


Heart failure (HF) is a common condition in primary care with 1% of the population self-reporting this condition. Mortality is substantial, approaching 40% to 50% over 5 years. Heart failure is a complex syndrome in which abnormal heart function results in, or increases the subsequent risk of, clinical symptoms and signs of low cardiac output or pulmonary or systemic congestion.1 This article will present some practical tips for managing HF.2
Case description
C.C. is a 67-year-old woman with a long history of dilated cardiomyopathy and chronic atrial fibrillation (since 1992), type 2 diabetes requiring insulin (since 1994), stage 3 chronic renal insufficiency (since 2005), and gastroesophageal reflux disease. She has an extensive list of medications: 160 mg of valsartan once daily; 10 mg of ramipril once daily; 40 mg of furosemide twice daily; 0.25 mg of digoxin once daily; 20 mg of atorvastatin once daily; 30 mg of nifedipine extended release once daily; 81 mg of acetylsalicylic acid once daily; 7.5 mg of warfarin once daily; 24 units of Novolin ge NPH in the morning, 30 units at supper; 10 units of Novolin ge Toronto in the morning, 5 units at night; 1000 mg of metformin twice daily; 150 mg of ranitidine once daily; 420 mg of magnesium oxide once daily; 500 mg of calcium carbonate once daily; and 300 mg of ferrous sulfate once daily.
After 16 years of stability, her lifestyle has deteriorated, with a poor diet and cessation of her cardiac rehabilitation exercise program. During 5 hospital admissions, 5 different cardiologists suggested differing treatment regimens, modifying doses or agents in the same class. Metabolic investigations reveal poor control of her diabetes, with a glycated hemoglobin A1c of 8.1%. Results of complete blood count and electrolyte measurement are normal, but her creatinine level is 160 mmol/L (estimated creatinine clearance 40 mL/min). Cardiac investigations reveal new triple-vessel coronary artery disease. She declines revascularization and wishes to be treated medically. Her atrial fibrillation is well controlled. Echocardiography shows systolic dysfunction with an ejection fraction between 18% and 