


ABSTRACT
OBJECTIVE To explore physicians’ knowledge of and attitudes toward hyperbaric oxygen therapy (HBOT) in order to better understand current diabetic foot ulcer management practices and to determine potential barriers to HBOT use.
DESIGN A 24-item questionnaire.
SETTING Primary Care Today conference in Toronto, Ont, in May of 2006.
PARTICIPANTS Physician attendees, 313 of whom completed the survey.
MAIN OUTCOME MEASURES Self-reported knowledge of and attitudes toward HBOT.
RESULTS Less than 10% of respondents had a good knowledge of HBOT, but 57% had a good attitude toward HBOT. Knowledge of and attitude toward HBOT were positively correlated (P < .0001). Good knowledge of HBOT was associated with sex (P = .0334), age younger than 40 years (P = .0803), years in medical practice (P = .0646), patient requests for HBOT referrals (P = .0127), and having previously referred patients for HBOT (P < .001). Twenty years or more in medical practice (P = .0593) and receiving patient requests for HBOT (P = .0394) were multivariate predictors of having good knowledge of HBOT. Good attitude toward HBOT was associated with age younger than 40 years (P = .0613) and having previously referred patients for HBOT (P = .0013). Multivariate analysis showed that male physicians (P = .0026) received more patient requests for HBOT (P < .0001), had good knowledge (P = .0129) and a good attitude (P = .0488), and were more likely to refer patients for HBOT.
CONCLUSION Primary care physicians have underdeveloped knowledge of HBOT, but their generally positive attitudes toward its use suggest that they might be receptive to educational interventions. Educating both physicians and patients about HBOT, specifically its cost-effectiveness, might encourage future use.
Development of lower limb ulcers is a serious complication of diabetes, affecting 15% of all patients with diabetes over the course of the disease1,2 and accounting for 20% of diabetes-related hospital admissions in North America.3–6 Management of lower limb ulcers, commonly known as diabetic foot ulcers (DFUs), has traditionally involved surgical referral, which might lead to resultant limb loss via amputation. The problem often escalates because of excessive postamputation pressure on the remaining limb. Contralateral amputation occurs an average of 2 years later.7 Subsequent post-amputation mortality rates can be as high as 50% after 3 years and rise to 70% after 5 years.8–13
A recent systematic review of hyperbaric oxygen therapy (HBOT) in the management of chronic wounds revealed that adjunctive HBOT reduces the risk of major amputations among patients with diabetes.14 In HBOT, systemically applied pharmacologic doses of oxygen (ie, breathing 100% oxygen at greater than 1.4 atm) are delivered via perfusion to all tissues. Poorly perfused tissue therefore receives some oxygen through diffusion, yet an oxygen concentration gradient between hypoxic and perfused tissue is established. The macrophages are sensitive to this gradient, producing angiogenic factors in response to the hypoxic signal. This is but one vasculogenic process augmented by the oxidative stress of HBOT; others include vascular endothelial growth factor production,15 mobilization of endothelial progenitor stem cells, and thioredoxin activation (which leads to elevations of hypoxia-inducible factors 1 and 2).16 This initiation of vascular repair can be seen clinically as improved wound healing.
A recent report by the Canadian Agency for Drugs and Technologies in Health (CADTH) concluded that HBOT for DFUs is cost-effective compared with standard methods of care.17,18 In spite of this, limb salvage by adjunct HBOT is rarely used by Canadian primary health care providers, who provide most of the health care for patients with diabetes.19 With the rising incidence of diabetes mellitus in North America20,21 it is becoming increasingly important for primary care physicians to update their knowledge of both this disease and the management of its comorbidities, including the benefits of such relatively new therapies as HBOT.
Guo et al22 recently identified factors that influenced American wound care specialists’ adoption of HBOT in the treatment of chronic wounds. In order to elucidate similar information in the Canadian physician population, we administered surveys about HBOT to primary care physicians at one of the largest annual medical conferences in the country. The purpose of this study is to explore the prevailing knowledge base and attitude trends regarding HBOT in a sample of primary care providers in order to identify potential barriers to its use, as well as to gauge physicians’ receptiveness to this therapy. Further, discovery of knowledge gaps and negative attitude predictors will help to identify physicians who would benefit most from future educational efforts. If physicians’ knowledge of and attitudes toward HBOT are improved, patients will be more likely to receive optimal care and avoid devastating lower limb amputation.
