


ABSTRACT
OBJECTIVE To compare the effectiveness and toxicity of semisynthetic penicillins (SSPs) (amoxicillin, ampicillin, pivampicillin) and trimethoprim-based regimens (trimethoprim, trimethoprim-sulfamethoxazole, trimethoprim-sulfadiazine) in treating acute bacterial exacerbations of chronic bronchitis (ABECB).
DATA SOURCES We searched MEDLINE, EMBASE, Current Contents, and the Cochrane Central Register of Controlled Trials to identify and extract data from relevant randomized controlled trials (RCTs).
STUDY SELECTION Only RCTs comparing penicillins with trimethoprim-based regimens for the treatment of patients with ABECB that reported data on effectiveness, toxicity, or mortality were considered eligible for this meta-analysis.
SYNTHESIS Out of 134 RCTs identified in the search, 5 RCTs involving 287 patients were included in the analysis. There were no differences between patients with ABECB treated with SSPs and those treated with trimethoprim, alone or in combination with a sulfonamide, in treatment success (intention-to-treat patients: n = 262, odds ratio [OR] 1.68, 95% confidence interval [CI] 0.91–3.09; clinically evaluable patients: n = 246, OR 1.59, 95% CI 0.79–3.20) or number of drug-related adverse events in general (n = 186 patients, OR 0.37, 95% CI 0.11–1.24), frequency of diarrhea or skin rashes, or number of withdrawals due to adverse events (n = 179 patients, OR 0.27, 95% CI 0.07–1.03).
CONCLUSION Based on limited evidence leading to wide CIs of the estimated treatment effects, SSPs and trimethoprim-based regimens seem to be equivalent in terms of effectiveness and toxicity for ABECB.
Studies show that administration of antimicrobial agents leads to reduction in mortality associated with acute bacterial exacerbations of chronic bronchitis (ABECB).1 However, the best antimicrobial agent to use in this patient population is not clear. Trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline, and semisynthetic penicillins (SSPs) such as amoxicillin have been recommended by the Canadian Thoracic Society and Canadian Infectious Diseases Society as first-line agents for patients with ABECB.2 The European Respiratory Society, however, does not include TMP-SMX in the relevant guidelines.3 The objective of this meta-analysis was to compare the effectiveness and safety of the SSPs (amoxicillin, ampicillin, pivampicillin) with trimethoprim (TMP) alone or in combination for ABECB.
METHODS
Literature search and study selection
The methods regarding data sources, study selection, data extraction, definitions, and statistical analysis used for this study have been described in more detail in another meta-analysis performed by our research team comparing the outcomes of patients with ABECB treated with quinolones, macrolides, or amoxicillin–clavulanic acid.4 The literature search included PubMed and the Cochrane Central Register of Controlled Trials until July 2006 (without limit on the start date of the search). The literature search of EMBASE revealed only nonrandomized comparative trials. The key words used to identify the appropriate randomized controlled trials (RCTs) for our meta-analysis were chronic bronchitis, acute exacerbations of chronic bronchitis, antibiotics, amoxicillin, ampicillin, trimethoprim/sulfamethoxazole, and doxycycline. Only RCTs comparing penicillins with TMP alone or in combination for the treatment of patients with ABECB that reported data on effectiveness, toxicity, or mortality were considered eligible for this meta-analysis.
