


ABSTRACT
OBJECTIVE To evaluate the clinical observation that the number of individuals seeking opioid detoxification from oxycodone was increasing at the Centre for Addiction and Mental Health (CAMH) in Toronto, Ont; and to identify the characteristics of individuals seeking opioid detoxification at CAMH.
DESIGN Retrospective analysis of patient health records.
SETTING Medical Withdrawal Management Service at CAMH.
PARTICIPANTS All patients admitted for opioid detoxification between January 2000 and December 2004.
MAIN OUTCOME MEASURES Number of opioid detoxification admissions each year; type, dose, and source of opioids; comorbid problems and symptoms.
RESULTS There were 571 opioid detoxification admissions during the 5-year study period. The number of admissions increased steadily over the 5 years; in particular, the number of admissions related to controlled-release oxycodone increased substantially (3.8%, 8.3%, 20.8%, 30.6%, and 55.4% of the total opioid admissions in 2000 to 2004, respectively; χ42= 105.5, P < .001). The rates of admissions involving heroin remained low and stable. Use of controlled-release oxycodone was associated with considerably higher doses than use of other prescription opioids was. Physician prescriptions were the source of the prescription opioids for a large percentage of patients, particularly for older patients. Prescription opioid users reported considerable comorbid substance use problems, pain, and psychiatric symptoms.
CONCLUSION This study has demonstrated a significant rise in the number of individuals seeking treatment at CAMH for controlled-release oxycodone addiction. The substantial comorbid pain, psychiatric symptoms, and other psychoactive substance use problems in these patients, coupled with the finding that prescriptions were an important source of opioids, highlight the clinical complexities encountered in the treatment of these individuals. Further research examining these complexities and the many possible pathways leading to prescription opioid addiction is required in order to develop effective prevention and treatment strategies.
Prescription opioids are an important therapeutic option in clinical practice and bring important improvements to quality of life in the treatment of pain. Most opioids, however, are potentially addictive. In fact, it appears that the abuse of prescription opioids might have become the predominant form of illicit opioid use in Canada.1 Very little is known about prescription opioid abuse, particularly the characteristics of this use and of the individual users. The Centre for Addiction and Mental Health (CAMH) in Toronto, Ont, has been treating a large number of prescription opioid–addicted individuals, providing an opportunity to investigate this population. Affiliated with the University of Toronto, CAMH is Canada’s leading addiction and mental health teaching and research hospital. Through one of its founding partners, the Addiction Research Foundation, CAMH has been operating a methadone maintenance treatment program since 1970. An increase in prescription opioid–addicted treatment seekers was first noticed in the 1990s, with the expansion of the methadone maintenance treatment program. Traditionally, methadone maintenance programs serviced primarily heroin users requiring opioid substitution treatment. In a review of the 178 patients who were admitted to the program between 1997 and 1999, it was found that 24% had used prescription opioids only, 24% had used prescription opioids initially then heroin, 35% had used heroin first and prescription opioids later, and only 17% had used heroin only.2 Codeine and oxycodone were the primary prescription opioids used by these individuals. Since a controlled-release oxycodone product became available in 1995, the numbers of individuals seeking treatment for oxycodone addiction in particular appeared to be increasing at CAMH. To evaluate this clinical observation, this study was undertaken to identify the characteristics of individuals seeking opioid detoxification at CAMH over a 5-year period.
METHODS
The Medical Withdrawal Management Service is an inpatient service at CAMH for patients who require 24-hour nursing and medical care to withdraw from their substances of abuse. Patients are referred to the service from the greater Toronto area and across Ontario. This study was conducted through a retrospective analysis of patients’ medical charts. The study was approved by the CAMH Research Ethics Board and by the Health Canada Research Ethics Board.