METHODS
Sample selection and exclusion criteria
The study was conducted at the medical conference Primary Care Today in May 2006. The 24-item questionnaire was distributed to 818 attendees, which included both physicians and nonphysicians. Questionnaires were excluded if respondents did not identify themselves as physicians.
The questionnaire was adapted from that of Guo et al,22 who assessed American wound care specialists’ knowledge of HBOT. The survey was pretested on 5 health care providers and further refined based on their feedback.
Survey instrument
Physician characteristics ascertained in the first section of the questionnaire included year of graduation, health care field, sex, age, practice postal code, and practice setting. The second section pertained to respondents’ sources of medical knowledge, referral patterns, and monthly volume of wound-care patients. The third section contained 3 items that addressed respondents’ self-reported knowledge of HBOT, which was measured using a 5-point Likert scale. For the purposes of statistical analyses, the answers to these 3 questions were compiled into 1 composite score as an overall measure of familiarity or knowledge, a decision supported by both reliability analysis (Cronbach α = 0.82 for internal consistency) and factor analysis (74% of the variance explained by 1 factor). The composite score was further dichotomized as “more than somewhat knowledgeable” if the value was greater than 3.5 or as “otherwise” if less than 3.5. “Good physician knowledge” was therefore defined as a composite familiarity score in excess of 3.5.
Respondents’ attitudes toward HBOT as an adjunct treatment of chronic DFUs were assessed in the same manner. Scores from 5 questions about attitude toward HBOT were compiled into 1 composite score as an overall measure of attitude toward HBOT, a decision supported by reliability analysis (Cronbach α = 0.91 for internal consistency) and factor analysis (75% of the variance explained by 1 factor). The composite score was dichotomized as “agree or more” if it exceeded 3.5. Hence, “good physician attitude” was also defined as a composite score in excess of 3.5.
Heat maps
Ontario has been regionally divided into Local Health Integration Networks (LHINs) to geographically consolidate fiscal management of health care.23 Heat maps showing the relative proportion of physicians with good knowledge of or attitudes toward HBOT in each LHIN were made using ArcGIS version 9.
Analysis
Statistical Analysis Software version 9.1 for Windows was used for statistical analysis. Descriptive data were presented as frequencies and percentages; χ2 analysis, Fisher exact tests, and multiple logistic regression models were used to identify predictors of good physician knowledge of and attitudes toward HBOT. Statistical significance was set at P < .05.
RESULTS
Of the 818 conference attendees who received questionnaires, 451 (55.1%) responded; of those, 126 surveys (15.4%) were excluded because they were completed by nonphysicians. An additional 12 surveys (1.5%) were excluded because the responding physicians did not complete the portion of the survey on HBOT. In total, 313 questionnaires (38.3%) were retained for analysis.
The respondents’ median age was 46 years, and about half of respondents were female. More than 80% of respondents indicated that they were family physicians. Most (90.3%) practised in urban communities, and 77.0% saw 5 or fewer wound care patients per month (Table 1). When asked to report their practice locations, 79.2% (248) of the respondents provided Ontario postal codes, 13.4% (42) provided postal codes from outside of Ontario, and 7.4% (23) did not provide postal codes.
Respondents’ subjective knowledge of and attitudes toward HBOT in wound care: N=313, but not all categories add to 313 owing to missing data.
For the 3 subjective knowledge questions, the physicians were asked to assess their familiarity with HBOT. Most respondents (mean score 60.7%, range 52.7% to 69.3%) indicated that they had little or no knowledge of HBOT (Table 2).
Respondents’ subjective knowledge of HBOT: N=313.
For 5 of the 6 questions about physicians’ attitudes toward HBOT, most respondents (mean 58.9%, range 56.2% to 65.8%) exhibited a positive attitude by agreeing or strongly agreeing with the provided statements. The remaining attitude question pertained to the cost-effectiveness of HBOT. Only 32.9% of respondents agreed or strongly agreed that HBOT was cost-effective, while most (62.9%) neither agreed nor disagreed (Table 3).
Respondents’ attitudes toward use of HBOT in wound care: N=313.
