


Abstract
OBJECTIVE To review the management of bariatric surgical patients.
QUALITY OF EVIDENCE MEDLINE, EMBASE, and Cochrane Library databases were searched, as well as PubMed US National Library, from January 1950 to December 2009. Evidence was levels I, II, and III.
MAIN MESSAGE Bariatric surgery should be considered for obese patients at high risk of morbidity and mortality who have not achieved adequate weight loss with lifestyle and medical management and who are suffering from the complications of obesity. Bariatric surgery can result in substantial weight loss, resolution of comorbid conditions, and improved quality of life. The patient’s weight-loss history; his or her personal accountability, responsibility, and comprehension; and the acceptable level of risk must be taken into account. Complications include technical failure, bleeding, abdominal pain, nausea or vomiting, excess loose skin, bowel obstruction, ulcers, and anastomotic stricture. Lifelong monitoring by a multidisciplinary team is essential.
CONCLUSION Limited long-term success of behavioural and pharmacologic therapies in severe obesity has led to renewed interest in bariatric surgery. Success with bariatric surgery is more likely when multidisciplinary care providers, in conjunction with primary care providers, assess, treat, monitor, and evaluate patients before and after surgery. Family physicians will play a critical role in counseling patients about bariatric surgery and will need to develop skills in managing these patients in the long-term.
Recent estimates from the 2004 Canadian Community Health Survey show that 59% of the adult population is overweight and 1 in 4 (23%) adults is obese.1 The obesity rate has increased dramatically in the past 15 years: between 2% and 10% among boys and between 2% and 9% among girls.2,3 Moreover, it is estimated that 1 in 10 premature deaths among Canadian adults aged 20 to 64 years is directly attributable to obesity.4
The limited long-term success of behavioural and pharmacological therapies in patients with severe obesity has led to a renewed interest in bariatric (obesity) surgery in Canada.5 Currently, several provinces are attempting to improve access to bariatric surgery programs. In the near future it is anticipated that more than 4000 to 5000 patients will undergo bariatric surgery in Canada; as such, family physicians will play a critical role in counseling patients regarding the need for bariatric surgery and will need to develop skills in managing these patients in the long-term.
The aim of this review is to inform family doctors about some of the key issues relevant to the management of bariatric surgical patients.
Quality of evidence
We performed an electronic literature search of MEDLINE, EMBASE, and Cochrane Library databases, as well as the PubMed US National Library, from January 1950 to December 2010. We used the search terms bariatric surgery, obesity surgery, gastric band, gastric bypass, sleeve gastrectomy, and gastroplasty in combination with weight gain or weight loss or nutrition. Studies were limited to the English language, adult populations, and human subjects. Google was also used to search for gray literature. We defined our inclusion criteria as randomized controlled trials, meta-analyses, case reports, non-randomized control trials, reviews, and retrospective and prospective case series. Studies only reporting surgical techniques or without follow-up outcomes were excluded. Evidence was levels I, II, and III.
Levels of evidence
-
Level I: At least one properly conducted randomized controlled trial, systematic review, or meta-analysis
-
Level II: Other comparison trials, non-randomized, cohort, case-control, or epidemiologic studies, and preferably more than one study
-
Level III: Expert opinion or consensus statements
Indications for bariatric surgery
In 1991, the National Institutes of Health published specific indications for the appropriateness of bariatric surgery6–8:
Surgical intervention is an option for carefully selected patients with clinically severe obesity (BMI [body mass index] ≥ 40 or ≥ 35 kg/m2 with comorbid conditions) when less invasive methods of weight loss have failed and the patient is at high risk for obesity-associated morbidity or mortality.
Gastrointestinal surgery … can result in substantial weight loss, and therefore is an available weight loss option for well-informed and motivated patients with a BMI ≥ 40 or ≥ 35, who have comorbid conditions and acceptable operative risks.
Patients opting for surgical intervention should be followed by a multidisciplinary team ….
Lifelong medical surveillance after surgical therapy is a necessity.8
Based upon the National Institutes of Health criteria, many adults might meet the criteria for assessment for bariatric surgery. In addition to these recommendations, the following factors need to be taken into account when considering bariatric surgery:
Weight-loss history
It must be documented that conventional weight-loss attempts have been tried and have not been successful over time. Medical necessity for bariatric surgery should be documented.9
Accountability and responsibility
The individual needs to demonstrate adherence to recommendations by attending appointments, practising self-monitoring with record-keeping, making time for healthy eating and activity, taking medication, and completing bloodwork.
