


ABSTRACT
OBJECTIVE To determine the effects of adding stages of change–based counseling to an exercise prescription for older, sedentary adults in family practice.
DESIGN The Step Test Exercise Prescription Stages of change counseling study was a 12-month cluster randomized trial.
SETTING Forty family practices in 4 regions of Canada.
PARTICIPANTS Healthy, community-dwelling men (48%) and women (52%) with a mean (SD) age of 64.9 (7.1) years (range 55 to 85 years). There were a total of 193 participants in the intervention group and 167 in the control group.
INTERVENTION Intervention physicians were trained to deliver a tailored exercise prescription and a transtheoretical behaviour change counseling program. Control physicians were trained to deliver the exercise prescription alone.
MAIN OUTCOME MEASURES Predicted cardiorespiratory fitness, measured by predicted maximal oxygen consumption (pVO2max), and energy expenditure, measured by 7-day physical activity recall.
RESULTS Mean increase in pVO2max was significant for both the intervention (3.02 [95% confidence interval 2.40 to 3.65] mL/kg/min) and control (2.21 [95% confidence interval 1.27 to 3.15] mL/kg/min) groups at 12 months (P < .001); however, there was no difference between groups. Women in the intervention group improved their fitness significantly more than women in the control group did (3.20 vs 1.23 mL/kg/min). The intervention group had a 4–mm Hg reduction in systolic blood pressure, while the control group’s mean reduction was 0.4 mm Hg (P < .001). The mean (SD) energy expended significantly increased and was higher in the intervention group than in the control group (69.06 [169.87] kcal/d vs −6.96 [157.06] kcal/d, P < .006). Practice setting characteristics did not significantly affect the primary outcomes.
CONCLUSION The Step Test Exercise Prescription Stages of change exercise and behavioural intervention improved fitness and activity and lowered systolic blood pressure across a range of Canadian practices, but this was not significantly different from the control group, which received only the exercise prescription. Women in the intervention group showed higher levels of fitness than women in the control group did; men in both groups showed similar improvement.
Accumulating evidence indicates that short- and long-term1,2 exercise prescription programs improve aerobic fitness. Sedentary lifestyle is associated with an increased risk of coronary artery disease, diabetes, hypertension, and osteoporosis3–5; however, many older adults remain inactive.
Estimates indicated that only 21% of Canadians—and only 17% of Canadians aged 55 years and older—were physically active in 2000 to 2001.6 Similarly, the 2000 National Health Interview Survey indicated that only 19% of Americans and 15% of Americans aged 65 years and older achieved the level of physical activity recommended in the Healthy People 2010 guidelines.7 By 2025, the number of Canadians older than 65 years is expected to double,8 and the absolute number of inactive older Canadians with related comorbidity could reach epidemic levels.
Community-based interventions are effective for promoting physical activity among older adults (aged 50 years and older).9 However, despite reasonable physical activity participation rates and relatively long study durations, few interventions have targeted specific behavioural- or program-based (eg, exercise frequency, intensity, mode, and duration)1,2,5 strategies that promote physical activity participation and adherence, and also prescribed dosing of activity to achieve health benefits. A particular challenge has been identifying the setting in which such coordinated, comprehensive interventions have the highest likelihood of success among those at risk.
The average Canadian adult makes about 3.1 visits to his or her family physician annually. For those aged 45 to 65 years, the average number of visits increases to 3.3, and for those aged 65 years or older, it increases to almost 6 visits per year.10 Similarly, Americans make an average of 1.6 visits to family physicians annually at age 15, compared with 6.3 per year for those older than 65.11 Hence, family physicians could potentially play a unique and important role in promoting healthy lifestyle changes in a large at-risk population. Further, organizations including the American Heart Association,12 the National Heart, Lung, and Blood Institute,13 the US Centers for Disease Control and Prevention,14 and the Canadian Task Force on Preventive Health Care15 have recommended that physicians should advise and counsel their patients to be physically active. In the United States, studies have shown that 28% of older adults reported receiving advice about physical activity from their family physicians in the previous 6 months,16 and only 36%17 to 48%18 reported that they had ever received such advice. In Canada, we found that 85% of family physicians reported asking patients about their physical activity levels, but only 26% assessed fitness in their patients and a few (11%) referred patients to others for assessment; 70% provided verbal counseling about exercise, and only 16% wrote exercise prescriptions.19 Most family physicians do not prescribe physical activity, resulting in a substantial care gap in a growing at-risk population.