Demographic factors that correlated with good knowledge of HBOT (Table 1) included male sex (P = .0334), having received patient requests for HBOT referrals (P = .0127), and having previously referred patients for HBOT (P < .001). Positive attitude toward HBOT was significantly associated with having referred patients for HBOT (P = .0013).
Respondents indicated that they update their medical knowledge using the following sources: medical journals and websites (97.8%), lectures and grand rounds (62.6%), nonmedical websites (46.6%), colleagues (27.2%), news media (25.6%), patients (12.1%), formal diver training courses (10.2%), and formal hyperbaric courses (2.2%). The last 2 sources were specifically included in the survey to investigate whether seeking information on HBOT was a priority for respondents when building upon their medical knowledge. Formal hyperbaric courses (P = .0195), formal diving courses (P = .0094), and news media (P = .0125) were significantly related to good knowledge of HBOT. The only sources of medical knowledge significantly associated with good attitude toward HBOT were lectures and grand rounds (P = .046).
Overall, less than a tenth of the physicians surveyed exhibited good knowledge of HBOT, although 57.2% had a positive attitude toward it. Knowledge and attitude were significantly correlated (P = .0115). Nearly half (49.8%) of respondents exhibited poor knowledge but good attitude (Table 4).
Correlation between respondents’ subjective knowledge of and their attitudes toward the use of HBOT in wound care: N=313; P = .0115.
Multivariate analysis of respondents’ knowledge of HBOT revealed that physicians who had practised for at least 20 years were more than twice as likely to have good knowledge of HBOT. Physicians whose patients had requested referrals for HBOT were nearly 3 times more likely to be knowledgeable about HBOT (Table 5). Further, a patient request was strongly associated with subsequent HBOT adoption in primary care practice (Table 6).
