two models was acceptable and led to accurate results. Multivariate-adjusted estimates were derived from models after adjusting for all relevant confounders in the corresponding studies. All results presented were RRs of all-cause mortality associated with one of the three doses of MVPA compared to inactivity (reference dose for which the RR was set at 1). The linear regression was used to show the linear relationship between MVPA dose and mortality reduction. Mortality data related to cardiovascular disease and cancers were also analysed when available. Comprehensive Meta-Analysis software (V.3.3.070—21 November 2014, Biostat, Englewood-USA) was used to pool RR estimates for the total cohorts. The effect sizes were pooled using the DerSimonian and Laird random effect model because (1) there were more than three studies and (2) there was heterogeneity within studies (I2>25).63–65 The fixed effects meta-analysis model was used to calculate average RR within the same study when there were more than four doses of MVPA. If the given doses of exposure were shorter in duration than the relevant cut-offs, we assumed the exposure was based on the longer duration of MVPA (eg, 1–299 and 300–449 for the low dose in Brown et al52). Forest plot (with 95% CI) was constructed for the low, medium and high MVPA doses, to demonstrate the individual and pooled effect estimates, and to allow visual inspection for study heterogeneity. Heterogeneity between studies was assessed by the I2 test and Cochran's homogeneity test. All meta-analysis procedures were performed on the logarithmic RR scale and results were then transformed into the RR scale.64 ,65 Sensitivity analyses were performed to examine the influence of meta-analysis variables on the association between MVPA and all-cause mortality, including gender distribution (male, female and mixed) and type of questionnaire used (validated or not in adults). In all analyses, p<0.05 was used as the significance level.
Results
Nine cohort studies focusing exclusively on the relationship between MVPA and mortality in older adults were included (figure 1 and online supplementary table S1).
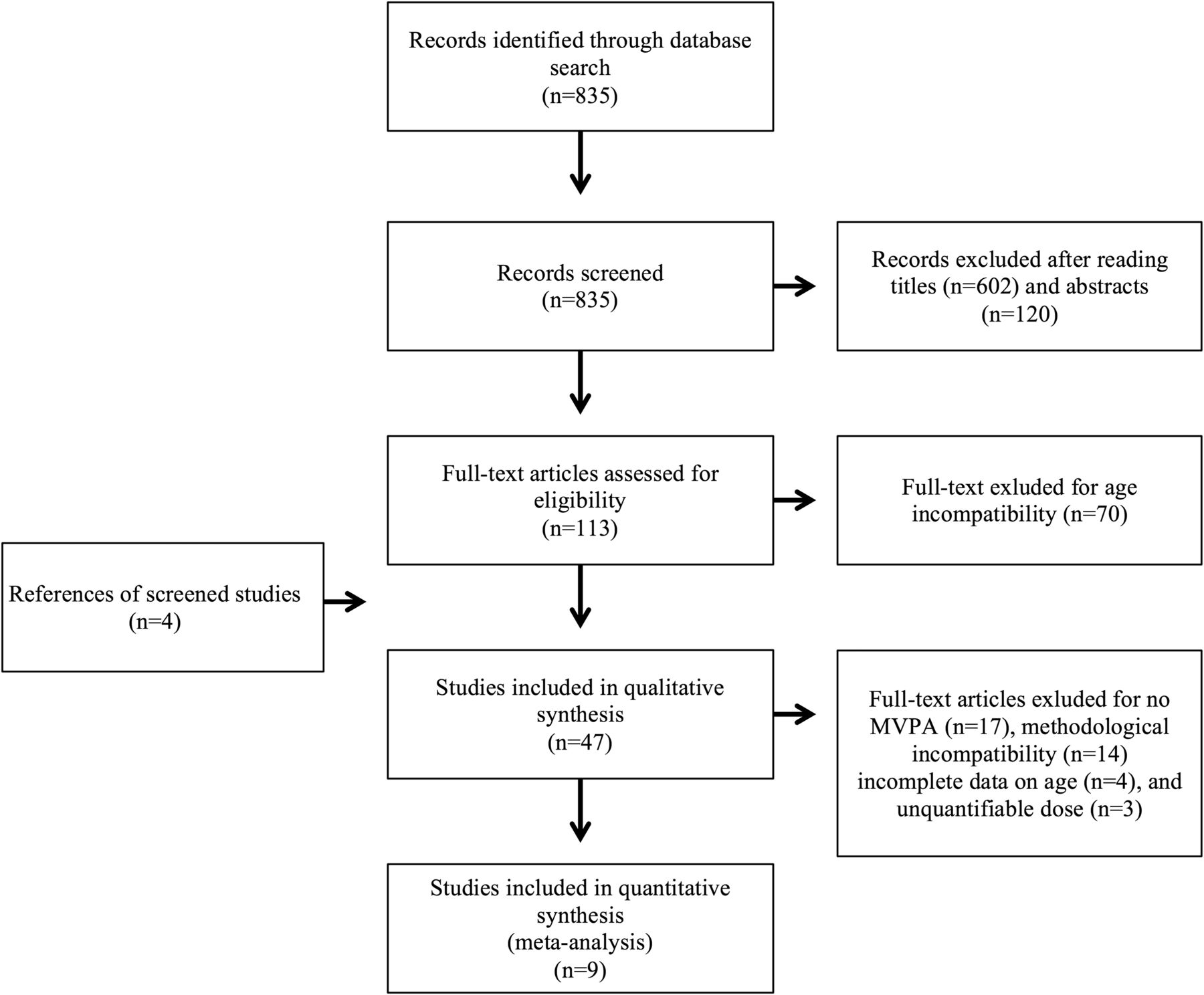
Selection of studies for meta-analysis on Pubmed and Embase in February 2015.