The project included all patients admitted to CAMH’s Medical Withdrawal Management Service seeking treatment for opioid detoxification between January 2000 and December 2004. There were no exclusion criteria. For any patient who had multiple admissions during this period, only the most recent admission was included in subsequent analyses. Two research analysts, trained by the investigators, retrieved the following information from the medical charts using standardized data collection forms: demographics, opioid use (including types and sources), current use of other psychoactive substances reported by the patient to be a problem, and medical and mental health complaints indicated in the chart to be part of the current clinical picture. More detailed reviews were conducted for patients admitted in 2004, including opioid doses, patterns of use, and age at first use. Prescription opioid doses were expressed as oxycodone equivalents based on approximate equianalgesic oral doses.3 Descriptive statistics were calculated using SPSS version 12.0. Pearson χ2 was used to compare the proportion of admissions related to controlled-release oxycodone with the proportion of admissions related to other opioids.
RESULTS
From 2000 to 2004, there were 571 opioid detoxification admissions. The number of admissions increased steadily over the 5 years. In particular, the number of admissions related to controlled-release oxycodone increased substantially (n = 3 [3.8% of total opioid admissions], n = 8 [8.3%], n = 25 [20.8%], n = 34 [30.6%], and n = 92 [55.4%] from 2000 to 2004, respectively; χ42 = 105.5, P < .001). The other opioids involved in these admissions included other oxycodone products (acetaminophen-oxycodone combinations); other pharmaceutical opioid products; and heroin (Figure 1). The other pharmaceutical opioid products were primarily codeine (n = 201), morphine (n = 116), hydromorphone (n = 43), and meperidine (n = 13). Rates of admissions involving heroin remained low and stable. Some admissions involved more than 1 problem opioid.

The number of admissions increased over the 5 years (2000, n = 78; 2001, n = 96; 2002, n = 120; 2003, n = 111; and 2004, n = 166). Of the 571 admissions, 295 involved 1 opioid, 204 involved 2 opioids, 68 involved 3 opioids, and 4 involved 4 opioids.
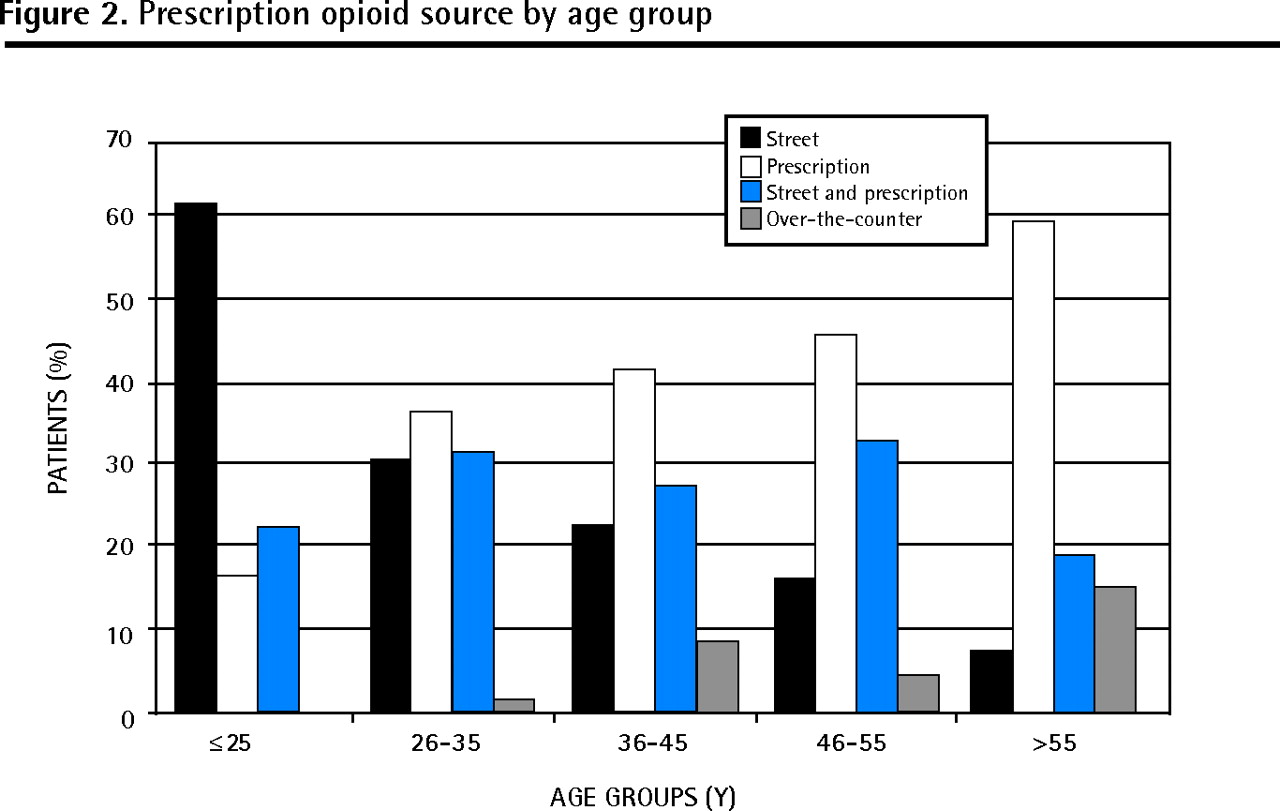
Of the 571 admissions, 295 involved 1 opioid, 204 involved 2 opioids, 68 involved 3 opioids, and 4 involved 4 opioids. Of the 571 admissions, 62 patients had multiple admissions; therefore only the most recent admission was included for each of these patients in the subsequent analyses. The study sample consisted of 499 unique cases. Of these, those using prescription opioids (n = 428) had a mean age of 41.3 (SD 9.7) years (range 20 to 81 years); 56% were men and 44% were women; and 60% were unemployed. The sources of prescription opioids were