Article Text

Statistics from Altmetric.com
This article discusses the diagnosis and management of myocarditis and pericarditis (both acute and recurrent), as well as other pericardial diseases.
Myocarditis
Myocarditis is the term used to indicate acute infective, toxic or autoimmune inflammation of the heart. Reversible toxic myocarditis occurs in diphtheria and sometimes in infective endocarditis when autoimmune mechanisms may also contribute. Persistent viral infection of the myocardium was first demonstrated a decade ago.1 Slow growing organisms such as chlamydia and trypanosomal infection in Chagas' disease are causes of chronic myocarditis. Non-infective causes in sarcoidosis and the collagen vascular diseases need to be sought.
Acute myocarditis and acute pericarditis are not always associated (likewise meningitis and encephalitis do not always occur together) and the clinical emphasis is usually on one or the other.
Myocarditis can be caused by many different viruses and the microbial pathogenesis may be complex. Most cases of myocarditis with onset in otherwise healthy people probably have an infectious origin, although the pathogenesis is not yet fully understood (such as the finding of a link between chlamydia and heart disease through antigenic mimicry). In western countries enteroviruses, especially coxsackie B 1–6 serotypes, are the most frequent, and the recent identification of a common coxsackie virus B and adenovirus receptor has explained why these very different virus types both cause myocarditis.2-4
Prevalence and clinical features
The prevalence of acute myocarditis is unknown because most cases are not recognised on account of non-specific or no symptoms (but sudden death may occur). Myocarditis may develop as a complication of an upper respiratory or gastrointestinal infection with general constitutional symptoms, particularly fever and skeletal myalgia, malaise, and anorexia. This systemic acute phase response increases energy production but compromises performance. Since myocarditis may not develop for several days or weeks after the symptoms and after a return to normal work and leisure activity, there is a risk of overexertion, which may be dangerous.
Diagnosis is easiest during epidemics of coxsackie infections but difficult in isolated cases. These are not seen by cardiologists unless they develop arrhythmia, collapse or suffer chest pain, the majority being dealt with in the primary care system.
Acute onset of chest pain is usual and may mimic myocardial infarction or be associated with pericarditis. Arrhythmias or conduction disturbances may be life threatening despite only mild focal injury, whereas more widespread inflammation is necessary before cardiac dysfunction is sufficient to cause symptoms.
Investigations
The ECG may show sinus tachycardia, focal or generalised abnormality, ST segment elevation, fascicular blocks or atrioventricular conduction disturbances. Although the ECG abnormalities are non-specific, the ECG has the virtue of drawing attention to the heart and leading to echocardiographic and other investigations. Echocardiography may reveal segmental or generalised wall motion abnormalities or a pericardial effusion. Echocardiography allows other causes of heart failure to be excluded but pronounced focal changes in wall motion may lead to confusion with myocardial infarction, especially if the ECG changes also suggest this.5
The chest x ray may be normal, show cardiac enlargement, pulmonary venous congestion or pleural effusions.
Evidence of myocyte necrosis may be found with an increase in creatine kinase or appearance of troponin, indicating myocytolysis. The highest enzyme concentrations occur early and will probably have returned to normal by about a week after onset.6 Cardiac autoantibodies can be demonstrated only later in the disease process.
A viral origin of myocarditis can only be proved if the virus is detected within an altered myocardium. This has become possible through molecular analyses of necropsy, transplant, and endomyocardial biopsy specimens using new techniques of viral gene amplification, which have shown persistence of viral mRNA.1 The histological diagnosis of myocarditis (fig 1) was clarified by the Dallas criteria,7 but these unfortunately did not include immunohistochemistry to demonstrate a T cell mediated immune response.

Acute myocarditis showing sheets of pale staining myocytes. Lymphocytes are seen which were identified as CD4 and CD8 cells on immunohistology.