Comprehension and understanding
The individual must have an understanding of the benefits and limitations of a surgical procedure to assist with management of his or her obesity.
Acceptable level of risk
The risks of surgical intervention must not be excessive and must be lower than the risks of not providing the treatment.7,9,10
Box 16–9 shows exclusion criteria for patients who should not be offered bariatric surgery.
Exclusion criteria for bariatric surgery
Patients who are or have any of the following should not be offered bariatric surgery:
|
Options for bariatric surgery
There are 3 main types of bariatric surgical procedures categorized by function: restrictive; combined (restrictive and malabsorptive), and primarily malabsorptive. All procedures are considered permanent. The following is a brief overview of bariatric surgeries:
Restrictive procedures
Laparoscopic adjustable gastric banding (LAGB) (Figure 1A): Laparoscopic adjustable gastric banding employs laparoscopic insertion of a silicone gastric band at the upper end of the stomach, creating a small proximal gastric pouch with a volume of approximately 30 mL. This band is connected via a tube to a subcutaneously placed injection port. The band is inflated with a saline solution to achieve an appropriate narrowing to effect sufficient early satiety, which will sustain moderate weight reduction. The degree of inflation is customized to each individual.11
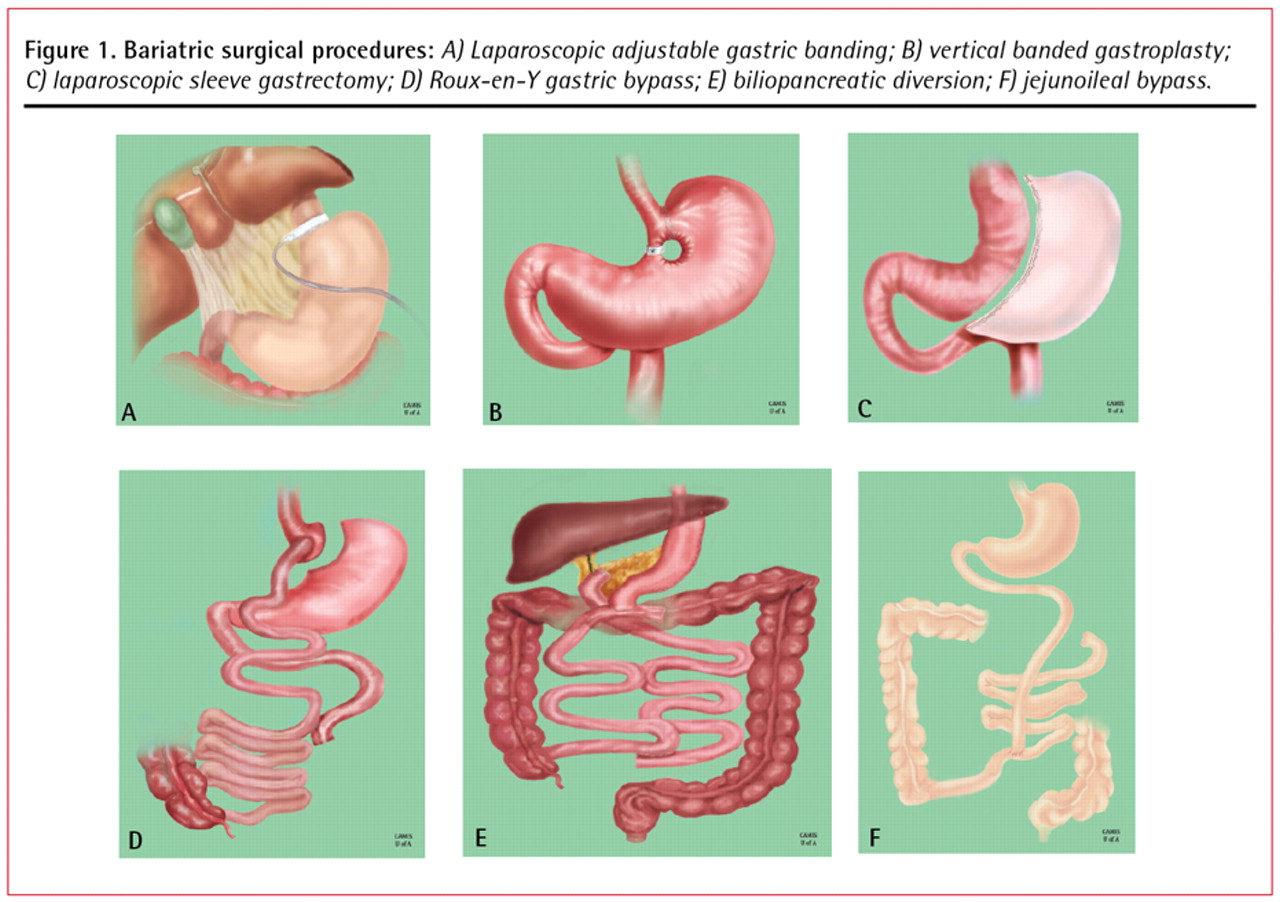
Bariatric surgical procedures: A) Laparoscopic adjustable gastric banding; B) vertical banded gastroplasty; C) laparoscopic sleeve gastrectomy; D) Roux-en-Y gastric bypass; E) biliopancreatic diversion; F) jejunoileal bypass.