The studies selected led to the inclusion of a total cohort of 122 417 participants aged 60 years and above (73 745 women and 48 672 men, mean age (only for 7 cohorts) 72.9 years (±4.5) ranging from 60 to 101). The average size of cohorts was 13 602 participants (median: 6292), with a maximum for the Asian cohort of Wen et al53 (51 295 participants) and a minimum for the Women’s Health and Aging Study of Xue et al51 (433 participants). Four cohorts included only women (44%),51 ,52 ,55 ,57 two, only men (22%),52 ,54 and three were mixed (33%).50 ,53 ,56 Six cohorts were American,50 ,51 ,54–57 two were from the Pacific region,52 and one was Asian.53 The average follow-up of these studies was 9.8 years (±2.7). Overall, 18 122 (14.8%) deaths were reported.
The present meta-analysis revealed that a low dose of MVPA (1–499 MET-min per week) led to a 22% reduction in mortality (RR=0.78 (95% CI 0.71 to 0.87) p<0.0001) (figures 2 and 3). Mortality was 28% lower in older adults who followed the current recommendations of 150 min of MVPA (500–999 MET-min) per week than in their sedentary counterparts (RR=0.72 (95% CI 0.65 to 0.80) p<0.0001) (figures 2 and 3). This relationship was even stronger when doses of MVPA were higher. Indeed, mortality risk in elderly participants who engaged in high MVPA (well above current recommendations, ≥1000 MET-min per week) was 35% lower (RR=0.65 (95% CI 0.61 to 0.70) p<0.0001) than that in their inactive counterparts (figures 2 and 3).

Relationship between dose of moderate-to-vigorous-intensity physical activity (MVPA) and mortality reduction. Scatter plots correspond to the different relative risks of studies for each dose of MVPA. The average relative risks were calculated from nine studies for the doses of physical activity (only 8 for the low dose) via Comprehensive Meta-Analysis Software (V.3.3.070—21 November 2014, Biostat, Englewood, New Jersey, USA). Bars illustrate 95% CIs. Mortality reduction was estimated by percentage (±95% CI) in the figure. MET, Metabolic Equivalent of Task.

{kind=link}
{kind=link}
{kind=link}
Multivariate-adjusted all-cause mortality relative risk (RR) for participants of the (A) low, (B) medium and (C) high moderate-to-vigorous-intensity physical activity (MVPA) groups compared with participants in the inactive group. All RRs (RR 95% CI) of the forest plot are linked to health outcomes in participants in the inactive group (RR=1). An average RR was calculated within the same study when there were more than four doses of MVPA (Comprehensive Meta-Analysis Software, V.3.3.070—21 November 2014, Biostat, Englewood, New Jersey, USA).52 ,53 ,55 ,56.