Myocardial failure in myocarditis
Contributory causes of myocardial dysfunction include:
- (1)
- a direct cytotoxic effect of the agent, be it viral, bacterial, etc;
- (2)
- a secondary immune response, which can be triggered by any one of many different agents including non-infective ones;
- (3)
- cytokine expression in the myocardium, which plays a crucial role—for example, tumour necrosis factor α (TNF α) and nitric oxide synthase.4
- (4)
- aberrant induction of apoptosis, which may also play a part, particularly in individuals who go on to develop a chronic cardiomyopathy.4 The proportion of patients who do this is completely unknown, but a genetic predisposition to ongoing inflammation, and possibly also to viral persistence, would explain the recognition of a 25–30% familial incidence of dilated cardiomyopathy.8
Detection of a causal agent is uncommon during the early phase (or even later). Demonstration of a viral origin is dependent upon gaining serial antibody titres against specific viruses and on showing a gradual fall in titre during convalescence. Even if endomyocardial biopsy is carried out, persisting viral mRNA will be found in only 25–50% of patients with biopsy proven acute myocarditis.9
Management
The treatment of acute myocarditis is largely supportive. Effective antiviral agents are unavailable and usually inappropriate, but they need to be more extensively investigated for clinical use. Immunosuppressive agents would be inappropriate if the myocarditis were caused by the direct effect of persisting virus but potentially useful to suppress an ongoing autoimmune inflammatory response. Discouraging results were obtained in a randomised controlled trial of the use of immunosuppressive agents in the treatment of biopsy proven acute myocarditis.10 The trial was weakened by failure to include immunohistochemical techniques in the biopsy criteria and by frequent protocol violations. The use of steroids in an acutely ill patient therefore remains a discretionary clinical option in addition to the use of diuretics, angiotensin converting enzyme (ACE) inhibitors, β adrenergic blocking agents, and spironolactone.
It is recommended that whenever myocarditis is suspected exercise should be avoided.11 Interestingly, in a large Finnish epidemiological study of myocarditis, which included nearly 700 000 healthy young men, there were 10 sudden unexpected deaths of which only one was associated with acute myocarditis (and there were no cases of hypertrophic cardiomyopathy or arrhythmogenic right ventricular cardiomyopathy).5
The future development of effective treatment will depend on ability to make an early diagnosis before establishment of a myopathic process and on knowledge of whether the cause is infective or autoimmune.12
Endocardial fibroelastosis in infancy and childhood, which was associated with persistent mumps virus infection, has been almost eradicated by vaccination and the development of vaccines against the other common viruses may help reduce the incidence of myocarditis in childhood.
Prognosis
Recovery from acute myocarditis often surprises and delights after life threatening illness. Some recover seemingly normal ventricular function, but some cardiovascular reserve must have been lost because biopsies during the acute phase show myocytolysis. It is also uncertain how many will progress to dilated cardiomyopathy.13
In a recent study 147 cases of myocarditis were followed up for an average of 5.6 years. Out of 15 cases classed as fulminant, 93% were alive without transplant 11 years after biopsy compared with 45% of 132 less severe cases. Left ventricular dilatation was not as great in the fulminant cases, who were more likely to recover, as in the clinically milder cases who had bigger ventricles.14
Other causes of acute myocarditis
Lyme disease caused by Borrelia burgdorferi, a tick borne organism carried by deer, may cause an acute myocarditis, typically with a long PR interval as occurs with acute rheumatic fever. Left ventricular dysfunction is usually transient but the organism has been cultured from endomyocardial biopsy material in a patient with a dilated cardiomyopathy.
Chagas' disease, common in rural parts of Central and South America, results from infection by Trypanosoma cruzi. Although best known as a cause of heart block and cardiomyopathy in the chronic phase, it can also cause a severe acute myocarditis and sudden death. During this phase, but not the chronic one, trypanosomes can be shown lying within the myocytes.
Kawasaki disease (Japanese mucocutaneous lymph node syndrome) can cause a diffuse myocarditis in its first or second stages. Occlusion of proximal coronary artery aneurysms is the usual cause of death. Treatment with immunoglobulins during the early phases may help to prevent aneurysms from forming. The cause is still unknown but is probably infective.