28%. The cardiothoracic surgeon indicates that cardiac pacing or an implanted cardioverter defibrillator are not options for C.C. Her treatment is challenged by the family medicine resident who questions potential inconsistencies between her treatment regimen and HF management guidelines. The patient’s understanding of her condition is inadequate for her to comply effectively with lifestyle changes, and communication among her caregivers has been inadequate, given the complexity of her case.
Bringing evidence to practice
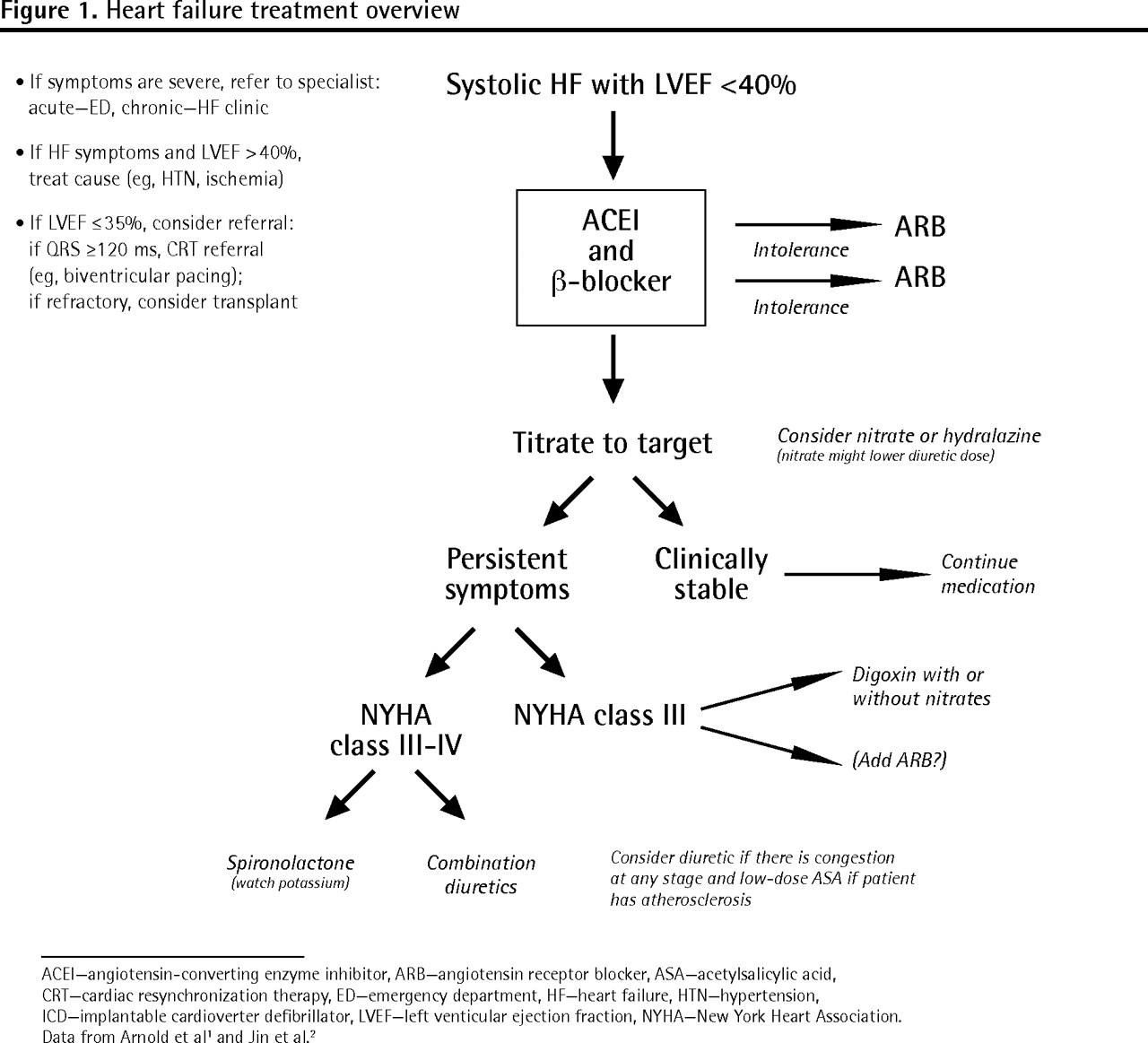
The management algorithm for chronic HF is summarized in Figure 1.2 Both aggressive use of medication to target doses and patient education are required for effective management of HF1; however, the foundation for all HF therapy includes nonpharmacologic management (Box 1).2
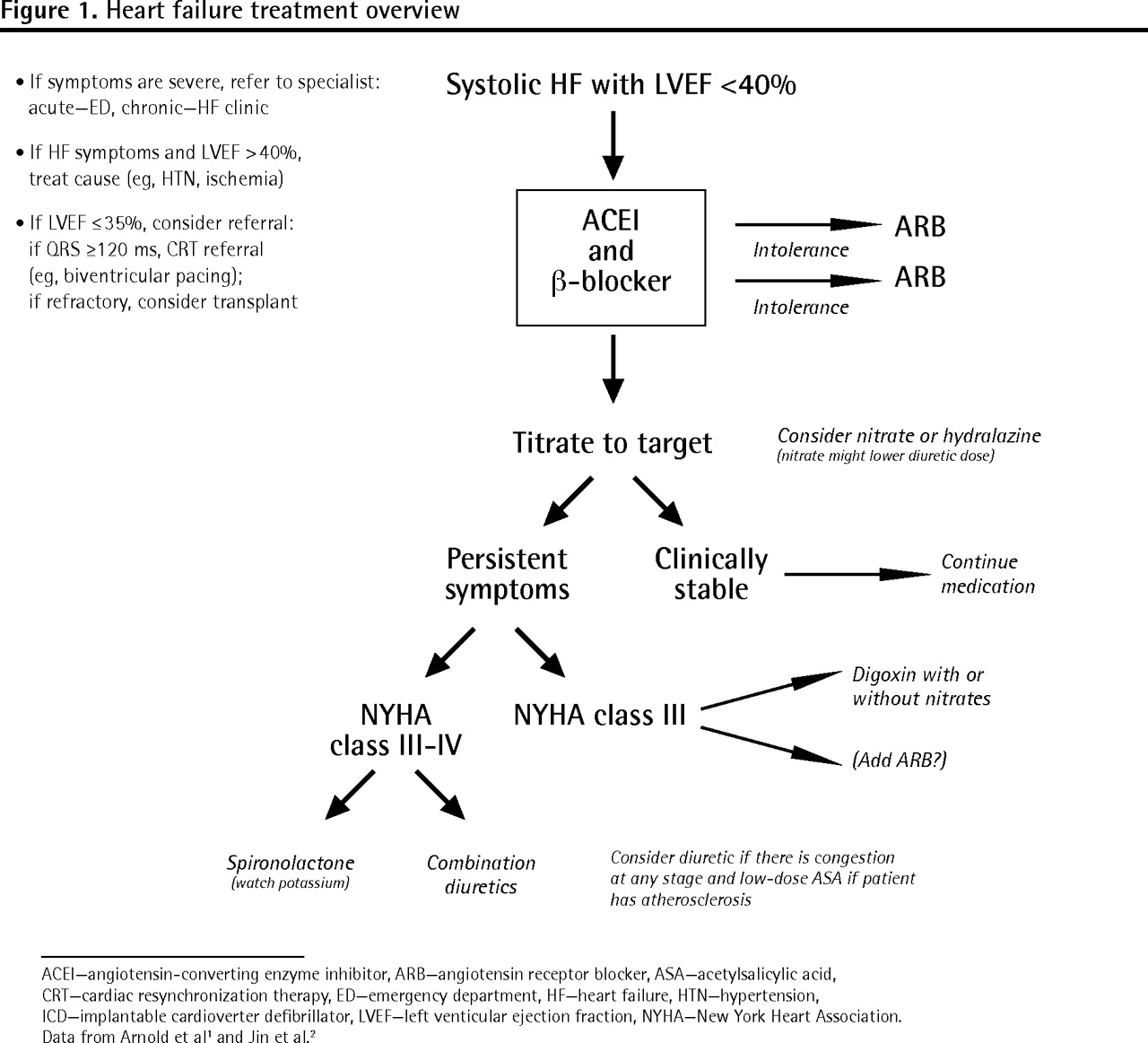
Heart failure treatment overview
ACEI—angiotensin-converting enzyme inhibitor, ARB—angiotensin receptor blocker, ASA—acetylsalicylic acid, CRT—cardiac resynchronization therapy, ED—emergency department, HF—heart failure, HTN—hypertension, ICD—implantable cardioverter defibrillator, LVEF—left venticular ejection fraction, NYHA—New York Heart Association.
Nonpharmacologic management of heart failure
|
Data from Jin et al.2
Dietary, lifestyle, and over-the-counter nonsteroidal anti-inflammatory drug indiscretions are common sources of HF exacerbations.2,3 Lifestyle measures facilitate HF management. Communicating information about exercise and salt and fluid intake to patients is essential for optimal management.
-
The patient can exercise aerobically 3 to 5 times per week (30 to 40 minutes per session) for New York Heart Association class I to III HF.4
-
All patients need to restrict salt intake to 2 to 3 g (0.5 tsp) per day. Patients with unremitting fluid retention or advanced cardiac failure (ejection fraction less than 35%) require restriction to less than 2 g (eg, approximately 0.25 tsp) of salt per day.
-
Have patients report any weight gain of 2 lb (1 kg) in 1 to 2 days or 5 lb (2 kg) in 1 week. Selected patients might be suitable candidates to self-adjust their furosemide doses, doubling furosemide until normal weight is restored or holding furosemide if weight decreases by 1 kg.