Overall, the nine cohorts included reported an inverse correlation between the dose of MVPA and mortality risk (figures 2 and 3). The magnitude of the correlation increased with increasing doses of MVPA in seven cohorts.50–54 ,56 ,57 Two cohorts reported higher mortality risk in participants who engaged in a medium dose of MVPA than for those who practiced a low dose of MVPA.52 ,55
Discussion
This meta-analysis of prospective cohort studies of older adults showed that a dose of MVPA below recommended level reduced mortality among adults aged ≥60 years. The older adults who performed 1–499 MET-min per week (<150 min per week) had a 22% reduction in mortality compared with those reporting 0 min per week of MVPA. This is similar to that reported in three meta-analyses66–68 in a non-specific population aged from 20 to 85 years who engaged in 150 min of moderate-intensity physical activity per week (14%66 and 19%67 ,68). In our study, mortality was reduced by 28% in participants who achieved the current recommendations of 150 min of moderate-intensity physical activity per week.1–3 A dose-effect was clearly identified, as shown by other systematic reviews or meta-analyses.66–77 Mortality was reduced to the greatest extent (35%) in those who engaged in the highest dose of physical activity. This meta-analysis suggested a curvilinear relationship between MVPA and all-cause mortality. There is a steep initial slope: the greatest benefits are seen in those who change from doing the least or no MVPA to doing more. This relationship is linear from a medium dose to a high dose of MVPA (y=−0,065x+0.836, R2=0.969). Indeed, the increase in health benefits per unit increase in MVPA becomes smaller at the highest doses of activity. Much of the strong inverse relationship between MVPA and mortality was due to mortality from cardiovascular disease. However, MVPA was less strongly related to cancer mortality, but the decrease in risk was statistically significant (see online supplementary table S3 and figure S1).
The reduction in all-cause mortality was considerably stronger for older women when compared with older men. Men who reported a dose of MVPA below current recommendations (1–499 MET-min per week) had a 14% reduction in mortality risk (RR=0.86 (95% CI 0.80 to 0.94) p<0.001)52 ,54 compared with a 32% reduction in women in this MVPA dose (RR=0.68 (95% CI 0.63 to 0.74) p<0.0001).51 ,52 ,55 ,57 Our results confirm those of Brown et al,52 for whom a possible explanation is that the men may have overestimated, or the women may have underestimated, their MVPA. The effect of this hypothesis may have been to increase the estimated gender difference in the effect of MVPA on mortality. Similar findings were found by Bucksch.78
Based on these results, we believe that the target for physical activity in the current recommendations might be too high for older adults and may discourage some of them. The shape of the dose-effect curve appears to differ for adults older and younger than 60 years of age (figure 2).2 The decline in risk appears steeper at the lowest levels of physical activity for older rather than for younger adults even though the maximum benefits at the highest doses seem to be equivalent. The fact that any effort will be worthwhile may help convince those 60% of participants over 60 years of age, who do not practice any regular physical activity to become active.58 The current guidelines1–3 for physical activity have been widely broadcast. Adapting these recommendations to older adults and underlining the dose-effect of regular physical activity may encourage them to adopt or maintain a more active lifestyle.
Strengths and limitations
To our knowledge, this is the first meta-analysis to focus on the relationship between the dose of MVPA and all-cause mortality in older adults. The main strengths of this study are: (1) the very large sample size and the long follow-up cohorts. (2) The rigorous selection of articles following the Cochrane strategy, using two validated methodology checklists,60 ,61 which allowed us to include only studies with good methodological quality (see online supplementary table S2). (3) The relevant and homogeneous evaluation of MVPA by questionnaire.79 ,80 Among the nine questionnaires used in the selected studies, five had been validated in adults (not specifically in older adults)50 ,51 ,53–55 and one was associated with objective measurements of MVPA.56 Sensitivity analyses were performed to examine the influence of not validated questionnaire on the association between MVPA and all-cause mortality. When only studies that used objective means and/or questionnaires validated among the adults50 ,51 ,53–56 were considered, mortality was reduced by 20% in the low MVPA participants compared with sedentary participants (RR=0.80 (95% CI 0.71 to 0.89) p<0.0001). This result is not statistically different from the 22% found in the whole-set meta-analysis. Keeping only studies with objective means or validated questionnaires, mortality was 26% lower in those who followed the recommendations for physical activity than in their sedentary counterparts (RR=0.74 (95% CI 0.67 to 0.82) p<0.0001). Again, this result was not statistically different from the 28% calculated for the whole set of studies selected in the meta-analysis. For participants who engaged in high physical activity, mortality was reduced by 37% (RR=0.63 (95% CI 0.60 to 0.72) p<0.0001), which is still not statistically different from the 35% found in the whole-set meta-analysis. (4) The adjustment for confounding variables and (5) The use of a random effects statistical model with two homogeneity tests minimised the variability within single studies and between different studies. The I2 test and Cochran's homogeneity test showed a strong homogeneity between studies (I2<45%) despite a diverse pool of population samples.64 ,65
However, the present study has some limitations: (1) a bias in the analysis of the data could be due to some uncertainty in the comparison of the doses of physical activity, since we chose to group participants into four doses in comparison to the selected studies including 3–5 doses groups. (2) Two large studies53 ,57 contributed to 61% of the results of the meta-analysis. The analysis of a low dose of physical activity in older adults was not the main objective of these two studies. These results were only available in the appendix.53 ,57 The remaining seven studies corroborated a strong relationship between a dose of MVPA below current recommendations and mortality in older adults on an international scale. (3) The geographical distribution of cohorts is uneven (no European cohort).
