


Answer to Ophthaproblem continued from page 489
3. Thyroid orbitopathy
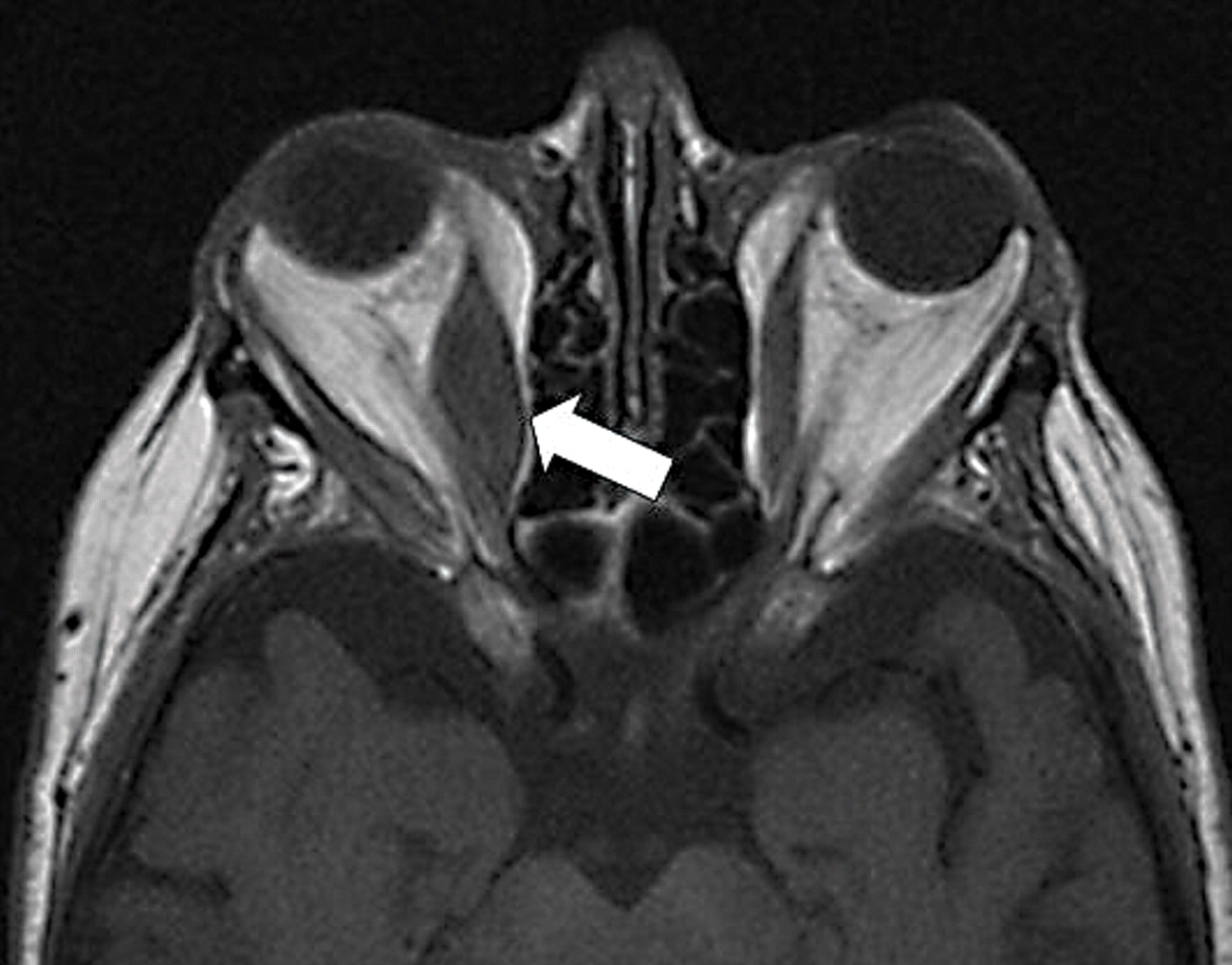
Figure 1 represents an axial, T1-weighted image of the orbits of a patient with thyroid orbitopathy (TO). There is marked enlargement of the right medial rectus muscle, with sparing of the tendinous sheath. Thyroid orbitopathy is usually associated with Graves disease and hyperthyroidism. Nonetheless, a substantial number of patients (20%) with TO are, in fact, clinically euthyroid.1 The prevalence of TO is 8 times higher in women than men, and tends to affect those aged 30 to 50 years. Smokers are at 4 times the risk of acquiring TO.2

Orbits of a patient with thyroid orbitopathy
Orbitopathy usually occurs within 18 months (before, after, or during) of the diagnosis of thyroid disease. Thyroid orbitopathy progresses slowly with a variable clinical course before stabilizing and later resolving. The duration of this process is often 18 to 36 months.3
Clinical manifestations
The triad of TO consists of inflammation, edema, and fibrosis of orbital tissues. The most common clinical manifestations are as follows:
Eyelid retraction
Thyroid orbitopathy is the most common etiology for upper eyelid retraction. It is sometimes incorrectly interpreted as ptosis of the contralateral eye.
