


ABSTRACT
OBJECTIVE To characterize hypertension management in an academic family medicine clinic.
DESIGN Cross-sectional chart review.
SETTING Academic family medicine clinic in Edmonton, Alta.
PARTICIPANTS A total of 210 patients with 1 or more visits for hypertension during the previous 3 years.
MAIN OUTCOME MEASURES Patient characteristics, current antihypertensive therapies, most recent blood pressure measurements, and compelling indications according to the 2006 Canadian Hypertension Education Program recommendations.
RESULTS A total of 185 subjects (88%) were prescribed antihypertensive medications, and 89 (42%) had controlled hypertension. Younger subjects, people with diabetes, and people not receiving antihypertensive medication therapy appeared less likely to have controlled hypertension. There were 76 subjects (36%) prescribed 1 antihypertensive medication, 65 subjects (31%) prescribed 2 antihypertensive medications, and 44 (21%) prescribed 3 or more antihypertensive medications. Angiotensin-converting enzyme inhibitors were prescribed for 51% of the subjects, diuretics for 47%, β-blockers for 27%, calcium channel blockers for 23%, angiotensin receptor blockers for 20%, and α-blockers for 1%.
CONCLUSION Hypertension treatment and control rates in this academic family medicine clinic appear to be better than those in the general population. Following the principles of a continuous quality improvement process, this information will serve as an important foundation for identifying areas to improve hypertension management in the clinic.
Hypertension is a leading modifiable risk factor for cardiovascular disease and has been estimated to account for 13% of deaths worldwide.1 There is a direct relationship between blood pressure and risk of cardiovascular disease. For example, as baseline blood pressure increases from below 120/80 mm Hg, there is a stepwise increase in cardiovascular event rates.2 Although hypertension is the most common reason for visiting physicians, accounting for more than 20 million visits to general practitioners and internists in 2006, management of this chronic disease has several challenges.3 The asymptomatic nature of this disease presents a substantial challenge to identifying people with high blood pressure and providing optimal care.4 In addition, the absence of symptoms renders medication adherence even more challenging.5
Despite the challenges, hypertension management has improved dramatically over the past decade, primarily in the areas of increased awareness and treatment.6,7 Most patients, however, do not reach therapeutic goals and continue to be at high risk of cardiovascular events.7 The last Canadian study to measure community rates of hypertension treatment and control was the Canadian Heart Health Study, conducted between 1985 and 1992.8 According to this study, the prevalence of hypertension was 22%; 58% of hypertensive patients were aware of their condition, 39% were being treated, and 16% had controlled hypertension in 1992.8 The Canadian Hypertension Education Program (CHEP) was initiated in 1999 to improve hypertension treatment and control in Canada and appears to have influenced patterns of antihypertensive medication prescription.9,10 The most current North American measurement of hypertension management used the 2003 to 2004 cycle of the United States National Health and Nutrition Examination Survey (NHANES).7 While 76% of hypertensive patients were aware of their condition, only 65% were treated with anti-hypertensive medications and only 37% had controlled hypertension.7
With hypertension management less than ideal, the first step in improving management within a clinic is to compare current practice patterns with external benchmarks, such as recent population-based observations, evidence-based practice guidelines, and clinical trials.11 This objective comparison establishes a foundation for a clinical quality improvement strategy to improve overall management. With these issues in mind, the purpose of this study was to describe hypertension management in an academic family medicine clinic.
METHODS
Site and study subjects
This was a cross-sectional chart review of patients attending a multiphysician family medicine clinic. The clinic is a teaching site for family medicine residents and students in the allied health professions at the University of Alberta. The University of Alberta Research Ethics Board approved the study. Subjects were eligible for inclusion if they had 1 or more visits coded for hypertension (International Classification of Diseases, Ninth Revision, code 401) within the past 3 years. Subjects were excluded if they only had 1 recorded visit to the clinic, were younger than 18 years of age, were cognitively impaired, resided in an institution, were a student or employee of our health region or the University of Alberta, or did not communicate in English. The list of eligible subjects was then stratified based on the treating physician, and 35 subjects were randomly selected from each group to ensure a balanced representation from each physician (Figure 1).