doctors’ prescriptions (37%), the street (21%), a combination of prescriptions and the street (26%), non-prescription (ie, codeine formulations) purchase (5%), and friends or family (1%). The data show a clear linear trend between age and source: the likelihood of obtaining drugs from the street decreased with age while the likelihood of obtaining them from physicians increased with age (Figure 2). There were substantial pain (eg, 31% reported back pain, 18% reported headache) and psychiatric (eg, 53% reported depressive symptoms, 25% reported anxiety) symptoms associated with these prescription opioid users. Many individuals also had self-reported problem use of other substances (eg, 45% also abused alcohol, 43% used benzodiazepines, 30% used cocaine, and 27% used cannabis).

Prescription opioid source by age group
The more detailed chart review of the 2004 admissions (n = 166) consisted of 155 patients after removing multiple admissions; 84 of these were related to use of controlled-release oxycodone (Table 13). The daily doses associated with controlled-release oxycodone were higher (mean 398 mg) than for the other prescription opioid products (mean 101 to 159 mg oxycodone equivalents), and the duration of regular use of controlled-release oxycodone was shorter (mean 2.2 years compared with means of 5 to 6 years for other opioids). Controlled-release oxycodone was most likely to be associated with product manipulation, primarily chewing the product (73.8%), but also crushing and snorting (13.1%) or crushing and injecting (13.1%). Heroin was most likely to be used by injection (77.8%); however, a substantial proportion of nonoxycodone prescription opioid users also injected the drugs (22.8%). The mean age at first use was younger for heroin users than for prescription opioid users.
N = 155.*
DISCUSSION
An increasing number of individuals addicted to prescription opioids have been seeking detoxification assistance at CAMH. The most significant increase has been in the number of controlled-release oxycodone users seeking treatment, whereas the number of heroin users seeking treatment has remained constant and low. Controlled-release oxycodone use was associated with considerably higher daily doses than other prescription opioids were. The duration of use of controlled-release oxycodone was shorter than for other prescription opioids, which might reflect the comparatively recent arrival of this drug on the Canadian market. Physician prescriptions were the source of prescription opioids for a large percentage of the patients in this study, with the percentage increasing in older age groups. It was not possible to further delineate legitimate prescriptions from those obtained through fraudulent means (eg, doctor scamming). These prescription opioid users reported considerable comorbidity, including other substance use problems, pain, and psychiatric symptoms.