Vertical banded gastroplasty (Figure 1B): This operation involves stapling the stomach, front to back, below the gastroesophageal junction and 1 cm from the lesser curvature. A vertical staple line is then made from the opening to the left side of the gastroesophageal junction, and the outlet stoma is restricted with a 1-cm diameter polypropylene band.12 The band mechanically restricts food intake, creating an early sense of satiety that limits intake. Because of the higher-than-expected complication rate, vertical banded gastroplasty is no longer routinely performed.
Laparoscopic sleeve gastrectomy (LSG) (Figure 1C): Rather than a pouch, this procedure creates a “sleeve” of the stomach, extending from the esophagus to the duodenum. The size of the gastric sleeve is approximately 60 to 120 mL. The gastric remnant, approximately 80% of the stomach, is removed. Production of ghrelin, a hormone involved in appetite, is reduced, resulting in decreased hunger and improved satiety.13 Sleeve gastrectomy remains an investigational procedure in our institute (ie, University of Alberta) to determine safety and long-term outcomes.
Combined restrictive and malabsorptive procedures
Roux-en-Y gastric bypass (RYGB) (Figure 1D): Roux-en-Y gastric bypass involves construction of a small (30 mL) proximal gastric pouch by stapling and dividing the stomach. The pouch empties into a segment of the jejunum that is brought up to the gastric pouch as a Roux-en-Y limb. Although the gastric bypass is considered a restrictive procedure, it causes some malabsorption as a consequence of the bypassed stomach, duodenum, and upper jejunum.
Biliopancreatic diversion with or without duodenal switch (Figure 1E): This procedure combines removal of a small section of stomach with alterations to the path of the small intestine. Complication rates are higher and include malabsorption, protein malnutrition, vitamin and mineral deficiencies, anemia, osteoporosis, and anastomotic ulceration.14
Malabsorptive procedures
Malabsorptive procedures decrease absorption of nutrients by decreasing the length of small intestine that is exposed to food. Malabsorptive procedures produce substantial weight loss but also have the highest complication rates.