Peripartum cardiomyopathy (PPCM) is a rare life threatening condition of unknown origin which occurs in women without known pre-existing heart disease. It is defined as the development of cardiac failure in the last month of pregnancy or within five months of delivery, in the absence of an identifiable origin or recognisable heart disease before the last month of pregnancy. The condition is rare and personal series are small.
Recent work has shown evidence of acute myocarditis in a majority of patients when endomyocardial biopsy is carried out early in the illness.15 The onset is most often postpartum and the origin probably immunological without an infective precipitant. This can be related to fetal–maternal incompatibility following the period of maternal immunosuppression during the pregnancy. A mortality of up to 50% has been reported but PPCM may not be as rare as is commonly thought, since subclinical cases may never be diagnosed. The use of immunosuppressive agents, in addition to full treatment for the often fulminating heart failure, is appropriate. Although transplantation has been carried out, a large measure of recovery is common in survivors as in acute myocarditis outside pregnancy. The use of ventricular assist devices as a bridge to recovery rather than transplantation is indicated for the most seriously affected patients.
A genetic predisposition may exist in these patients and occasionally patients give a history of relatives with dilated cardiomyopathy. Clinical recovery may be slow and delayed even up to a year or more after the birth. Even when it appears to be complete, a measure of cardiovascular reserve has been lost, as is indicated by the myocytolysis found on biopsy. Recurrence in future pregnancies is not invariable but there are few data. Pregnancy should therefore be discouraged in any patient with residual myocardial dysfunction and, if possible, delayed for some years.
Summary
Acute myocarditis has many different clinical presentations but, most commonly by far, mimics the onset of acute myocardial infarction. It may present with acute heart failure but only rarely as dilated cardiomyopathy of recent onset. Subclinical myocarditis is common and strenuous exercise should be avoided during acute infections.
Pericardial diseases
Pericarditis is very much a part of general medicine, developing as an acute illness or complicating rheumatic renal and malignant disease or treatment with certain drugs. Echocardiography has done much to reveal pericardial (and myocardial) involvement in “non-cardiac” conditions and to demonstrate the physiology of tamponade and constriction.
Clinical pericardial syndromes are:
Acute pericarditis
Relapsing pericarditis
Cardiac tamponade
Chronic pericardial effusion without compression
Effusive constrictive pericarditis
Constrictive pericarditis
Acute pericarditis
The features of acute pericarditis are pericardial pain, pericardial friction, and concordant ST segment elevation on the ECG.
As in acute myocarditis, there are numerous causes but frequently none is found. Acute idiopathic pericarditis is usually benign but may rapidly constrict or pursue a relapsing course before burning out. Rarely it may be associated with a clinically occult diffuse myocarditis (rather than the more usual epicarditis which is responsible for the typical ECG changes). Pericardiocentesis in such cases may be followed by collapse and cardiogenic shock and is ill-advised. Echo should prevent mistakes by checking ventricular contractile function as well as the features of tamponade.
Some important causes of pericarditis
Idiopathic
Infectious
viral
bacterial
fungal
parasitic
Immunological
relapsing pericarditis
post-infarction (Dressler's syndrome)
post-cardiotomy syndrome
associated with the connective tissue disorders
rheumatic fever
Still's disease
rheumatoid arthritis
systemic lupus erythematosus (SLE)
mixed connective tissue disease
polyarteritis and the Churg-Strauss variant
Neoplastic
Post-irradiation
Traumatic
Uraemic
Drug induced
The patient is usually febrile and the pain may be mild or severe. It is typically exacerbated by inspiration and relieved by leaning forward. A friction rub may come and go. Signs of tamponade are unusual.
The chest radiograph may be normal or the heart shadow may be slightly enlarged. There may be pleural effusions but pulmonary congestion, if present, indicates associated myocarditis.
The ECG shows generalised ST segment elevation. This is a current of injury from the superficial layers of the myocardium. The changes are usually generalised. The QRS is normal unless there is a large pericardial effusion. With resolution the ST segment becomes isoelectric and there may be T wave inversion which sometimes persists. Arrhythmias may develop.