Data extraction
Two investigators (K.G.M. and I.I.S.) independently performed the literature search, study selection, and data extraction. Treatment success was analyzed in the intention-to-treat (ITT) and clinically evaluable (CE) groups of patients included in the RCTs, while toxicity of the regimens administered and withdrawals because of the study drugs were analyzed only in the ITT patients. In addition, the 2 reviewers independently evaluated the methodologic quality of each RCT by assessing the following components: randomization, generation of random numbers, details of double-blinding procedures, information on withdrawals, and concealment of allocation. One point was awarded for the specification of each criterion; the maximum score for a study was 5. Those RCTs that scored more than 2 points were considered high-quality studies (those RCTs that scored 2 or fewer points were considered low-quality studies) according to a modified Jadad score.5
Data analysis and statistical methods
Statistical analysis was performed using S-PLUS 6.1 software. The heterogeneity of RCTs was assessed by using the I2 test.6 Publication (sample size) bias was assessed by the funnel plot method using the Egger test.7 Pooled odds ratios (ORs) and 95% confidence intervals (CIs) for all primary and secondary outcomes were calculated by using both the Mantel-Haenszel fixed-effect8 and the DerSimonian-Laird random-effects9 models. For all analyses, results from the fixed-effect model (FEM) are presented only when there was no heterogeneity between RCTs; otherwise, results from the random-effects model (REM) are presented.
RESULTS
Figure 1 summarizes the study selection process for our meta-analysis. Through researching the electronic databases, we identified 134 potentially relevant RCTs, of which 129 RCTs did not meet the inclusion criteria for our analysis mainly because they compared antimicrobial agents other than penicillins and TMP. Thus, there were 5 RCTs available for further data extraction and analysis.10–14

Study selection
The characteristics and outcomes of the 5 trials included in our meta-analysis are presented in Tables 1 and 2, respectively.10–14 The mean quality score of the analyzed trials was 2.2 (range 0–4), and mean sample size was 57 (range 30–100). All included trials were published in or before 1995. Four of the studies examined hospitalized patients with ABECB; the other10 studied only ambulatory patients. The administered SSP was amoxicillin in 3 trials10,11,14 (compared with TMP-SMX in 2 trials10,14 and TMP in 1 trial11), pivampicillin-pivmecillinam (compared with TMP-SMX) in 1 trial,12 and ampicillin (compared with TMP-sulfadiazine [SDZ]) in the remaining trial.13