Since we reviewed the literature between 1985 and 1998 on the effects of primary care physical activity counseling on fitness,20 results of additional studies of such counseling have been made available.2,21–23 Generally these have investigated behavioural theories (eg, social cognitive theories, transtheoretical model) and short-term (4 weeks to 6 months) monitoring of changes in physical activity levels or stages of adoption for physical activity. Although behavioural strategies have been found to increase physical activity participation, there is no evidence to indicate that this is associated with an increase in fitness. Further, most studies have used a range of physical activity outcome variables (and not fitness), relying on patient self-reports. Few studies2,24 have measured aerobic fitness, but those that did showed differing levels of improvement in fitness. The primary question in this study was whether the addition of behaviour counseling to an exercise prescription, tailored for family practice, resulted in greater improvement in fitness and secondary clinical outcomes than an exercise prescription alone did.
METHODS
Design
The Step Test Exercise Prescription Stage of change counseling (STEPS) study was a stratified, cluster randomized25 clinical trial in which the clusters, or units of randomization, were family physician practices. Eligible practices were stratified according to 2 variables: region (British Columbia, Alberta, Ontario, or Nova Scotia and New Brunswick) and setting (urban or rural). The 1:1 urban-rural stratum was a reflection of current practice distribution in Canada, while sampling in the 4 regions ensured generalizability across Canada.
Family physicians
A local physician coordinator from each region was approached by the principal investigator (R.J.P.) before the study during a national family medicine continuing education meeting. Family physicians agreeing to participate were randomized to either the intervention or the control group. Those family physicians randomized to the intervention group, along with members of their office staff, attended a 3-hour training session conducted by the principal investigator and a research assistant. The session was designed to increase physician and staff knowledge about the health benefits and risks of exercise among older patients; increase physician and staff knowledge about the stages of change model; and increase physician skill in individualizing prescription and counseling techniques for older patients. Family physicians in the control group attended a workshop designed to provide knowledge about treatment of hypertension and the importance of lifestyle as a foundation of treatment. For the purpose of the study, they were instructed to provide patients with exercise prescriptions according to our previously described Step Test Exercise Prescription intervention (exercise prescription without behavioural counseling).2 Both groups were given training on how to collect study outcomes. Family physicians received continuing medical education credits for their participation in the study and retained all study-related equipment and materials.
Patients
The study population consisted of healthy community-dwelling men and women aged 55 to 85 years who were patients at one of the participating family practices. Recruitment took place between August 2000 and January 2002. Patients were included if they met the following criteria: inactive lifestyle (energy expenditure less than 35 kcal/kg/d) determined using the 7-day physical activity recall (PAR) instrument26; readiness to increase their physical activity levels based on their stage of change (ie, not those in the maintenance phase); able to read and write English; and the absence of exclusionary medical conditions, including recent myocardial infarction or stroke, New York Heart Association class II to IV congestive heart failure, atrial flutter, uncontrolled hypertension (greater than stage 2), unstable angina, severe chronic obstructive pulmonary disease, uncontrolled diabetes mellitus, severe systemic or musculoskeletal disease preventing increased physical activity, or major psychiatric disease. During the recruitment phase of the study, office staff initiated recruitment with screening telephone calls to potential patients who were already scheduled to see the study physicians within the next 3 months. At the baseline visit, informed consent was obtained by the family physician, and questionnaires about psychosocial determinants of physical activity (ie, quality of life, self-efficacy, and stage of change) were administered. Measures of clinical outcomes (ie, blood pressure and body mass index [BMI]) were collected by trained staff members; then step tests, supervised by the family physicians, were performed to calculate predicted maximum oxygen consumption (pVO2max). Further data collection visits in the family practice occurred at 3, 6, 9, and 12 months after recruitment as well as through monthly staging done by telephone. The coordinating centre also conducted PAR telephone interviews at 3, 6, 9, and 12 months. Subjects reported any adverse events at each study visit. The study was approved by the Review Board for Health Sciences Research at the University of Western Ontario and local review boards in the participating regions.