The ECG changes of acute pericarditis may be mimicked by early repolarisation seen most often in young males. Elevated concave upward ST segments are located in the precordial leads with reciprocal depression in AVR; T waves are peaked and slightly asymmetrical with a notch and a slur on the R wave. The axis is usually vertical with counter clockwise rotation, a short and depressed PR interval, prominent U waves, and sinus bradycardia. The ST segment becomes isoelectric with exercise or administration of isoprenaline. Early repolarisation is a benign condition.
The ECG in acute pericarditis is mimicked by:
early repolarisation
acute early anterior myocardial infarction
acute myocarditis
Both changes of early repolarisation and of acute pericarditis mimic those of early acute anterior myocardial infarction. Echocardiography provides the most rapid and certain means of differentiation in most cases but not in all. Acute myocarditis also commonly mimics acute myocardial infarction. Enzyme release is usual in those who show ST segment elevation on ECG16 and echo may show regional akinesia. Coronary angiography differentiates, and endomyocardial biopsy can be performed at the same time.
Other investigations include exclusion of known causes of acute pericarditis, particularly tuberculosis which may require pericardial aspiration. In that case, the pericardium should be aspirated to dryness and all the fluid sent to the laboratory so that it can be spun down and the sediment stained for microbacteria. A tuberculin test may be negative in acute tuberculous pericarditis, which is now being seen more commonly in immigrants and HIV positive patients and is increasingly found to be caused by variant and resistant forms of mycobacteria.
Relapsing pericarditis
Relapsing or recurrent pericarditis causes episodes of chest pain with or without a friction rub, sometimes with pericardial and even pleural effusions. Each episode may last several days and be accompanied by fever. Pericarditis of any cause may be followed by this disabling condition, which is frequently not diagnosed especially if an initiating bout of acute pericarditis has not been documented. It may complicate recovery from acute myocardial infarction (Dressler's syndrome) or cardiac surgery (the postcardiotomy syndrome). Each may be followed by one or several recurrences but the most recalcitrant cases tend to be idiopathic.
The condition is benign and does not lead to constriction. It can sometimes recur for several years before burning out and is then very debilitating, with a major impact on general well being, family life, and work.
Management
Mild cases of relapsing pericarditis respond to aspirin or other non-steroidal anti-inflammatory drugs. Steroids are dramatically effective but should be reserved for severe cases and used only to treat acute attacks, as maintenance steroids do not prevent relapses and create a tendency to ever increasing dosage.
Colchicine is the treatment of choice and can also provide effective prophylaxis. It was introduced because of its efficacy in familial Mediterranean fever (polyserositis). Patients who have been treated with steroids can be weaned off them and on to colchicine. The dose for acute attacks is 1 mg followed by 0.5 mg two or three hourly to a maximum of 10 mg.17 The maintenance dose is 0.5 mg twice daily. If necessary, colchicine can be combined with indomethacin.
Pericardiectomy has been tried but fails to prevent relapses of pain. This is to be expected as the inflammation may be a reaction to epicardial (or viral) material recognised as foreign, so there is no reason why removal of the fibrous pericardium should make a difference.
Cardiac tamponade
Tamponade may occur in pericarditis of any cause but is uncommon in idiopathic and post-infarction pericarditis. It is usual in acute pyogenic, tuberculous, and malignant pericarditis. Acute haemopericardium may cause tamponade following cardiac rupture after myocardial infarction, in dissection of the aortic root or after cardiac surgery. Metastatic carcinoma, as well as primary tumours, may present with tamponade.
Patients with tamponade may complain of shortness of breath, weakness, heaviness in the chest, or present with hypotension or even cardiogenic shock.