All antibiotics were administered orally.
Trials compared broad-spectrum semisynthetic penicillins with trimethoprim alone or in combination with a sulfonamide.
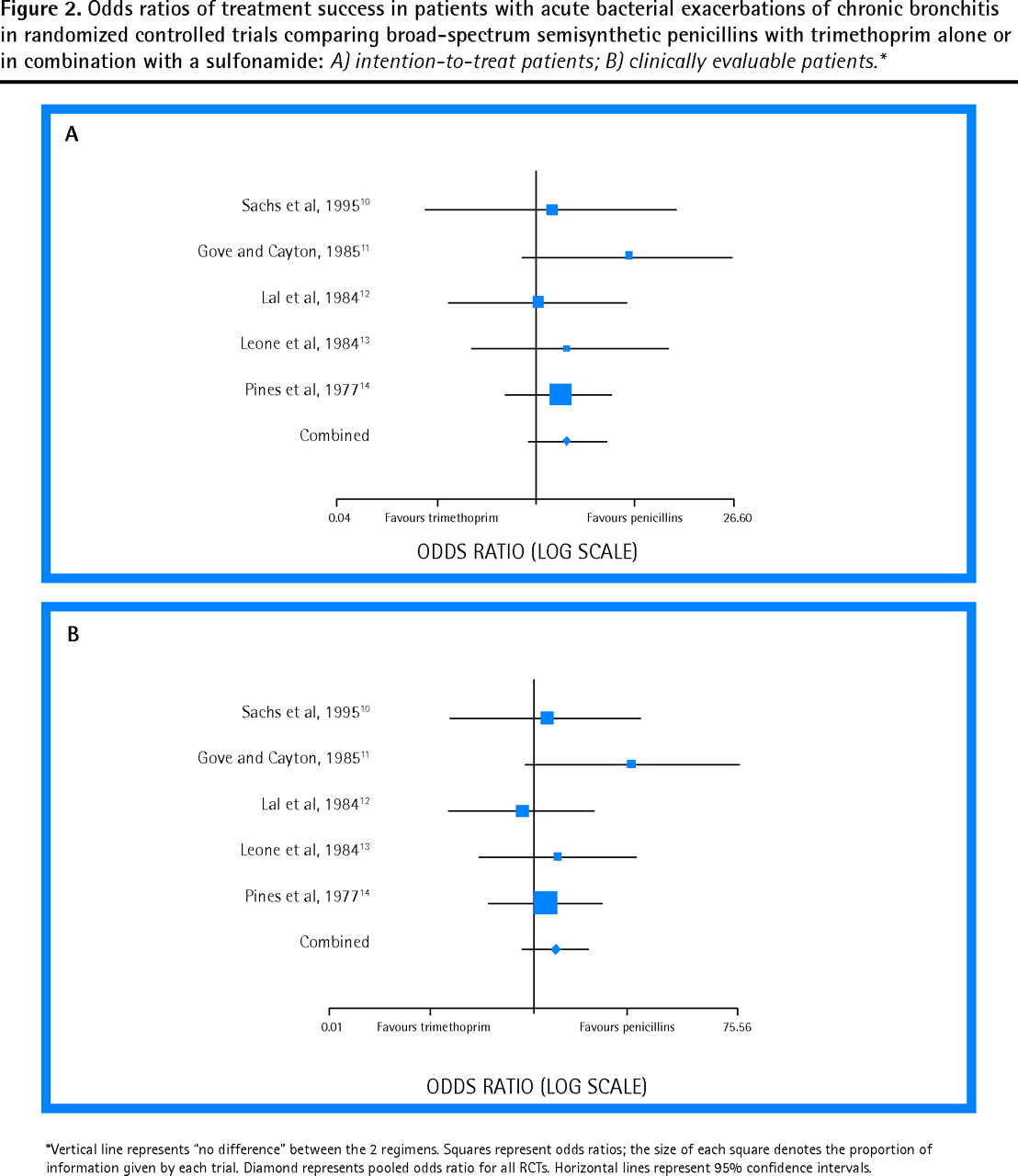
Data on treatment success in both ITT and CE patients with ABECB were reported for all RCTs included in our meta-analysis.10–14 There was no difference in this outcome between SSPs and TMP alone or in combination with a sulfonamide (ITT: n = 262, OR 1.68, 95% CI 0.91–3.09; CE: n = 246, OR 1.59, 95% CI 0.79–3.20, FEM, data from 5 trials10–14). The ORs for the treatment success of the antibiotics compared for the ITT and CE patients in the individual RCTs, as well as the pooled OR, are presented in Figure 2.10–14 Two subset analyses we performed showed no difference in treatment success for CE patients with ABECB treated with amoxicillin compared with those treated with TMP or TMP-SMX (CE: n = 168, OR 1.95, 95% CI 0.80–4.75, FEM, data from 3 trials10,11,14), as well as between those receiving SSPs and those receiving TMP-SMX (CE: n = 181, OR 1.12, 95% CI 0.47–2.67, FEM, data from 3 trials10,12,14).

A) intention-to-treat patients; B) clinically evaluable patients.*
Relevant data about drug-related adverse events were provided for 3 trials included in our analysis.11,12,14 In the remaining 2 trials,10,13 no relevant information was provided; in 1 of these13 the authors stated only that no clinically important adverse events occurred during the study period.
Administration of SSPs for the treatment of patients with ABECB was not associated with more drug-related adverse events in general (ITT: n = 186, OR 0.37, 95% CI 0.11–1.24, FEM, data from 3 trials11,12,14) neither with more episodes of diarrhea (Lal et al12: 0/25 (0%) vs 0/24 (0%), P > .99 by Fisher exact test; Pines et al14: 1/50 (2%) vs 2/50 (4%), P > .99 by Fisher exact test) nor with more episodes of skin rash (Gove and Cayton11: 1/18 (6%) vs 0/19 (0%), P = .486 by Fisher exact test; Pines et al14: 1/50 (2%) vs 4/50 (8%), P = .362 by Fisher exact test) compared with administration of TMP alone or in combination with a sulfonamide. We found no difference in withdrawals due to drug-related adverse events between the studied therapeutic regimens (ITT: n = 179, OR 0.27, 95% CI 0.07–1.03, FEM, data from 3 trials12–14). Finally, data on mortality were available only for 1 trial11 (patients who died among those treated with amoxicillin and those treated with TMP: 1/18 [6%] vs 2/19 [11%], P > .99 by Fisher exact test).