Intervention
Patients in the STEPS and control groups received individualized exercise prescriptions based on submaximal step test results,2,27 but only patients in the STEPS group received counseling and support based on their stages of exercise behaviour.28 Family physicians in both groups developed exercise prescriptions by determining pVO2max from step test results and using these data to prescribe training heart rate (THR) intensities for patients; they also provided advice about appropriate frequency, intensity, type, and duration of exercise. Family physicians’ prescriptions for patients in the STEPS group were matched to patients’ current stages of adoption for physical activity.28
Measures
Primary outcomes
Aerobic fitness: Aerobic fitness was the primary outcome measure, determined by pVO2max using a step test protocol.27 Using a hand-held computer, the step test data (age, weight, sex, stepping time, and maximum heart rate [HRmax]) were used to predict VO2max using logistic regression, then to calculate a THR corresponding to 75% of pVO2max. Effort during the test was determined using the rate of perceived exertion (RPE) scale.29
Physical activity level: Physical activity was assessed as total energy expenditure (kcal/kg/d), estimated by the 7-day PAR, a widely used and validated26 instrument that classifies activities into 5 categories according to their intensity expressed as metabolic equivalents (or kcal/kg/h). The total time spent in the light physical activity category was obtained by subtracting hours in other activities and in sleep from 24 hours. The caloric expenditure per day was quantified by multiplying the total energy expenditure by the patient’s body weight in kilograms.
Secondary outcomes
Resting systolic (SBPrest) and diastolic (DBPrest) blood pressures and heart rate (HRrest) were measured using standard procedures. Two seated readings were taken 5 minutes apart and then averaged. Body mass index was calculated as body mass (in kilograms) divided by height (in metres squared).
Sample size calculation
We estimated that the sample size needed to be 320 patients from 4 regions, stratified by urban or rural practice setting within each region, based on our previous 12-month intervention2 of the exercise prescription program compared with control in sedentary older adults, which produced a 10% increase in pVO2max. We assumed a type I error rate of 5%, 80% power, standard deviation (σ) in pVO2max of 1.7 L/min, and a clinical difference (δ) in pVO2max of 2.5 L/min. To account for the effect of clustering, we used an intracluster correlation coefficient (ρ) of 0.025 for pVO2max and an attrition rate of 30%.
Statistical analyses
All analyses were performed with SAS for Windows. Analysis of variance (ANOVA) and χ2 tests were used to test for differences in baseline characteristics by treatment group. All patients were analyzed according to treatment group assignment. As patients were clustered by practice, and practices were randomized to treatment, we adjusted the variance among practices for nonindependence. The dependent variable was pVO2max, and the change from baseline to 12 months was analyzed with repeated-measures multifactorial ANOVA. Dropouts were not replaced, as we performed an intent-to-treat analysis. Post hoc secondary analyses were performed to examine the change in pVO2max by subgroups (sex, age, BMI, setting, and region). All data were reported as means and standard deviations or means and 95% confidence intervals (CIs). Statistical significance was preset at P < .05 for all analyses.
RESULTS
Sample population
Forty family physicians were recruited to participate in the study. Only 1 physician was recruited from a group practice setting. Twenty-one family physicians were randomized to the STEPS group and 19 to the control group. Seventeen of the physicians were male. Mean (SD) age of participating physicians was 48 (9) years and years in practice was 11 (6). Ten physicians were from British Columbia, 8 were from Alberta, 14 were from Ontario, and 8 were from Nova Scotia or New Brunswick, and there was an equal urban-rural distribution. The progress of patients through the study is shown in Figure 1. A total of 426 patients from these 40 family practices were screened for entry into the study between August 2000 and January 2002. Of these, 42 patients were excluded because they were already active and 24 declined participation. The final sample included 360 patients (84.5% of the screened sample). During the course of the study, 2 patients died owing to complications not related to the study, and 29 patients withdrew. The most common reasons for withdrawing were failure to complete study requirements, perception of a failure to meet their physicians’ expectations, and lack of time; 79% of patients who withdrew were from the STEPS group. Few adverse events were reported (primarily muscle soreness), and there was no difference in such events between groups.