Multivariate analysis of respondents’ subjective knowledge of HBOT
Variables associated with adoption of HBOT in primary care practice
DISCUSSION
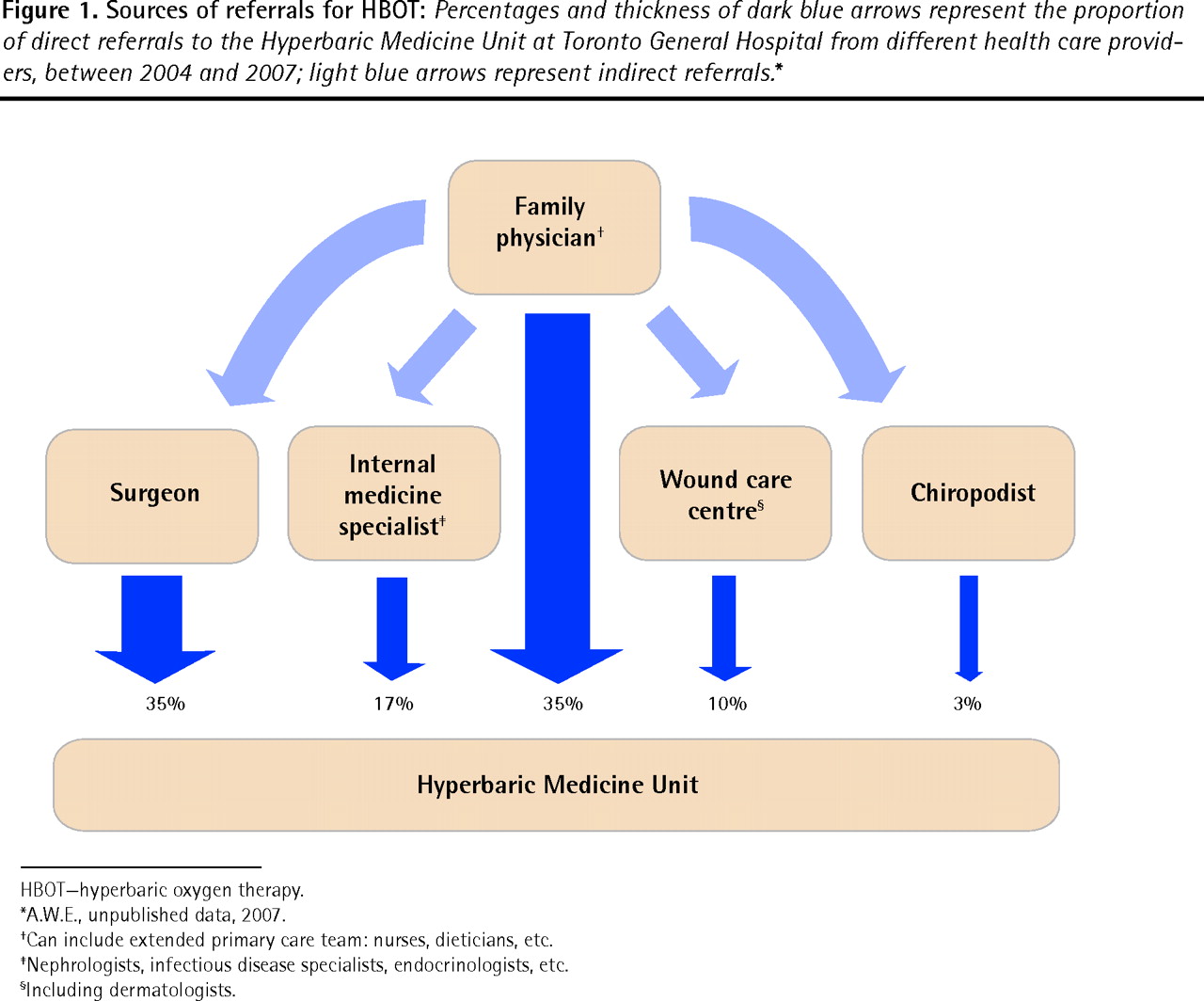
Primary care physicians are the principal managers of the health care of patients with diabetes and, along with surgeons, are responsible for more than 70% of referrals for HBOT (Figure 1). Yet only 10% of the surveyed physicians exhibited good knowledge of HBOT—a limb-salvaging therapy for some patients. Despite their poor knowledge of HBOT, however, nearly half of such respondents still demonstrated a positive attitude toward the therapy, suggesting that these physicians might be receptive to educational interventions. Improved knowledge of HBOT could encourage physicians to consider HBOT as a treatment option for their patients and increase the likelihood of patient referral.
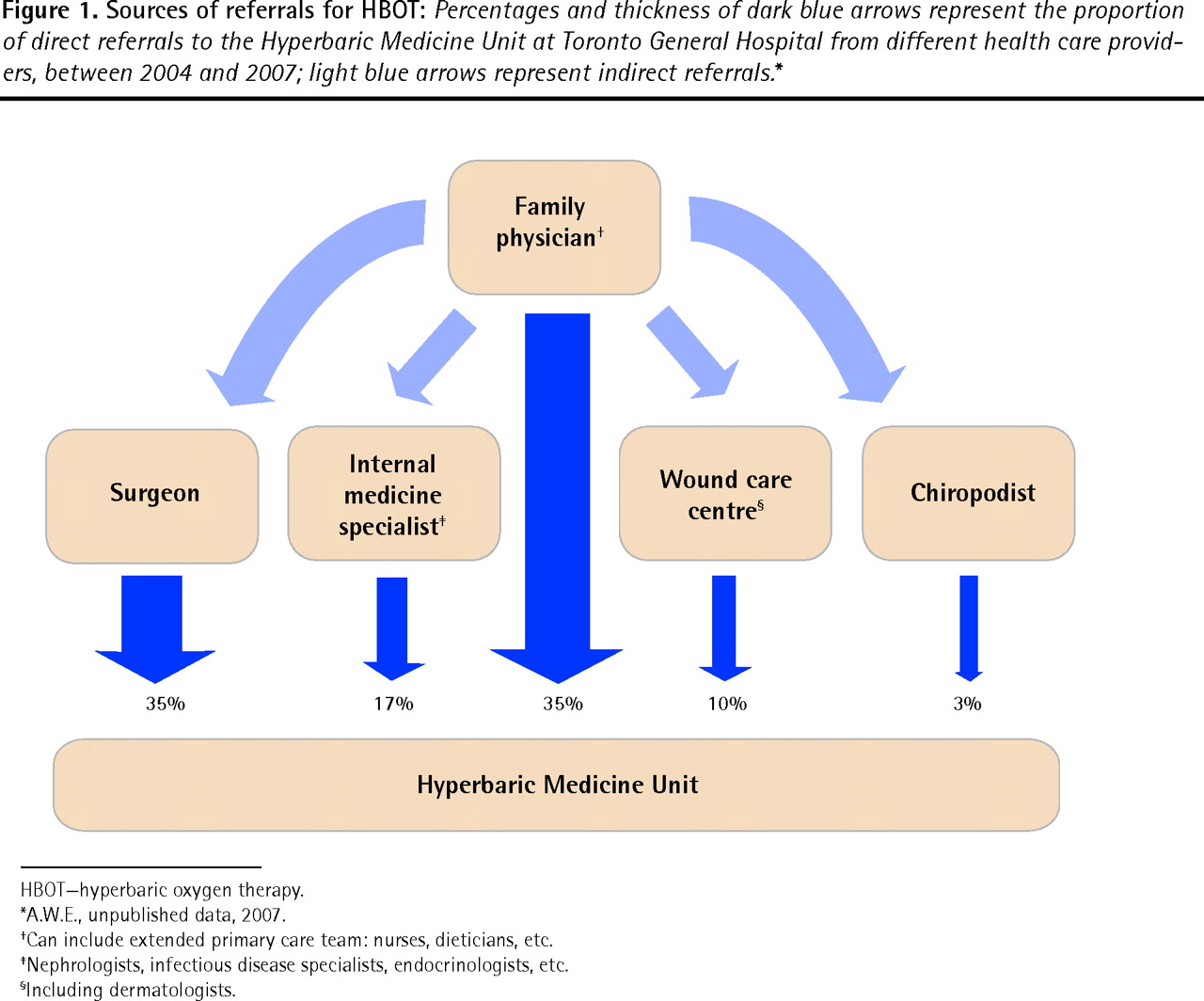
Sources of referrals for HBOT: Percentages and thickness of dark blue arrows represent the proportion of direct referrals to the Hyperbaric Medicine Unit at Toronto General Hospital from different health care providers, between 2004 and 2007; light blue arrows represent indirect referrals.*
HBOT—hyperbaric oxygen therapy.
*A.W.E., unpublished data, 2007.
†Can include extended primary care team: nurses, dieticians, etc.
‡Nephrologists, infectious disease specialists, endocrinologists, etc.
§Including dermatologists.
Owing to the scarcity of hyperbaric oxygen chambers in Canada and the lack of formal HBOT training at Canadian medical schools, physicians must actively seek information when interested in this treatment. Consistent with this notion, participation in either HBOT courses or diving courses was correlated with good knowledge of HBOT. More specific continuing medical education events that make HBOT information more easily accessible could help remedy this knowledge deficit.