DISCUSSION
The findings of this meta-analysis of the limited available evidence show SSPs (amoxicillin, ampicillin, and pivampicillin) and TMP-based regimens are equivalent with regard to effectiveness and toxicity for the treatment of patients with ABECB.
The Canadian Thoracic Society and the Canadian Infectious Disease Society have recommended SSPs (mainly amoxicillin), TMP-SMX, and doxycycline for the management of patients with ABECB.2 Thus, the comparison of doxycycline with TMP-SMX or SSP also seems to be clinically important. Unfortunately, there are not enough trials comparing doxycycline with these agents to perform meaningful meta-analyses. In fact, we found only 3 RCTs that compared doxycycline with another (not first-line) antimicrobial agent for the treatment of patients with ABECB (specifically with amoxicillin– clavulanic acid,15 roxithromycin,16 and spiramycin17).
Trimethoprim, a diaminopyrimidine congener, is usually combined with a sulfonamide to achieve a synergistic antibacterial effect, as both agents act on bacterial synthesis.18 Trimethoprim-sulfamethoxazole was found not to be bactericidal in chronic respiratory infections,19 whereas intrabronchial concentrations of amoxicillin and of other SSPs remain bactericidal as long as the antimicrobial agent is given for the treatment of such infections.20 Thus, administration of SSPs should result in better eradication rates of Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis than administration of TMP-SMX would. Lack of specific data regarding this microbiological outcome in the RCTs included in our analysis did not allow us to further evaluate this issue. Some might support the view that persistence of bacteria after resolution of the initial episode of ABECB influences the frequency of additional exacerbations,21 and thus SSPs are likely to be associated with fewer recurrences of ABECB than TMP-SMX. Unfortunately, relevant data were provided in only 1 trial14 in which more patients treated with amoxicillin exhibited no recurrence during the 1-month period after therapy for the initial episode than patients treated with TMP-SMX (28/39 [72%] vs 12/35 [34%], P = .002 by Fisher exact test).
Diarrhea and skin rash are among the most common adverse effects of both SSP and TMP-SMX; their frequency did not differ between the comparison groups in our meta-analysis. There is evidence that most adverse effects of TMP-sulfonamide combinations are caused by the sulfonamide moiety, as a result of its high dose.22 It is important to note that potentially fatal adverse events of TMP-SMX, such as blood dyscrasias,23 were not reported in the trials included in our meta-analysis.
Limitations
We acknowledge that several limitations affect the value of our meta-analysis. First, the small number of identified RCTs, as well as their relatively small sample sizes, could be inadequate to reveal a difference in outcomes of patients treated with SSPs or TMP-based regimens. Second, we included trials that examined different medications. The sulfonamides SMX and SDZ do not, however, differ in the spectrum of their antibacterial activity or in their synergistic potentiation with TMP.24 In addition, both sulfonamides penetrate bronchial secretions poorly and, consequently, have limited antibacterial effects compared with TMP, which is found in good concentrations in bronchial secretions.25 Third, all trials included in this analysis were performed in or before 1995. Since then the patterns of antimicrobial resistance among pathogens causing ABECB have changed and, thus, the findings might not be fully applicable in several countries. There are serious concerns that TMP-SMX and SSPs now have limited in vitro activity against the main pathogens in ABECB (S pneumoniae, H influenzae, and M catarrhalis) because of the emergence of resistance in these pathogens.26 The findings might be of value, however, in countries with low antimicrobial resistance among S pneumoniae, H influenzae, and M catarrhalis, such as The Netherlands, the Nordic countries, and Canada (especially in “antibiotic-naïve” patients like immigrants, who comprise a considerable proportion of the Canadian population).