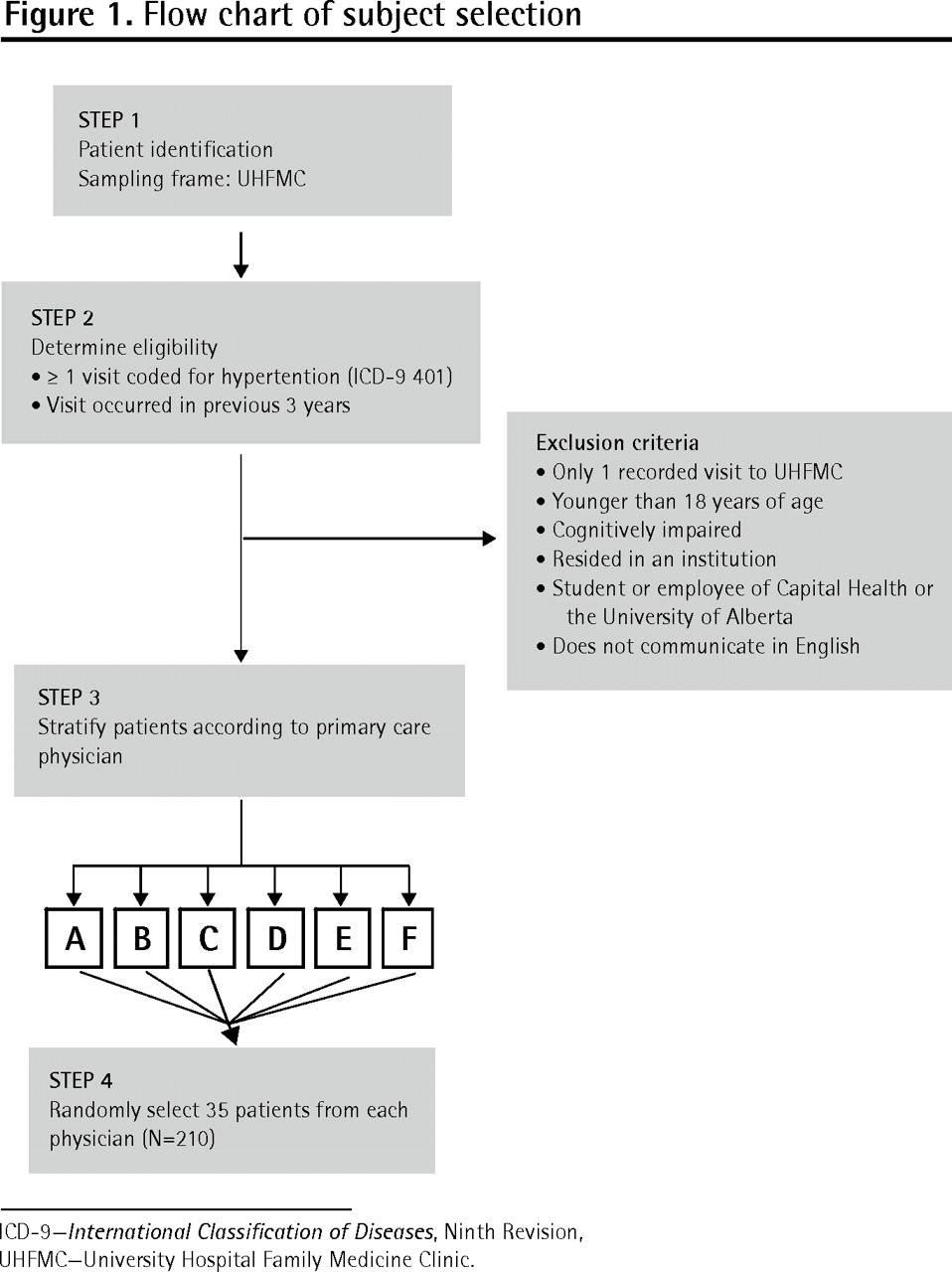
Flow chart of subject selection
Data collection
A standardized case report form was used to abstract information from subjects’ clinic records regarding date of birth, sex, most recent blood pressure measurements, antihypertensive medication therapies, compelling medical conditions as indicated in the 2006 CHEP recommendations, as well as smoking status and alcohol use.12
The most recent blood pressure measurement was defined as the last clinic visit with a recorded blood pressure. Medication lists recorded in the chart were reviewed to identify antihypertensive medications and medications known to induce hypertension according to the 2006 CHEP recommendations.12 Each medication was recorded by its generic name and total daily dose in milligrams. Antihypertensive medications were categorized as previous, current, or new to characterize their potential effect on the most recent blood pressure measurement. Previous antihypertensive medications had been discontinued 3 months before the date of the most recent blood pressure measurement. In these cases, the date of discontinuation was also recorded. Current antihypertensive medications were considered ongoing therapy or medications that had been discontinued within 3 months of the most recent blood pressure measurement. New anti-hypertensive medications indicated a change in dose or addition of a new antihypertensive medication on or after the date of the most recent blood pressure measurement.