Physicians who have been in practice for 20 years or more possessed better knowledge of HBOT, likely because there was more opportunity for exposure to HBOT over the course of a relatively longer career. Additionally, physicians who received patient requests for referral for HBOT displayed a higher level of knowledge because they were likely motivated to learn more about the treatment. Educating patients about HBOT (eg, including information about HBOT in brochures for patients with diabetes) might help to introduce HBOT to physicians earlier in the course of their patients’ care, encouraging physicians to learn about and use this treatment.
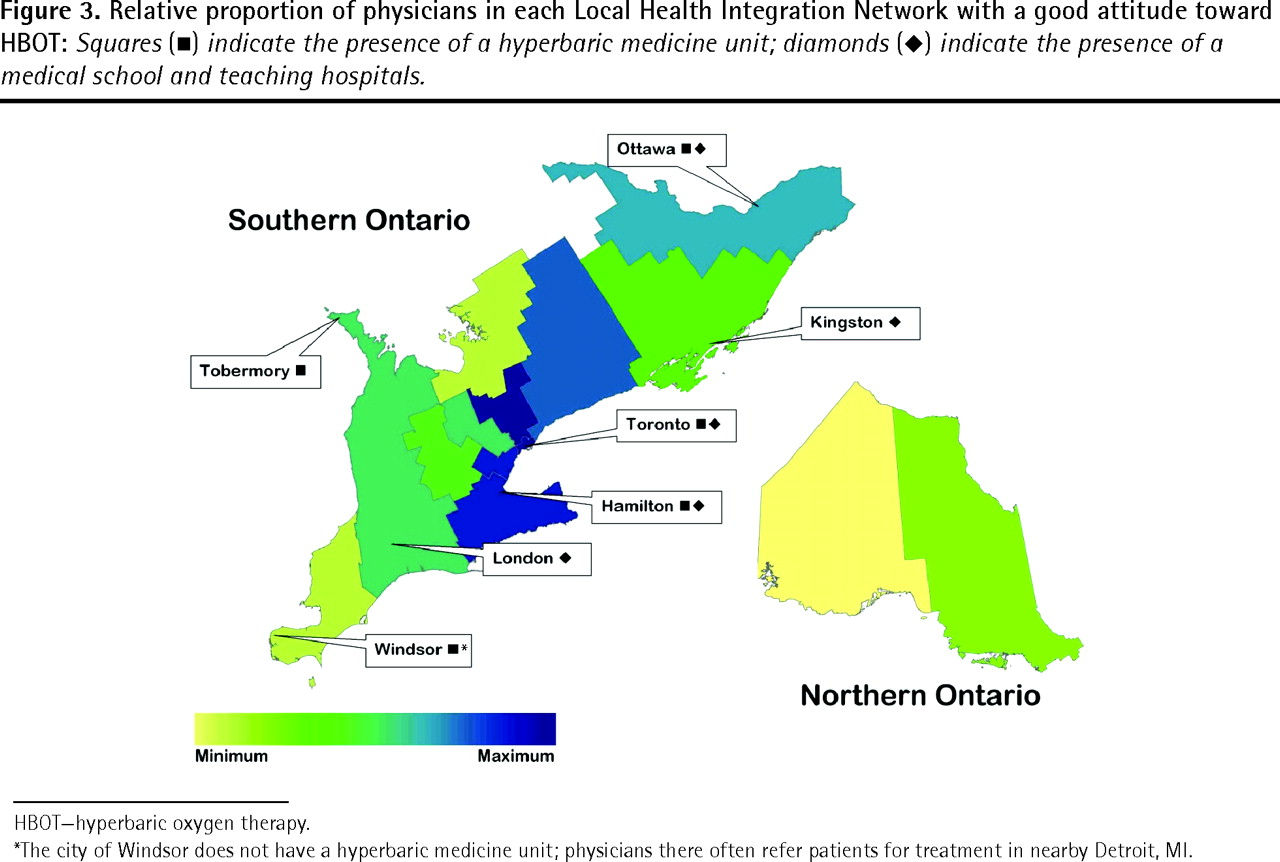
Interestingly, physicians who practised in LHINs that contain both HBOT chambers and medical schools were found to have better knowledge of and attitudes toward HBOT than those who practised in other LHINs (Figures 2 and 3). Exposing medical students to nearby HBOT chambers might foster better knowledge of and attitudes toward the therapy among future doctors. Encouraging such early exposure might also remedy the apparent discrepancy between the knowledge of younger physicians and that of physicians who have practised for 20 years or more. Accordingly, creation of a Canadian residency in hyperbaric medicine should also be a long-term objective.

Relative proportion of physicians in each Local Health Integration Network with a good knowledge of HBOT: Squares (▪) indicate the presence of a hyperbaric medicine unit; diamonds (♦) indicate the presence of a medical school and teaching hospitals.
HBOT—hyperbaric oxygen therapy.
*The city of Windsor does not have a hyperbaric medicine unit; physicians there often refer patients for treatment in nearby Detroit, MI.