Implications for policy and practice
Epidemiological studies are a powerful tool for scientific societies to promote recommendations regarding physical activity intended for the general population.81 Meta-analysis has the potential to be the best source of evidence to inform decision-making.82 At the present time, US recommendations for older adults are not different from those for middle-aged adults.2 ,3 Only mentioned is: “when older adults cannot do 150 minutes of moderate-intensity aerobic activity a week because of chronic conditions, they should be as physically active as their abilities and conditions allow”. Our meta-analysis showed that a weekly dose of MVPA corresponding to 250 MET-min (this is the midpoint of the range of 1–499 MET-min), which corresponds to 75 min per week or 15 min per day, has a beneficial effect on health in older adults. We demonstrated that among the different bouts of daily exercise, the end of the first 15 min of MVPA yielded the largest increase in benefits, with tapering off for the subsequent increment of 15 min. Fifteen minutes per day could be a reasonable target dose. A modification of the recommendations for physical activity in older adults that emphasises the health benefits of doses below the current recommendations may thus be warranted and beneficial. The widespread diffusion of this message will encourage more older adults to include even low doses of MVPA in their usual daily activities, without experiencing high levels of fatigue or of pain.83 This message should be relayed by general practitioners who play a key and essential role in promoting physical activity behaviour in older adults.58 Moreover, even if the physical activity dose required to decrease mortality and improve quality of life remains a matter of debate, it could be summarised as ‘Even a little is good, more may be better!’; Indeed, this year, a pooled analysis of prospective cohorts in the USA and Europe showed a benefit threshold at approximately 3–5 times the recommended MVPA minimum.84 To convey a simple and attractive message, and in agreement with Wen et al,53 we thus recommend at least 15 min of MVPA 5 days per week as a first target for older adults. This could include brisk walking, cycling, swimming or gymnastics, all possibly associated with leisure time physical activity or daily life activities. Scientific evidence is now emerging to show that there may be health benefits from light intensity activity (1.6–2.9 METs), and from replacing sedentary activities with light intensity activities, when the dose of MVPA is held constant.85–87 Future studies using objective measures of moderate-intensity, vigorous-intensity and light-intensity physical activity will be helpful to add clarity.
Conclusion
MVPA reduces all-cause mortality in older adults with the most rapid reduction per minute of added MVPA at the lowest doses of MVPA. This protective effect appears dose-dependent and is already significant for a low dose of MVPA (1–499 MET-min per week or about 15 min per day), which is below current recommendations for older adults. These results can guide future recommendations for older adults and may improve adherence to regular physical activity programmes and thus their global health.
What are the new findings?
A dose of moderate-to-vigorous-intensity physical activity (MVPA) below current recommendations reduced mortality in older adults by 22%.
Mortality was 28% lower in older adults who followed the current recommendations of 150 min of MVPA per week and 35% lower in those who exceeded the currently recommended range.
The greatest reduction in risk is seen in those who change from doing no MVPA to some MVPA (1–499 Metabolic Equivalent of Task (MET)-min per week).
How might it impact on clinical practice in the near future?
These findings may help convince currently inactive older adults that a lower dose of MVPA than currently recommended has health benefits.
Fifteen minutes per day of MVPA could be a reasonable target dose for older adults.
General practitioners who play an essential role in promoting MVPA should encourage older adults to include even low doses of MVPA in their daily lives.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors DH had full access to all data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis. DH and PE had the idea for and designed the study. All authors had a substantial contribution to the conception and design. DH and PE conducted the literature search. DH, PE and MO developed the meta-analysis methodological design. DH and PE were responsible for collection and analysis of data. DH, PE and MO provided statistical expertise. DH, PE and FR were responsible for interpretation of data. DH and PE drafted the manuscript and submitted the paper for publication. FR, VG, J-CC and J-CB critically revised the manuscript for important intellectual content. J-MG was the final external expert. All authors approved the final version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data in the manuscript are available.