This study adds to the increasing literature on prescription opioid abuse. Most studies to date have focused on the prevalence of the problem, primarily in the United States,4–6 with less information available about the characteristics of the users and their use of these opioids, especially in Canada. Previous data from CAMH indicate that codeine and oxycodone have been commonly abused prescription opioids.2,7,8 The controlled-release formulation of oxycodone is available in higher doses (10- to 80-mg tablets) than the immediate-release oxycodone formulations (5-mg tablets). Controlled-release preparations were expected to have a lower abuse potential because it was suggested that users would be less likely to experience the euphoria associated with high concentrations of the drug rapidly reaching the brain. However, a substantial proportion of the oxycodone dose in controlled-release formulations is released immediately, with the rest released more slowly.9 In addition, abusers often report crushing or chewing these preparations before swallowing, snorting, or injecting, thereby destroying the slow-release properties. Results from the US National Household Survey on Drug Abuse (2000–2001) showed that nonmedical controlled-release oxycodone users (n = 553) were more likely to have indications of abuse of or dependence on prescription opioids compared with nonmedical users of other prescription opioids (n = 12 039) (20.1% vs 3.5%, respectively).10
With the rise in abuse of controlled-release oxycodone, there have been a few studies specifically aimed at identifying the characteristics of this population. These studies have also demonstrated a pattern of problems with multiple opioids and other substances, substantial pain, and psychiatric comorbidities.11–14 The primary source of prescription opioids varies in these reports. For example, the source of controlled-release oxycodone was primarily from the street in a study conducted in Kentucky12,13; yet in a report from the Researched Abuse, Diversion and Addiction-Related Surveillance System, which used a key informant network across the United States, 70% of the controlled-release oxycodone abusers listed prescriptions as their main source.14 Very few studies have characterized abusers of other prescription opioids; however, the presence of polysubstance abuse, pain, and psychiatric comorbidities are consistent findings,15,16 even in studies conducted before the advent of controlled-release oxycodone.7,8,17
Limitations and areas for further study
The limitations of this study are those of any retrospective chart review. Potential inaccuracies in the reporting and documentation in the clinical record are inherent concerns in this type of research. However, the primary physician for these admissions was one of the authors (L.C.B.), which provided continuity in the clinical documentation. In addition, the large sample size covering all admissions over a 5-year period provides a reasonable picture of the changing patterns of drug use, particularly related to controlled-release oxycodone use, in this population. The population of opioid abusers in this study might not necessarily represent other opioid-abusing populations, including those not seeking treatment or those seeking other types of treatment.
The natural history of prescription drug abuse and the relationship of abuse and addiction to the clinical management of patients who are prescribed these agents for legitimate medical conditions require further study.18,19 The substantial comorbid pain, psychiatric conditions, and other psychoactive substance use problems highlight the clinical complexities encountered in the treatment of these individuals. The significant rise in individuals addicted to controlled-release oxycodone seeking treatment has focused these concerns and has helped bring the issue of prescription opioid abuse to the fore. Many clinicians tend to divide patients into 2 categories: individuals with legitimate pain and substance abusers “scamming” to obtain drugs. The clinical reality is much more complex, as pain and substance abuse are not mutually exclusive. This retrospective analysis was not able to fully explore the relationships between prescription opioid use and comorbidities, but this line of research is critical. It underlies the key difference between prescription drug abuse and other substance abuse: some individuals can be and might need to be exposed to these substances therapeutically. Initial work exploring first exposures to prescription opioids in a population of prescription opioid abusers in a methadone maintenance treatment program indicated a relationship between previous substance use and continued use of prescription opioids following initial therapeutic exposure.20 The health care system is inextricably linked to this problem as a source of the drugs, and therefore a potential enabler, but also as a solution.
Conclusion
This study has demonstrated a significant rise in individuals addicted to controlled-release oxycodone seeking treatment at CAMH. This has helped bring the issue of prescription opioid abuse to the fore. The significant comorbid pain, psychiatric conditions, and other psychoactive substance use problems in these patients, coupled with the finding that prescriptions were an important source of opioids, highlights the clinical complexities encountered in the treatment of these individuals. Further research, including prospective studies, examining these complexities and the many possible pathways leading to prescription opioid addiction is required in order to develop effective prevention and treatment strategies.