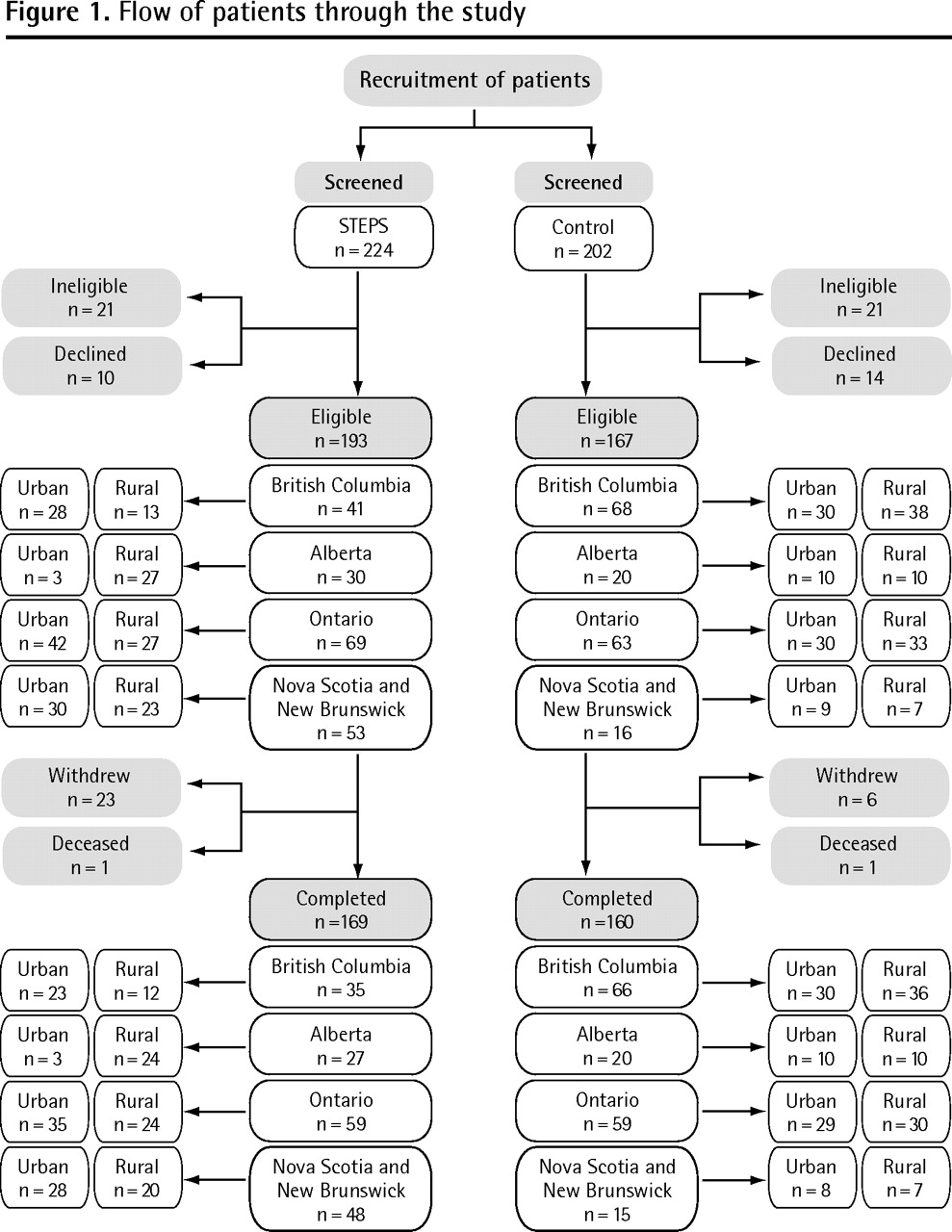
Flow of patients through the study
Demographic and clinical characteristics
All baseline characteristics and demographics, except for age, were similar between the STEPS and control groups (Table 1). Overall, mean (SD) age of participants was 64.9 (7.1) years (range 55 to 85 years).
Patient demographic and clinical characteristics at baseline: Comparisons of continuous means were performed using ANOVA; comparisons of categorical variables were performed using χ2 analysis.
Primary outcome
Change in fitness, pVO2max, and related exercise test variables are shown in Table 2. In the STEPS group, pVO2max increased 9.9% (95% CI 7.9% to 12.0%) at 12 months, and it increased 7.1% (95% CI 4.1% to 10.2%) in the control group (P < .001). However, the difference in the change in pVO2max between the treatment groups did not reach statistical significance. For the STEPS group, the greatest improvement in pVO2max (6.6%) occurred within the first 3 months, with sequential increases from previous measurement of 3.9% at 6 months and 1.7% at 9 months; the last 3 months served as a maintenance phase. The control group showed an increase in pVO2max of 4.9% within the first 3 months, with an additional increase of 5.8% at 6 months, followed by a slight decline of 1.0% in the last 6 months.