Relative proportion of physicians in each Local Health Integration Network with a good attitude toward HBOT: Squares (▪) indicate the presence of a hyperbaric medicine unit; diamonds (♦) indicate the presence of a medical school and teaching hospitals.
HBOT—hyperbaric oxygen therapy.
*The city of Windsor does not have a hyperbaric medicine unit; physicians there often refer patients for treatment in nearby Detroit, MI.
Although the physicians surveyed generally showed enthusiasm about HBOT, they were somewhat undecided when asked about its cost-effectiveness. A recent health technology assessment report by CADTH concluded that HBOT for DFUs is indeed cost-effective compared with standard care.17,18 The misconception that HBOT is an expensive burden to the health care system might be partially responsible for the reluctance to refer patients for this treatment and is a topic that should be addressed as part of educational interventions.
Although correcting the aforementioned knowledge gaps is a crucial step toward optimizing management of DFUs, the key obstacle that must ultimately be overcome is lack of access to HBOT. There are more than 500 HBOT facilities in the United States, while the authors estimate that there are perhaps 20 in Canada. As a result, HBOT wait times escalate, likely contributing substantially to its underuse. The CADTH report suggests that 179 monoplace chambers or 19 multiplace chambers need to be built across Canada in order to treat all prevalent DFU cases in Canada.17,18 Until a large number of HBOT treatment centres are constructed to effectively manage the rising number of DFU cases, the suggested educational interventions will not address the underlying problem of access. However, educating physicians and their patients is an important first step that will empower and motivate them to lobby policy makers so that implementation and provision of new HBOT units becomes a priority.