According to the 2006 CHEP recommendations, the approach to hypertension management might be influenced by specific compelling indications, including diabetes, chronic renal disease (CRD), ischemic heart disease, myocardial infarction, angina, dyslipidemia, heart failure, cerebrovascular accident, and left ventricular dysfunction.12 For this study, such compelling indications were considered present if they were documented in the charts. Diabetes and angina were also considered present if antidiabetic medications or nitro-glycerin products, respectively, were listed in subjects’ medication lists.13
Sample size and analyses
During the design stage of this study, the most recent information from NHANES was based on the 2001 to 2002 cycle, in which 1038 of the 1696 participants (61%) with hypertension were treated with antihypertensive medications.14 Using this published treatment rate as our external benchmark and assuming an α error of .05 and β error of .20, we determined that 187 subjects would be required to detect a 10% absolute difference in treatment rate. The sample size was increased to 210 subjects by selecting 35 hypertensive subjects from each of the 6 physicians in our clinic.
Patients were considered to be receiving treatment for hypertension if their medication history included at least 1 new or current antihypertensive medication. Controlled hypertension was defined as a blood pressure below 140/90 mm Hg or, if the subject had diabetes or CRD, below 130/80 mm Hg.12
All analyses of the extracted data were descriptive, using frequencies and means where appropriate. Differences in the characteristics of subjects with controlled versus uncontrolled hypertension were tested using χ2 tests or 2-tailed t tests where appropriate. A P value less than .05 was considered statistically significant.
RESULTS
Mean age of the 210 subjects was 61.6 (SD 15.1) years, and 116 (55%) were women (Table 1). A total of 185 subjects (88%) were treated with antihypertensive medications, and 89 subjects (42%) had controlled hypertension. Younger people and those with diabetes appeared less likely to have controlled hypertension (Table 1).
Subject characteristics
A single antihypertensive medication was prescribed to 76 (36%) subjects, 2 anti-hypertensive medications were prescribed to 65 (31%) subjects, and antihypertensive regimens with 3 or more medications were prescribed to 44 (21%) subjects (Figure 2). Of the 185 subjects prescribed 1 or more antihypertensive medications, 84 (45%) had controlled blood pressure, compared with 5 of the 25 (20%) subjects not prescribed any antihypertensive medications (odds ratio 3.3, 95% confidence interval [CI] 1.3 to 8.8, P < .02) (Figure 3). The specific anti-hypertensive medications prescribed were angiotensin-converting enzyme (ACE) inhibitors in 51% of subjects, diuretics in 47%, β-blockers in 27%, calcium channel blockers in 23%, angiotensin receptor blockers (ARBs) in 20%, and an α-blocker in 1% (Table 2). As monotherapy, ACE inhibitors were the most frequently prescribed (46%), followed by diuretics (25%), ARBs (12%), β-blockers (12%), and calcium channel blockers (5%).

Antihypertensive medication regimens in 210 hypertensive subjects

Hypertension control according to antihypertensive medication use: Odds ratio 3.33, 95% confidence interval 1.25 to 8.83.