Mean changes in primary and secondary outcome variables in the STEPS and control groups at 12 months
At 12 months, HRmax and RPE significantly increased (P < .01) in both the STEPS and control groups, but there were no differences between groups. The stepping time significantly decreased (P < .001) in both treatment groups, but the STEPS group had a significantly greater decrease (P < .001) than the control group did.
Secondary measures
As shown in Table 2, at 12 months the control group’s mean HRrest had significantly increased (P < .05) and the STEPS group had a nonsignificant increase. The STEPS group had a 4.1–mm Hg reduction (P < .001) in systolic blood pressures compared with a 0.4–mm Hg in the control group at 12 months. The DBPrest significantly decreased (P < .05) in both the STEPS and control groups. Self-reported total energy expenditure (kcal/kg/d) significantly increased in both the STEPS and control groups; however, the STEPS group had a significantly greater increase compared with the control group (2.1% and 0.8%, respectively; P = .006). When mean (SD) energy expenditure was adjusted for body weight (kcal/d), there was still a significant increase (P < .001) at 12 months in the STEPS group (69.06 [169.87] kcal/d), whereas the control group did not change significantly (−6.96 [157.06] kcal/d).
Subgroup analyses
Sex differences
As seen in Table 3, the men in both treatment groups significantly increased (P < .001) pVO2max at 12 months, yet the change in pVO2max did not significantly differ between treatment groups. Among the women, only the STEPS group significantly increased pVO2max at 12 months (P < .001); therefore, the change in pVO2max was significantly different between the STEPS and control groups.
Mean changes in the STEPS and control groups at 12 months
Age differences
Those younger than 65 years of age (mean 59.4, SD 3.2 years) significantly increased pVO2max at 12 months (P < .001), yet there was no significant difference in the change in pVO2max between the STEPS and control groups.
Body composition differences
When patients were classified based on their baseline BMI (mean 34 kg/m2), all cohorts in both treatment groups, except for the normal (≤ 24.9 kg/m2) control group, significantly increased pVO2max at 12 months (P < .001).
Setting differences
Among participants in the urban settings (Table 3), both those in the STEPS group and those in the control group significantly increased pVO2max at 12 months (P < .001), and there was no difference between treatment groups. Similarly, among the rural settings, both the STEPS and control groups significantly increased pVO2max at 12 months (P < .001), although again the change was not significantly different between treatment groups.
Regional differences
In Alberta and Nova Scotia or New Brunswick (Table 3), the STEPS group significantly increased pVO2max at 12 months (P < .01), compared with the control group. However, these differences were not significantly different for either region. In Ontario and British Columbia, both the STEPS and control groups also significantly increased pVO2max at 12 months (P < .001); the change was not significantly different between intervention and control groups for Ontario, whereas British Columbia showed a significant difference between treatment groups (16.3% and 5.5%, respectively; P = .003).
DISCUSSION
In this study, family physicians from different regions across Canada were randomized to deliver an exercise prescription2 and behaviour counseling28 program (STEPS) among older adults compared with the exercise prescription (control) program alone.2 The principal finding from this study is that both the STEPS and control groups experienced significant and comparable improvement in pVO2max at 12 months compared with baseline measures. Examination of secondary outcomes revealed that SBPrest was reduced, while physical activity and energy expenditure levels were increased in both groups; these changes were significantly different between groups, favouring the STEPS treatment group from baseline to 12 months. Furthermore, the change in pVO2max differed by sex between groups—the change was greater among the women receiving the STEPS intervention—but not by age or between urban and rural community settings. These results are provocative and suggest that no overall difference in fitness is observed on the primary outcome when behaviour counseling is added to a tailored exercise prescription. However, changes in important secondary clinical variables such as systolic blood pressure, energy expenditure, and behaviour change favoured STEPS in both men and women, suggesting that the added behaviour counseling in STEPS might have benefits in some individuals beyond fitness alone.