Fourth, concomitant interventions for the management of ABECB, such as administration of systemic corticosteroids or bronchodilators, that might act as confounding factors when evaluating the effectiveness of the antimicrobial agents were not standardized in the individual RCTs. Indeed, in 4 of 5 trials11–14 included in the analysis, data on use of systemic corticosteroids were not available; in the remaining trial10 use of corticosteroids before ABECB was an exclusion criterion. Fifth, the selected RCTs did not provide data regarding quality of life and time to next exacerbation, which are important considerations in the management of patients with ABECB. Sixth, as depicted in detail in Table 1, there were differences in dosages of the study drugs as well as in treatment duration. Finally, it should be stressed that current guidelines do not advocate the use of antibiotics in patients with Anthonisen type II (presence of only 2 of the following symptoms: increased dyspnea, sputum volume, and sputum purulence) ABECB without purulence or patients with Anthonisen type III (none or 1 of the above symptoms) ABECB.3
One might argue that our analysis is limited by methodologic weaknesses of the included RCTs. Indeed, selected trials provided data mainly for CE and not for ITT patients. In addition, we could not preclude any possibility of underreported adverse effects of evaluated antibiotics.
Conclusion
Despite these limitations, we think that our study offers potentially useful data that might be of value to clinicians caring for patients with ABECB in countries with low antimicrobial resistance among S pneumoniae, H influenzae, and M catarrhalis strains. The limited evidence from the available RCTs shows no difference between SSPs and TMP-based regimens regarding effectiveness and toxicity for the treatment of patients with ABECB. We do emphasize, however, that the limited evidence from available RCTs leads to wide CIs of the estimated treatment effects. Thus, the presence of a difference between the compared regimens for ABECB cannot be excluded, especially in favour of SSPs after taking into account the estimated ORs for the various outcomes we analyzed.
Notes
EDITOR’S KEY POINTS
-
Because semisynthetic penicillins (SSPs) and regimens containing trimethoprim (TMP) have both been recommended for acute bacterial exacerbations of chronic bronchitis, it is not clear which is the best antimicrobial agent to use.
-
The objective of this meta-analysis was to compare the effectiveness and safety of the SSPs (amoxicillin, ampicillin, pivampicillin) with trimethoprim-based regimens for this indication.
-
The limited available evidence shows SSPs and trimethoprim-based regimens to be equivalent in effectiveness and toxicity for treatment of patients with acute bacterial exacerbations of chronic bronchitis. Because of the wide confidence intervals of the estimated treatment effects, however, the possibility of a difference between the compared regimens cannot be excluded.
POINTS DE REPÈRE DU RÉDACTEUR
-
Les pénicillines semi-synthétiques (PSS) et les préparations contenant du triméthoprime (TMP) sont toutes deux recommandées pour les exacerbations bactériennes de la bronchite chronique, mais on ne sait trop lequel de ces antimicrobiens est le meilleur.
-
Cette méta-analyse avait pour objectif d’établir laquelle entre les PSS (amoxicilline, ampicilline, pivampicilline) et les préparations à base de triméthoprime avait les meilleures efficacité et innocuité pour cette indication.
-
Les quelques données probantes disponibles montrent que les PSS et les préparations à base de TMP ont des efficacités et toxicités équivalentes pour traiter les exacerbations bactériennes de la bronchite chronique. Toutefois, parce que les effets estimés des traitements ont de larges intervalles de confiance, on ne peut exclure la possibilité d’une différence entre les traitements comparés.
Footnotes
-
Contributors
Drs Manta and Siempos performed the literature search, study selection, and data extraction. All authors contributed to concept and design of the study, analysis and interpretation of the studies, and preparing the manuscript for submission.
-
Competing interests
None declared
-
This article has been peer reviewed.
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}