Antihypertensive medications prescribed in 210 subjects
Medication use in this study group was also compared with the 2006 CHEP recommendations for management of patients with compelling indications (Table 3 and Box 112). Of the 36 patients with either diabetes or CRD, 23 (64%) were prescribed ACE inhibitors or ARBs with or without thiazide diuretics. Of the 12 patients with documented cerebrovascular disease, 6 (50%) were prescribed β-blockers and 7 (58%) were prescribed ACE inhibitors.
Antihypertensive medication use according to compelling indication
Box 1 Treatment recommendations from the Canadian Hypertension Education Program guidelines12
Diabetes or chronic renal disease: ACE inhibitor or ARB with or without thiazide diuretic
Ischemic heart disease: ACE inhibitor (or ARB) and β-blocker (or long-acting CCB)
Cerebrovascular disease: ACE inhibitor and diuretic combination
ACE–angiotensin-converting enzyme, ARB–angiotensin receptor blocker, CCB–calcium channel blocker.
DISCUSSION
Since the last reported Canadian prevalence rate of 22% in 1992, the number of people with hypertension has steadily increased, with the most current estimate being 30% in the United States.7,8 Prevalence of this important cardiovascular risk factor is expected to continue to increase, especially as our population ages.15 Therefore, it is paramount that clinicians optimize management. Although the last Canadian community study reported low treatment and control rates, observations from the various NHANES cycles illustrate that these rates are slowly improving.7,8,14 Our cross-sectional chart review in an academic family medicine clinic determined that 88% of hypertensive subjects were prescribed antihypertensive medications and 42% had controlled hypertension. We also observed that subjects were 3 times more likely to have controlled hypertension if they were on at least 1 antihypertensive medication.
Although the difference in treatment and control rates between our clinic and the NHANES observations were initially anticipated, we did not test the statistical significance of this hypothesis for 2 reasons. First, the time gap between collection of the NHANES data, collected during the 2001 to 2002 and 2003 to 2004 cycles,7,14 and our study data, recorded primarily in 2005 and 2006, is relevant, given the increasing awareness and treatment of hypertension in recent years.7,10 Furthermore, the number of antihypertensive agents introduced onto the market during this period could also affect physician prescribing patterns. Second, the study groups used for the NHANES cycles differ greatly from our clinic population. The NHANES data are derived from a nationally representative sample of 5000 people randomly selected from the general population.6,7,14 The proportion of NHANES participants with regular family physicians is not known; in our study, all subjects had 1 or more visits to family physicians. There could, therefore, be a difference in accessibility of antihypertensive medications. Despite these differences, NHANES still provides the most current data characterizing hypertension treatment and control in North America and, therefore, serves as a reasonable benchmark for comparison.11
This study provided an opportunity to compare practice patterns with other important benchmarks. First, we identified that choice of antihypertensive medication was consistent with CHEP management recommendations for various compelling indications.12 For example, ACE inhibitors and ARBs were commonly used in patients with diabetes or CRD. Similarly, recommended first-line agents were used in most patients with cerebrovascular disease. Second, we observed that 66% of patients prescribed ACE inhibitors were using ramipril at doses consistent with clinical trials,16 suggesting good use of evidence-based medicine to guide therapy.
Our study suggested that younger age, diabetes, and no documented antihypertensive medications appeared to be associated with poor blood pressure control. Although it is well established that the hypertension control rate among those with diabetes is quite low,17 it was unexpected that older age, a cardiovascular risk factor in itself, would be associated with a higher proportion of controlled hypertension. Given the limitations of a cross-sectional study, however, this information should be interpreted with caution.11
Limitations
A number of factors might have limited our findings. These include the sensitivity of our inclusion criteria, variance in blood pressure measurements, white-coat hypertension, and our definition of treatment. First, we included subjects if they had any visits coded for hypertension within the previous 3 years because we believed subjects visiting their family physicians for hypertension management would likely have these visits coded as such. Although we expected this criterion to have high specificity, hypertensive patients visiting their family physicians for other indications, or patients with multiple comorbidities in addition to hypertension, might have been missed—contributing to a low sensitivity. Second, as this was a cross-sectional chart review, we were unable to standardize the method used for measuring blood pressure. As such, there would be variance in the blood pressure measurements among clinicians. Because these values were taken from the subjects’ medical records, however, they would reflect the actual values clinicians used for treatment decisions. Third, we used blood pressure measurements recorded in the clinic to determine if the subject had controlled hypertension. These measurements could be confounded by 2 well-known phenomena in hypertension management—white-coat hypertension and masked hypertension.4 A final limitation is that we restricted our definition of treatment to patients prescribed antihypertensive medications. This does not include lifestyle modifications, such as salt restriction and exercise advice.