Our exercise prescription and counseling approach differs from previous physician-based physical activity interventions2,19,21 because we combined physiologic (exercise prescription) and behavioural (stages of change) strategies. Further, the literature to date has largely focused on behavioural-based programs, self-reported physical activity levels, and short-term follow-up; few studies have used individualized exercise prescriptions based on fitness.2
At 6 months, pVO2max significantly improved in both groups; however, for the last 6 months, pVO2max appeared to continue to improve in the STEPS group, while the control group started to decline. This is in contrast to our previous study of the exercise prescription without behavioural counseling: although demonstrating an increase in pVO2max, similar to that identified in both groups in this study, the exercise prescription group in the initial study had not begun to decline at 12 months. The study population might have affected this outcome: the initial study was conducted in an academic family practice setting; this study was more generalized and was conducted across academic and community practices in urban and rural regions. Academic practices might have more resources for preventive care compared with nonacademic practices, although this was not explored in our studies. However, follow-up visits within the STEPS group provided ongoing motivational support, suggesting that behaviour has an important effect on longer-term fitness change.
It has been suggested that continuity of care in family practice offers opportunities to sustain individual motivation, assess progress, provide feedback, and adjust behaviour change plans30; therefore, the regular contact between physicians and patients might have contributed to the improvements observed. In the United States, telephone follow-up is popular and has been shown to be effective for achieving longer-term exercise adherence.9,31
Previous studies24 have supported our finding of fitness interventions having different effects on men and women. Why women and not men appeared to benefit from the addition of behavioural support requires further investigation. We previously2 showed that pVO2max significantly increased following exercise prescription only, compared with a control group receiving regular care, at 12 months (14% and 3%, respectively). In the Activity Counseling Trial,24 the addition of incentives (including electronic step monitors) and follow-up mailings or more intensive telephone counseling and classes resulted in smaller increases in pVO2max at 24 months for women (3.7% and 4.0%, respectively), compared with those who received only physician advice (−1.0%). For men in the Activity Counseling Trial, all intervention groups (advice, assistance, or counseling) increased their fitness levels at 6 months; however, this effect was no longer apparent at 24 months (−0.7%, 1.6%, and −0.2% change in pVO2max, respectively). Among the various strategies used to improve fitness, the exercise advice strategy, which required the fewest resources, was generally as effective for men as the behaviour change strategies requiring more resources. This might be important when generalizing the results to practice. Those who are most likely to benefit from more intervention (ie, women) could be triaged to receive this from allied health professionals.
Secondary outcomes
The secondary aim of our study was to determine whether the intervention caused changes in clinical measures and physical activity levels. It is well established that SBPrest and DBPrest increase with age among adults in North America.32 Our findings showed that the STEPS group clinically and statistically decreased SBPrest and DBPrest by more than 2 mm Hg. In a meta-analysis, Kelley and Kelley33 reported on the efficacy of aerobic exercise training programs, similar to this community-based fitness program in older adults, for reducing SBPrest. Reducing DBPrest by as little as 2 mm Hg could lower the prevalence of hypertension by 17% and the risk of stroke and transient ischemic attack by 15%.34
Expending an additional 1000 kcal per week is associated with a 20% to 30% reduction in risk of all-cause mortality compared with sedentary men and women.4,5 Our study showed that the mean (SD) increase in energy expenditure in the STEPS group (483.45 [1189.06] kcal/wk) was greater than that in the control group (−48.69 [1099.45] kcal/wk) at 12 months. Four previous primary care physical activity interventions21–24 have reported significant changes in self-reported physical activity for a follow-up period greater than 6 months (P < .05); however, 3 of these studies did not measure changes in fitness. Overall, these beneficial changes in blood pressure, physical activity levels, and physical fitness suggest that exercise prescription and counseling delivered by family physicians could increase the proportion of patients meeting physical activity goals to improve cardiovascular health.
In Canada, a perception exists that living in urban environments or western provinces might be associated with better fitness and health.6 In this study, delivery of exercise prescription in either urban or rural settings improved pVO2max in both groups at 12 months, yet there were no differences between treatment groups. At the regional level, pVO2max improved in the STEPS group for all 4 regions, whereas the control group only showed improvements in Ontario and British Columbia. As well, British Columbia was the only region to show a significant difference between treatment groups at 12 months. Therefore, geographic location (region) might play a role in improvements in aerobic fitness; community setting (urban vs rural) does not appear to play a role. This might corroborate observed differences in cardiovascular health and fitness in different parts of Canada, and could be related to differences in socioeconomic, environmental, and health resources.8
Study strengths and limitations
The main strengths of this study include the fact that it was conducted in a range of Canadian primary care practices (making the findings more generalizable); the long duration of follow-up; use of a large, older population sample (with similar baseline characteristics in both groups); inclusion of both energy expenditure and fitness outcome measures; and randomization cluster by practice to reduce the risk of intervention contamination. The study is limited by the fact that it did not include a “no treatment” control group, but rather compared the intervention with a previously described exercise prescription delivered in a rather homogeneous setting. There were more dropouts from the intervention group than from the control. Although this could relate to the greater time required to deliver the intervention (approximately 10 minutes more per visit), we did not find any other explanations for this discrepancy.