Exophthalmos
The most common cause of proptosis in adults is TO.4 Inflammation, edema, and fibrosis of extraocular muscles and connective tissues can all cause axial proptosis. Nonaxial proptosis warrants investigation of other orbital pathologies, such as lymphoma or orbital inflammatory syndrome. Increased resistance to retropulsion also necessitates a computed tomography scan or magnetic resonance imaging to rule out an orbital tumour.
Extraocular muscle (EOM) fibrosis
Diplopia on upward gaze frequently occurs in patients with TO and is caused by fibrosis of the inferior rectus muscle limiting elevation. The second most common EOM fibrosis presentation is impaired lateral gaze due to fibrosis of the medial rectus.
Soft tissue edema
Involvement can include eyelid edema, conjunctival chemosis and injection, and lacrimal gland enlargement.
Corneal exposure
Exposure keratitis results from the combination of eyelid retraction, proptosis, lagophthalmos (inability to completely close eyelids), and lacrimal gland dysfunction. The severity of exposure keratitis varies widely, from subtle inferior punctate staining to corneal ulcers.
Optic neuropathy
The most common cause of blindness from TO is optic neuropathy.5 Patients with symmetric EOM enlargement are at greater risk of optic nerve compression and optic neuropathy.5 These cases do not necessarily involve substantial proptosis; the orbital septum might limit anterior displacement despite high retrobulbar pressures. Relative afferent pupillary defects are present in 35% of cases, while visual field defects are present in 66%.6 Nearly one-fifth of those with optic neuropathy have normal visual acuity (20/20 to 20/25).6 Furthermore, colour-vision tests (eg, Ishihara colour test plates) are helpful; the presence of red desaturation in particular is often an early sign of optic nerve compromise.
Investigations
Patients with suspected TO should first undergo serum thyroid-stimulating hormone (TSH) testing. Hyperthyroidism can be diagnosed with low TSH levels. Second, free thyroxine measurement determines whether or not the thyroid disease is subclinical or overt. Euthyroid individuals (normal TSH levels) with obvious clinical manifestations do not require any additional laboratory tests, as TO can be a clinical diagnosis.
Euthyroid patients with subtle or atypical presentations should undergo an orbital B-scan ultrasound to detect minor muscle enlargement.7 For subtle thyroid eye disease, ultrasound might be more sensitive than computed tomography or magnetic resonance imaging. Thyroid-stimulating hormone antibody tests are helpful but not entirely diagnostic, as TSH antibodies are present in only 50% of cases of euthyroid orbitopathy.8
Management
During the active phase of TO, ophthalmologists should provide counseling and symptomatic treatments and monitor for serious complications, such as exposure keratitis and optic neuropathy, until stabilization and resolution occurs. The active phase typically lasts 12 to 18 months. Without proper patient education and counseling, patients might feel frustrated and abandoned during this period as their symptoms worsen and little definitive treatment is offered. The natural history of stabilization and improvement must be emphasized. Smoking cessation should be encouraged because it reduces orbitopathy progression during radioactive (iodine 131) treatment and improves response of diplopia to prednisone and radiation.9
Patients with Graves disease often see an ophthalmologist before starting iodine 131 therapy, which is associated with a 15% probability of worsening thyroid orbitopathy.10 Steroid prophylaxis can eliminate this risk; however, side effects of prednisone must be discussed with the patient.
Preventing exposure keratitis can usually be managed with ocular lubricants. Severe eyelid retraction can be treated with botulism-toxin injections, although risks of overcorrection can result in ptosis.11
Diplopia is often the primary concern during active TO. High-dose prednisone, with tapering doses, is an effective treatment to reduce inflammation and pressure within the bony orbit. Because treatment and tapering frequently spans several months, patients must understand the side effects and risks of such treatment.
If diplopia cannot be successfully managed with prednisone, low-dose radiation is a valid option. The safety profile of low-dose radiation is superior to that of long-term prednisone. Although the standard low-dose regimen of 2000 rad given over a 2-week period might temporarily cause dry eye syndrome, it is not typically associated with any complications. However, the main drawback of radiation is delayed response. Benefits usually begin 5 to 6 weeks after treatment and continue to improve for up to 3 months. Because of this deferred effect, many treatment plans comprise a combination of prednisone and radiation.
Optic neuropathy monitoring is paramount in TO management. Although less than 5% of patients will experience optic neuropathy with vision loss, it is the leading cause of blindness secondary to TO.12 Risk factors for optic neuropathy include sex (male), age (50 to 70 years), and diabetes.6 Computed tomography scans can determine the degree of compression within the bony orbit. Treatment involves steroids, radiation, and surgical orbital decompression. Optic neuropathy in TO is reversible and vision can be restored with prompt treatment.
The inactive phase of TO includes stabilization and often improvement. Definitive treatment can begin and involves first orbital decompression, then strabismus surgery, and finally correction of eyelid retraction.
Conclusion
Patients with TO are usually hyperthyroid, but up to 20% of them are clinically euthyroid. The clinical course of TO can extend to 3 years, during which monitoring and counseling are key. Optic neuropathy might occur, with normal visual acuity and no proptosis; visual loss is reversible with timely treatment.
Footnotes
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.