Conclusion
This study used external benchmarks to examine hypertension management within our academic family medicine clinic. The hypertension treatment and control rates were qualitatively better than the most current NHANES measurements. Although prescribed antihypertensive therapy was consistent with current evidence and guideline recommendations, the overall treatment rate was not ideal. The next step in our quality improvement process will be to determine optimal treatment and control rates for hypertension and then identify barriers and facilitators to achieving these rates.18–20 For example, it might be of benefit to develop an interdisciplinary program to improve antihypertensive drug use. The ultimate goal of this process will be to close the gap between evidence-based guidelines and current patient care.
Notes
EDITOR’S KEY POINTS
-
Hypertension is the most common reason for visiting a physician, accounting for more than 20 million visits a year, but its asymptomatic nature sometimes makes it difficult to identify and treat–and makes medication adherence challenging. As a result, hypertension is generally not well controlled.
-
As part of a continuous improvement approach to management of patients with hypertension, the authors sought to compare rates of treatment and control of hypertension in their academic family medicine clinic with existing population data and found that their rates appeared to be higher than those among the general population. They also found that choice of antihypertensive medication was consistent with the Canadian Hypertension Education Program recommendations and that pre-scribed doses were consistent with clinical trials, suggesting good use of evidence-based medicine to guide therapy.
-
Although prescribed antihypertensive therapy was consistent with current evidence and guideline recommendations, the overall treatment rate was not ideal. The next step in the quality improvement process will be to determine optimal treatment and control rates for hypertension and then identify barriers and facilitators to achieving these rates.
POINTS DE REPÈRE DU RÉDACTEUR
-
L’hypertension est la raison la plus fréquente de consulter un médecin représentant plus de 20 millions de visites par année, mais sa nature asymptomatique la rend parfois difficile à identifier et à traiter, en plus de poser un défi pour l’observation de la médication. En conséquence, l’hypertension est souvent mal contrôlée.
-
Dans le cadre d’un projet visant à améliorer le traitement des hypertendus, les auteurs ont voulu comparer les taux de traitement et de contrôle de l’hypertension dans leur clinique de médecine familiale universitaire aux données de la population générale; ils ont trouvé que leurs taux semblaient plus élevés que ceux de la population générale. Ils ont aussi observé que le choix de la médication antihypertensive était conforme aux directives du Programme canadien d’éducation sur l’hypertension, et que les doses prescrites étaient conformes aux essais cliniques, ce qui suggère un usage adéquat de la médecine fondée sur des preuves pour guider le traitement.
-
Même si la médication antihypertensive prescrite était conforme aux données actuelles et aux recommandations, le taux de traitement n’était pas idéal. L’étape suivante dans le processus d’amélioration des soins sera de déterminer les taux optimaux de traitement et de contrôle de l’hypertension, pour ensuite identifier les facteurs qui empêchent ou facilitent l’atteinte de ces taux.
Footnotes
-
This article has been peer reviewed.
-
Contributors
Ms Houlihan and Drs Simpson, Cave, Flook, Hurlburt, Lord, Smith, and Sternberg contributed to concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Documentation and treatment of hypertension: quality of care and missed opportunities in a family medicine resident clinic
- Hypertension and the family physician
- Hypertension management by family physicians: Is it time to pat ourselves on the back?
- L'hypertension et le medecin de famille
- Prise en charge de l'hypertension par les medecins de famille: Est-ce le temps de nous feliciter?