Gains in pVO2max in both groups might have been the result of the Hawthorne effect. The fact that all patients initially consented to participate in a study that would prescribe and counsel about exercise with the goal of increasing physical activity and improving fitness might have biased the outcome. Further, we did not assess compliance with the intervention, as THR achieved during exercise sessions and validation of proper pulse-palpation techniques were not quantified. However, we did measure RPE (Borg score), PAR, stage of change, and pVO2max, which would likely only show improvements if patients were indeed exercising. Given that our exercise prescription intervention requires only minimal training and equipment and can be completed within a typical 15-minute office appointment suggests that it could be implemented in a range of practices.
Conclusion
This study has shown that routine exercise prescription with or without behaviour counseling every 3 months by family physicians among sedentary, but otherwise healthy, older adults can make substantial improvements in pVO2max for at least a year. Addition of staged behavioural support to our exercise prescription appeared to improve important clinical measures and might promote better long-term behaviour and outcomes among some patients. Thus, if implemented widely, STEPS could aid public health efforts to reduce the prevalence of sedentary lifestyles and might be a clinically effective and economical means of reducing cardiovascular risk.
Acknowledgments
This study was supported by an operating grant from the Heart and Stroke Foundation of Canada. We are also indebted to the physician coordinators, physician participants, their staff, and more important, their patients.
Notes
EDITOR’S KEY POINTS
-
This study showed that routine exercise prescription with or without behaviour counseling among sedentary, but otherwise healthy, older adults can make substantial improvements in fitness, as measured by maximum predicted oxygen consumption, for at least a year.
-
The addition of stages of change behavioural support to the exercise prescription appeared to improve important clinical measures, such as systolic blood pressure, energy expenditure, and behaviour change, and might promote better long-term behaviour and outcomes among some patients. Because women seem to benefit from the addition of behavioural counseling, they could be triaged to receive this from allied health professionals.
POINTS DE REPÈRE DU RÉDACTEUR
-
Cette étude a montré qu’une simple prescription d’exercice, avec ou sans counseling comportemental, chez des sujets âgées sédentaires mais par ailleurs sains peut entraîner une amélioration importante pendant au moins un an de la condition physique, telle que mesurée par la consommation maximale d’oxygène.
-
L’addition d’un counseling comportemental à la prescription d’exercice a apparemment amélioré certains paramètres cliniques importants, tels la tension artérielle systolique, la dépense énergétique et un changement de comportement, ce qui, pour certains patients, pourrait favoriser des issues et un comportement meilleurs à long terme. Comme les femmes semblent bénéficier de l’addition de counseling comportemental, certaines d’entre elles pourraient éventuellement en recevoir de professionnels de la santé intéressés.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
The abstract of this study was previously published as Lattanzio CN, Petrella RJ, Shapiro S, Overend T. Effects of a physician-based exercise counseling program for improving aerobic fitness in older adults. Med Sci Sports Exerc 2009;41(5 Suppl 1):364. Republished with permission.
-
Un résumé de cette étude a déjà été publié en anglais par Lattanzio CN, Petrella RJ, Shapiro, S et Overend T sous le titre : Effects of physician-based exercised counseling program for improving aerobic fitness in older adults. Med Sci Sports Exerc 2009;41 (5 Suppl 1) :364. Publié à nouveau avec permission.
-
Contributors
Drs Petrella, Lattanzio, and Overend and Ms Shapiro contributed to concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Are family medicine residents trained to counsel patients on physical activity? The Canadian experience and a call to action
- ABC of prescribing exercise as medicine: a narrative review of the experiences of general practitioners and patients
- Longitudinal qualitative study describing family physicians experiences with attempting to integrate physical activity prescriptions in their practice: 'Its not easy to change habits
- Can certified health professionals treat obesity in a community-based programme? A quasi-experimental study
- Counseling on physical activity to promote mental health: Practical guidelines for family physicians
- Promouvoir la sante mentale par un counseling sur l'activite physique: Lignes directrices pratiques pour les medecins de famille
- The miracle drug