Examination reveals pulsus paradoxus, a high venous pressure in the neck, and a quiet heart with faint heart sounds. It is readily diagnosed in patients known to be at risk but often missed in a previously fit individual or, for example, in a patient with septic shock where the shock is actually caused by pericardial tamponade rather than by septicaemia.18
Echocardiography is diagnostic, and has shown that inspiratory increase of blood flow into the heart is accommodated in the right atrium and admitted to the right ventricle at the expense of left ventricular volume as the ventricular septum moves sharply towards the left ventricle, reducing left ventricular stroke volume. Diastolic collapse of the right atrium and right ventricular walls are seen when pericardial pressure rises to exceed the intracardiac pressure, terminating further flow into the heart and thereby reducing or removing the Y descent of the venous pulse, which shows very small volume excursion and may therefore be difficult to see.
Pericardiocentesis should be performed in the cardiac catheterisation laboratory under ultrasound guidance, in addition to fluoroscopy and ECG, and preferably with simultaneous cardiac pressure monitoring. The sub-xiphoid approach is the safest. Pericardioscopy has been used to facilitate diagnostic pericardial biopsy. Triamcinolone can prevent recurrence of immunologically based effusions and cisplatin can deter re-accumulation of malignant effusions.19
Chronic pericardial effusion without compression
Large lax effusions occasionally occur, may cause few symptoms, and are found accidentally. It is unusual to find a cause. A very few may be associated with myxoedema.
Effusive constrictive pericarditis
When pericardial effusion is associated with thickening of the visceral pericardium the patient may have persistent cardiac compression, even after pericardiocentesis. It may be seen in tuberculous pericarditis, rheumatoid patients or after mediastinal irradiation.
Constrictive pericarditis
When thickening and scarring of the parietal and/or visceral pericardium compresses the heart and restricts cardiac filling, stroke volume becomes limited despite a considerable rise in filling pressure. Constriction is usually generalised but rarely may be localised, owing to constricting bands usually in the left or right atrioventricular grooves or round the entry of the superior or inferior vena cava.
A tuberculous origin is uncommon now in the west and most cases are idiopathic. A few are associated with rheumatoid arthritis, collagen vascular disease or uraemia, or rarely follow cardiac surgery or irradiation.