Acknowledgment
This study was supported by the Drug Strategy and Controlled Substances Programme of the Office of Research and Surveillance at Health Canada.
Notes
EDITOR’S KEY POINTS
-
This study identifies the characteristics of individuals seeking opioid detoxification at the Centre for Addiction and Mental Health in Toronto, Ont.
-
From 2000 to 2004, the number of admissions increased steadily each year, while the number of admissions related to controlled-release oxycodone increased substantially. The main source of prescription opioids was doctors’ prescriptions, followed by the street and a combination of prescriptions and the street; the likelihood of obtaining drugs from the street decreased with age, while the likelihood of obtaining them from a physician increased with age.
-
Before their introduction, controlled-release preparations were expected to have a lower abuse potential because users would be less likely to experience the euphoria associated with high concentrations of the drug rapidly reaching the brain. Many abusers, however, reported crushing or chewing these preparations before swallowing, injecting, or snorting them, thereby destroying the slow-release properties.
POINTS DE REPÈRE DU RÉDACTEUR
-
Cette étude détermine les caractéristiques des personnes venues au Center for Addiction and Mental Health de Toronto pour sevrage des opiacés.
-
Entre 2000 et 2004, le nombre d’admissions annuelles a augmenté régulièrement, tandis que celui des admissions en lien avec l’oxycodone à libération contrôlée augmentait de façon substantielle. Les opiacés sur ordonnance avaient comme principale source les prescriptions médicales, suivies par la rue et une combinaison de prescriptions et de rue; la probabilité d’obtenir les drogues dans la rue diminuait avec l’âge, tandis que celle de les obtenir d’un médecin augmentait avec l’âge.
-
Avant leur introduction, on croyait que les préparations à libération contrôlée auraient un plus faible potentiel d’abus parce que les utilisateurs seraient moins susceptibles de ressentir l’euphorie causée par l’arrivée de fortes concentrations de drogue au cerveau. Toutefois, plusieurs toxicomanes ont avoué écraser ou mâcher ces préparations avant de les avaler, de les injecter ou de les priser, annulant ainsi leurs propriétés de libération lente.
Footnotes
-
*Full text is available in English at www.cfp.ca.
-
Contributors
Dr Sproule was the principal investigator responsible for the project and she contributed substantially to the conception and design of the study, analysis and interpretation of the data, and preparation of the article. Dr Brands contributed substantially to the conception and design of the study and interpretation of the data and critically appraised the article for intellectual content. Ms Li contributed substantially to the data acquisition and analysis. Dr Catz-Biro contributed substantially to the conception and design of the study and interpretation of the data and critically appraised the article for intellectual content.
-
Competing interests
None declared
-
This article has been peer reviewed.
- Copyright© the College of Family Physicians of Canada
Reference List
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Oxycodone: A Current Perspective on Its Pharmacology, Abuse, and Pharmacotherapeutic Developments
- Early detection of patients with narcotic use disorder using a modified MEDD score based on the analysis of real-world prescription patterns
- Improving wait time from referral to opiate replacement therapy in a drug recovery service
- Neonatal opioid withdrawal and antenatal opioid prescribing
- Controlling pain and reducing misuse of opioids: Ethical considerations
- Controler la douleur et reduire l'usage abusif d'opioides: Questions d'ethique
- Lignes directrices canadiennes sur l'utilisation securitaire et efficace des opioides pour la douleur chronique non cancereuse: Resume clinique pour les medecins de famille. Partie 2: populations particulieres
- Canadian guideline for safe and effective use of opioids for chronic noncancer pain: Clinical summary for family physicians. Part 2: special populations
- Pharmacists' experiences with dispensing opioids: Provincial survey
- Nonmedical use of opioid analgesics among Ontario students
- La douleur d'un marina: Troubles musculosquelettiques, douleur chronique et invalidite chez les veterans militaires
- A sailor's pain: Veterans' musculoskeletal disorders, chronic pain, and disability