Limitations
The study population consisted of the Canadian primary care physicians who attended this particular conference and voluntarily completed the survey. As such, it was not necessarily representative of all Canadian physicians, particularly those outside of Ontario where the conference took place. In addition, when investigating patient referral it is important to note that not all physicians see patients for whom referral for HBOT would be appropriate. Nevertheless, we are confident that the overwhelming lack of knowledge with respect to HBOT in Canada is certainly a reality.
Conclusion
Canadian primary care physicians appear to have little or no knowledge of HBOT and its mechanisms of action, contraindications, or adverse effects. As primary care physicians manage the bulk of the health care for patients with diabetes, it is imperative that their knowledge of HBOT be improved so that DFUs are treated optimally.
Despite their lack of knowledge, however, Canadian physicians’ fairly positive attitude toward HBOT suggests that they would be receptive to further education on the subject. Interventions in medical schools and continuing medical education events might improve Canadian physicians’ knowledge of HBOT and correct misconceptions, particularly those related to cost. Patient education strategies should also be expanded so that knowledgeable patients can encourage their physicians to seek out information about HBOT.
At present, amputation is the standard of care in Canada for nonhealing DFUs. With improved treatment access and effective educational interventions, HBOT should make the limb-sparing and cost-saving contributions that the literature suggests are possible.
Acknowledgments
This study was supported by the Adrian and Reta Hudson Fund at the Toronto Community Foundation. We also thank the Primary Care Today conference directors, the volunteers who facilitated survey administration, and all subjects who agreed to be surveyed.
Notes
EDITOR’S KEY POINTS
-
Hyperbaric oxygen therapy (HBOT) is an adjunct treatment that reduces the risk of major amputations following the development of ischemic diabetic foot ulcers (DFUs). Contrary to conservative belief, recent economic analysis reports that HBOT is more cost-effective than standard care; however, HBOT is substantially underused in Canada.
-
Optimal treatment and appropriate referral for HBOT depends on primary care physicians’ knowledge of and attitudes toward this treatment. This study aimed to explore these factors.
-
Although few physicians had good knowledge of HBOT, their fairly positive attitudes toward its use suggested that they would be receptive to further education on the subject. However, such educational interventions would not address the underlying problem of access, as there is currently an inadequate number of HBOT chambers in Canada to effectively treat all patients with DFUs.
-
At present, amputation is the standard of care in Canada for nonhealing DFUs. With improved treatment access and effective educational interventions, HBOT should make the limb-sparing and cost-saving contributions that the literature suggests are possible.
POINTS DE REPÈRE DU RÉDACTEUR
-
L’oxygénothérapie hyperbare (OTHB) est un traitement d’appoint qui réduit le risque d’amputation majeure en cas d’ulcère ischémique du pied diabétique (UPD). À l’encontre des croyances conservatrices, une analyse récente montre que l’OTHB a un meilleur rapport coût-bénéfice que le traitement conservateur; toutefois, l’OTHB est grandement sous-utilisée au Canada.
-
Un traitement optimal et une demande appropriée pour utiliser l’OTHB dépendent des connaissances des médecins de première ligne sur l’OTHB et de leur attitude envers ce traitement. Cette étude voulait examiner ces derniers facteurs.
-
Même si peu de médecins connaissaient bien l’OTHB, leur attitude généralement positive envers son utilisation laisse croire qu’ils seraient disposés à en apprendre davantage sur ce sujet. De telles sessions de formation ne résoudraient toutefois pas le problème sous-jacent d’accès, puisqu’il n’y a pas suffisamment de chambres hyperbares au Canada pour traiter efficacement tous les patients souffrant d’UPD.
-
Actuellement au Canada, le traitement standard pour l’UPD réfractaire est l’amputation. Un meilleur accès à l’OTHB et des sessions de formation efficaces devraient permettre de conserver des membres et de réduire les coûts, comme le suggère la littérature.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Contributors
All authors contributed to concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.