Jejunoileal bypass (Figure 1F): The upper small intestine is joined to the distal small intestine, effectively removing a large segment of the absorptive circuit, while retaining only about 35 cm of normal absorptive small intestine. Malabsorption of both macronutrients and micronutrients can contribute to severe malnutrition and related complications including organ (eg, liver, kidney) failure and mortality. This procedure is no longer recommended owing to high complication rates and poor long-term outcomes.9,14
Complications
Mortality rates are less than 1% for patients with BMIs less than 50 kg/m2 who are younger than 55 years of age.14 For patients with BMIs greater than 60 kg/m2, who also have comorbid conditions, the mortality rate is 2% to 4%. Lower risk of morbidity and mortality are positively correlated with surgical volume at the clinic (> 100 cases per year), surgeon experience, surgery at a tertiary care facility, sex of patient (female), age of patient (< 55 years), and respiratory status.10
Average bariatric surgical complication rates are less than 10%.15 A bariatric surgical patient differs from the average general surgery patient in that complications might present with minimal physical signs and symptoms, the patient is difficult to evaluate owing to his or her body habitus and inability to fit on many diagnostic examination tables, and the patient deteriorates rapidly and has very little reserve to weather a catastrophic illness. The best opportunity to improve outcomes is in the first 6 to 12 hours, and after 24 hours the risk of morbidity and mortality escalate rapidly.16
Early complications
Anastomotic or staple line leak
The overall incidence of an anastomotic leak after RYGB is 1.2% to 3%.17 The clinical presentation can be quite insidious and a high degree of suspicion is required by the physician. Sustained tachycardia (especially a sustained heart rate of >120 beats per minute), tachypnea, and fever raise the suspicion. Diagnostic tests such as upper gastrointestinal series and computed tomography detect only 22% of anastomotic leaks and tend to be very operator-dependent.17 The key diagnostic or therapeutic maneuver is prompt surgical intervention with a second look with diagnostic laparoscopy or laparotomy.17
Postoperative bleeding
There is approximately a 3.1% incidence of bleeding after bariatric surgery.18 Twenty-two percent of bleeds stop spontaneously, 55% necessitate blood transfusion, and 22% require operative intervention.18 Active bleeding often presents within 6 hours of the operative intervention and manifests with bright red bleeding orally, rectally, or abdominally, with possible hypotension and tachycardia. Prompt surgical or endoscopic intervention is required. Delayed bleeding often presents several days postoperatively with dark blood either within surgical drains or passed orally or rectally. Delayed bleeding often does not present with symptoms of hemodynamic instability, and the physician can pursue diagnostic maneuvers such as radiologic, hematologic, and endoscopic evaluation.
Late complications
All procedures
Nausea or vomiting: Nausea or vomiting can be improved for most patients with education regarding food selection and eating behaviour. Patients with protracted vomiting should be assessed for strictures, obstructions, overinflated LAGB, or other differential diagnoses (eg, pregnancy). Patients with persistent or protracted vomiting should be screened for thiamine deficiency and given supplements if neurologic symptoms present.9
Excess or loose skin: Excess or loose skin is a common, unwanted side effect of substantial weight loss. Mobility and self-care might be impaired. Infection and ulcerations might develop. Referral to a bariatric physician or occupational or physical therapist is recommended.
Small bowel obstruction: Small bowel obstruction might present as abdominal bloating, cramping, or pain and nausea to severe pain and emesis. It might be due to adhesions, internal hernias, or severe constipation.
Ulcers: Ulcers of the stomach or anastomosis (marginal ulcers) might present as upper epigastric pain or burning that can radiate to the back, with symptoms of nausea or vomiting and food intolerances. Iron deficiency anemia is commonly associated with chronic ulcers.19
Restrictive procedures
Erosion or slippage of the band: Erosion or slippage of the band might occur. Patients might present with symptoms of proximal gastric outlet obstruction (eg, dysphagia, nausea, vomiting, inability to tolerate solid food, or abdominal pain or discomfort) with possible excessive weight loss. Referral to a bariatric surgeon is recommended.
Leakage from port or band tubing (with LAGB): Patients report feelings of fullness or satiety initially after a fill, but complete loss of this sensation and a substantial increase in volume of solid food tolerated occurs within a few days. Weight regain or poor weight-loss outcome might occur.
Combined procedures
Anastomotic stricture: Anastomotic stricture might occur during healing as scar tissue develops. Strictures might be suspected if a recent surgical patient (ie, RYGB) who had previously been tolerating oral intake now reports consistent and progressive nausea and vomiting with solid foods and is able to tolerate only small amounts of liquids at a time. Referral to a registered dietitian and bariatric surgeon is recommended.
Gastrogastric fistulae: Gastrogastric fistulae might develop owing to failure or incomplete staple partition of the pouch.14 Patients might present with tolerance of high volumes of solid food, lack of restriction, lack of satiety, tolerance to textures commonly difficult after bariatric procedures (eg, sticky, doughy, stringy, tough), and either weight regain or poor weight-loss outcome. Referral to a bariatric surgeon is recommended.
Dumping syndrome: Dumping syndrome occurs when food enters the small intestine, bypassing the stomach. Dumping syndrome can occur after bariatric surgery for combined or primary malabsorptive procedures. Early symptoms (within 30 minutes after eating) occur when food and fluid pass into the small intestine too fast. Symptoms might include nausea, vomiting, stomach pain or cramping, diarrhea, feelings of fullness or bloating, or increased heart rate. Late symptoms (1 to 3 hours after eating) occur when there are changes in the amounts of insulin and sugar in the blood (ie, reactive hypoglycemia). Late symptoms might also include flushing or sweating, intense need to lie down, feeling weak or dizzy, feeling nervous or shaky, or a drop in blood pressure.