The heart is small and pulmonary venous congestion rare. The diastolic pressures in the four cardiac chambers will be similar and the left atrial pressure is rarely high enough to cause pulmonary congestion.
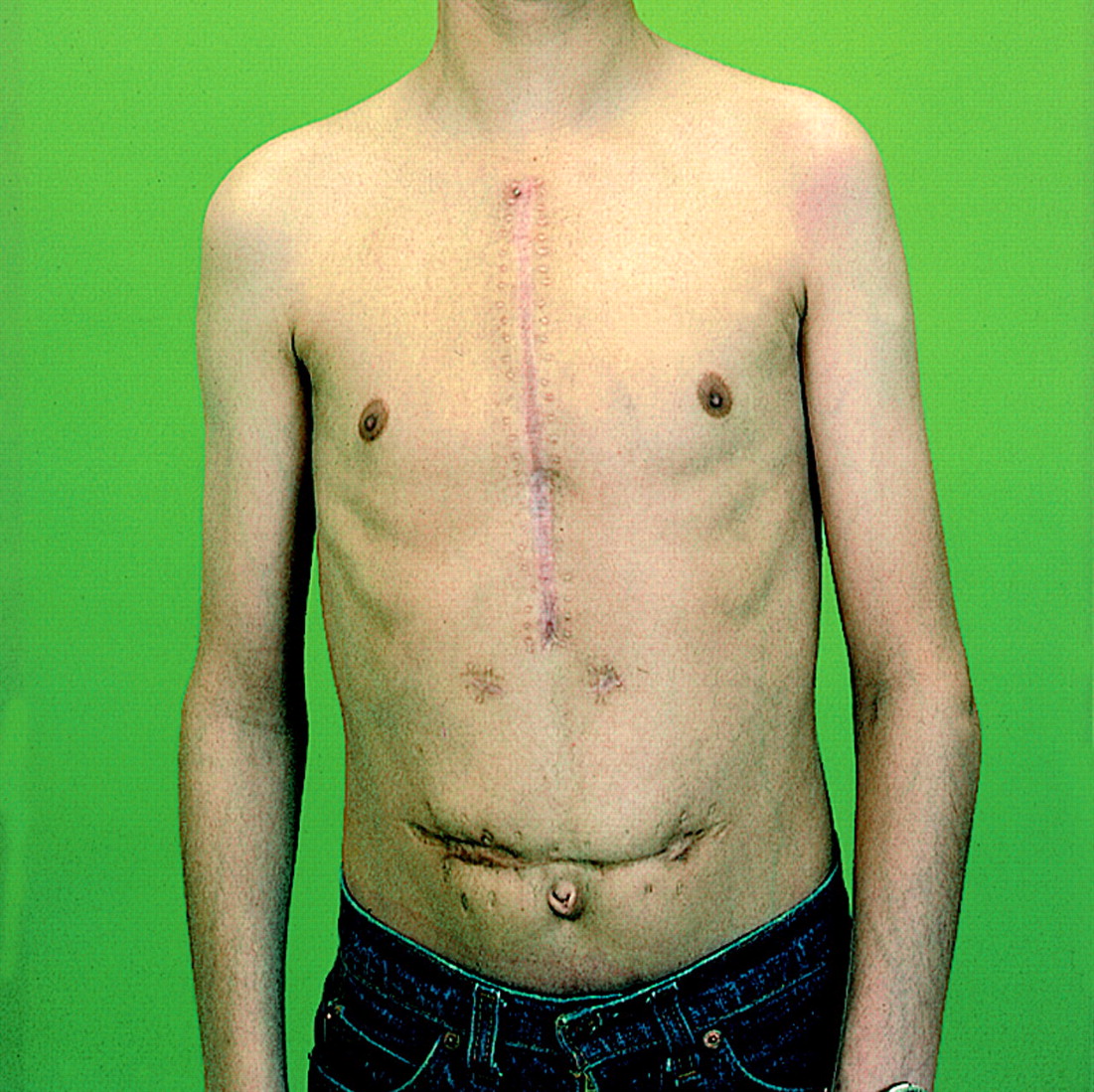
The signs are predominantly right sided and congestive, a high jugular venous pressure with prominent X and Y descents, hepatomegaly, and peripheral oedema. There may be ascites. The heart is small and quiet with a sharp early third heart sound, which may be confused with pulmonary closure (fig 2).
{kind=link}
{kind=link}
Constrictive pericarditis caused by infection presented 10 years after operation to relieve ileal atresia as a neonate. The patient had developed septicaemia as an infant but purulent pericarditis had not been recognised.
Differentiation from a restrictive cardiomyopathy is not usually difficult as in cardiomyopathy the left sided diastolic pressures are usually much higher than those on the right, unless there is considerable tricuspid regurgitation. The latter is rare in constrictive pericarditis.
Differential diagnosis of constrictive pericarditis
Primary restrictive cardiomyopathy
pulmonary congestion
pulmonary hypertension and tricuspid regurgitation with large right (and left) atrium
Amyloid heart disease
absent third sound (until very advanced)
low ECG voltage
thickening of myocardium on echo
In amyloid heart disease a left ventricular third sound is not heard because slow ventricular filling continues through diastole, except in very advanced cases who develop a restrictive physiology. Echocardiography quickly differentiates.
Pericarditis is common in the connective tissue diseases. Acute pericarditis is occasionally the presenting manifestation in Still's disease, when the presence and persistence of severe constitutional symptoms and development of arthritis make the diagnosis clear. Acute pericarditis is common in systemic lupus, particularly during acute flares, and in the Churg-Strauss variant of polyarteritis, but is usually painless in rheumatoid arthritis. Constriction may occur in any of these disorders but is most often seen in association with rheumatoid arthritis because of its greater prevalence.
A number of drugs can induce a lupus syndrome with pericarditis. The best known example is with hydralazine, but it may also be caused by procainamide, methyldopa, and minoxidil. It is reversible on stopping the drug.