-
Patients, especially those with renal dysfunction or hyponatremia, should restrict fluid intake to 1.5 to 2.0 L per day.
Diuretics are useful in providing symptom relief, especially acutely, but do not prevent long-term mortality.3 Overreliance on diuretics often results in hypotension and electrolyte abnormalities, limiting the use of other agents that reduce mortality.
-
Loop diuretics are preferred for congestive symptoms. Once symptoms are relieved, use the lowest effective maintenance dose. Multiple daily dosing can be used to improve diuretic effect, especially if higher doses are needed.
-
If persistent volume overload continues with optimal furosemide therapy, add a low-dose thiazide diuretic or metolazone (most effective if given 30 minutes before furosemide).5 Remember to monitor daily weight and regularly measure creatinine, urea, potassium, and magnesium levels.
-
Spironolactone (12.5 to 25 mg) should be considered for patients with an ejection fraction of less than 30% and symptoms of HF.6 Although the target dose in the RALES (Randomized Aldactone Evaluation Study Investigators) trial was 50 mg, 25 mg daily was the average dose reached.6 Remember to watch out for hyperkalemia.
-
Isosorbide dinitrate or a nitroglycerin patch are additional options, especially for nocturnal dyspnea.
While diuretics help symptoms, β-blockers (BBs) and angiotensin-converting enzyme inhibitors (ACEIs) have the best demonstrated evidence for mortality and morbidity outcomes in HF.7–9
-
The maximum tolerated target dose of ACEI should be used in all HF patients with ejection fractions of less than 40%1 (Table 1).2,3,10–16,* If ACEI intolerance develops, an angiotensin receptor blocker (ARB) can be used.13,17
-
Generally, ACEIs and ARBs should not be combined, as adverse effects increase with little extra benefit. Exceptions might include symptomatic patients with class III or IV HF on optimum ACEI and BB treatment, or those unable to tolerate BBs.2 Blood pressure, serum creatinine, and potassium should be monitored.
-
To titrate ACEIs or ARBs, start at low doses, then double the dose at 1- to 2-week intervals until the target dose is reached or until intolerable side effects persist. Trial evidence for best HF outcomes has been with relatively high doses.14,18
-
β-Blockers have strong evidence for mortality reduction.7 Initiate only if patients’ HF is stable and euvolemic. Start at low doses and double the dose every 2 to 4 weeks. Warn patients to expect some symptom worsening, initially.
-
When pursuing maximum tolerated doses of ACEIs or BBs, a heart rate as low as 50 beats per minute or a blood pressure as low as 80/50 mm Hg might not require any change in therapy, as long as the patient is not showing symptoms of hypotension (eg, dizziness and falls).
Heart failure drugs overview comparison chart
Other agents can help if symptoms persist after maximizing the most beneficial agents.
-
Digoxin can be used to improve symptoms and decrease hospitalization if symptoms persist on optimal treatment, especially if the ejection fraction is less than 30% or for concomitant treatment of atrial fibrillation. The target blood level in HF is less than 1.3 nmol/L to prevent adverse events.19
-
Combination isosorbide dinitrate and hydralazine should be considered in addition to standard therapy for African Americans with systolic dysfunction20 and for HF patients unable to tolerate other standard treatment or who have chronic renal failure. A nitroglycerin patch can be substituted for oral nitrates. Remember to allow for a 12-hour nitrate-free period.
While patient dietary indiscretions often occur, we must also be aware of prescriber indiscretions that can exacerbate HF. Specifically, medications such as nonsteroidal anti-inflammatory drugs, antiarrhythmic agents, diltiazem, verapamil, stimulants, glitazones, corticosteroids, tumor necrosis factor blockers, and numerous cancer chemotherapeutic agents are implicated.1,3
Case resolution
Steps are taken to improve C.C.’s treatment regimen. The first step is communication with her HF clinic physician, who agrees to be the primary consultant for cardiac therapy changes. She participates in an intense educational program on HF. In the year after her therapy is changed, C.C. avoids any admission to the hospital for HF. Her medications are adjusted and better reflect the evidence-based treatment guidelines: 10 mg of ramipril once daily; 10 mg of bisoprolol once daily; 0.125 mg of digoxin once daily; 25 mg of spironolactone once daily; 80 mg of furosemide twice daily; 2.5 mg of metolazone on Monday, Wednesday, and Friday; 420 mg of magnesium oxide once daily; 60 mg of isosorbide mononitrate at bedtime; 600 mg of Slow K once daily; 5 mg of warfarin once daily; 40 mg of atorvastatin once daily; 81 mg of acetylsalicylic acid once daily; 40 units of Novolin ge NPH twice daily; 24 units of Novolin ge Toronto 3 times daily; 20 mg of rabeprazole once daily; 1000 IU of vitamin D once daily; 300 mg of ferrous sulfate once daily; and 500 mg of calcium carbonate once daily. Metformin, which had been held during periods of acute congestion, was restarted at 500 mg twice daily, in line with current recommendations.3
Important concepts in management of chronic HF are summarized in Box 2.2 Educating patients on lifestyle measures supports medication management. Ensuring patients approach the maximal tolerated target doses for ACEIs and BBs improves mortality and morbidity. Adhering to the targets of treatment, combined with patient education and communication between family physicians, cardiologists, pharmacists, and dietitians, will lessen the burden of this disease on patients, caregivers, and the health care system.
Pearls for decreased morbidity and mortality in HF
|
ACEI—angiotensin-converting enzyme inhibitor, ARB—angiotensin receptor blocker BB—β-blocker, HF—heart failure.
Data from Jin et al.2
Notes
RxFiles is an academic detailing program providing objective comparative drug information. RxFiles incorporates information from family physicians, other specialists, and pharmacists with an extensive review of the literature to produce newsletters, question-and-answer summaries, trial summaries, and drug comparison charts. The RxFiles Drug Comparison Charts book and website have become practical tools for evidence-based and clinically relevant drug use information throughout Canada. For more information, go to www.RxFiles.ca.
Footnotes
-
↵* The full version of the RxFiles heart failure overview and treatment chart is available at www.cfp.ca. Go to the full text of the article online, then click on CFPlus in the menu at the top right-hand side of the page.
-
Competing interests
RxFiles and contributing authors do not have any commercial competing interests. RxFiles Academic Detailing Program is funded through a grant from Saskatchewan Health to Saskatoon Health Region; additional “not for profit; not for loss” revenue is obtained from sales of books and online subscriptions.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.