Outcomes after surgery
Weight loss
Outcomes after bariatric surgery are often reported as the percentage of excess weight lost (EWL). Excess weight is the total amount of weight above a reference standard for “ideal” weight (ie, BMI of 24.9 kg/m2). Table 115,20–25 summarizes the literature reports on weight loss after each option for bariatric surgery. Weight-loss outcomes (ie, percentage of EWL) might not be significantly different at 5 years or more after surgery, regardless of the procedure. The weight-loss targets after bariatric surgery are not to achieve a “normal” weight based on height and weight reference tables or BMI ranges. The most important outcomes are resolution of comorbid conditions and improvement in quality of life.
Weight loss after bariatric surgery
Inadequate weight loss (< 30% EWL) or weight regain (> 10% EWL) might be an indication of surgical or technical failure (ie, loss of integrity of gastric pouch), lack of proper adjustment to an LAGB, maladaptive eating behaviour, or psychological complications. Investigations and referral to the bariatric team are recommended.9
Up to 30% of people who have bariatric surgery might experience substantial weight regain. Box 2 presents several factors that can contribute to weight increase. It is important to continue interventions including nutrition and activity counseling, behaviour modification, and medical management, as surgical treatment alone is not successful. Weight regain might be related to technical failures of the surgery and should be reassessed by the bariatric surgeon.
Factors contributing to weight regain
Factors contributing to weight regain include the following:
|
Factors contributing to tolerance of an increased volume of solid food, which might lead to weight regain, include the following:
|
LAGB—laparoscopic adjustable gastric banding, RYGB—Roux-en-Y gastric bypass.
Comorbidity resolution
Successful treatment of obesity dramatically ameliorates the comorbidities associated with obesity. Type 2 diabetes, for example, was eliminated by gastric bypass in 82% of obese patients.26 Similarly, gastric bypass surgery effectively controls sleep apnea in many patients.27–29 Hypertension has shown an excellent response to gastric restrictive surgery (LAGB), disappearing in half to two-thirds of patients with obesity-related hypertension.27,30 Similarly in both meta-analysis and by weighted means, hyperlipidemia, hypercholesterolemia, and hypertriglyceridemia were significantly improved across all surgical procedures (P < .01).25,27 In studies of patients with class 1 or class 3 obesity who had symptoms of gastroesophageal reflux disease, gastric bypass operations consistently improved both symptoms and monitoring values.31,32
Finally, although data on the effect of LSG on comorbidity resolution are limited, short-term data demonstrating a beneficial effect on the metabolic syndrome have been published.33
Postsurgery follow-up
All bariatric patients are assessed by the surgeon 3 weeks after surgery to assess surgical wound healing and to rule out immediate postoperative complications (eg, abscess, infection, hernia). Thereafter, surgeon visits are scheduled every month for LAGB patients for band fills and every 3 months for RYGB and LSG patients (Table 2). Each visit focuses on weight loss and comorbidity resolution. Furthermore, close attention is paid to determining changes in blood pressure, blood glucose levels, and mental health.
Follow-up recommendations after bariatric surgery
The registered dietitian sees all patients at 6 weeks, 3 months, and then every 3 months for the first year. Each visit includes a thorough assessment of caloric and protein intake and an overall nutritional assessment.
Bloodwork (ie, complete blood count with differential, electrolytes, fasting blood glucose, hemoglobin A1c, fasting lipid panel, creatinine, urea, albumin, alanine aminotransferase, bilirubin, ferritin, vitamin B12, 25-hydroxyvitamin D, parathyroid hormone, calcium) is ordered at 3 months, 6 months, 1 year, and 18 months for RYGB and LSG patients. Laparoscopic adjustable gastric banding patients have the same bloodwork drawn at 6 months and 1 year. Annual bloodwork is then ordered on all patients thereafter.
Follow-up in our centre is lifelong, but visits with the surgeon and the registered dietitian are spread out to every 6 months after the first year.
Nutrition and supplementation
Patients should follow a well-balanced, calorie-reduced diet as part of a comprehensive weight management strategy. Box 334 shows some nutritional recommendations after bariatric surgery.
Nutrition recommendations after bariatric surgery
|
Adapted from Aills et al.34
Vitamin and mineral supplementation is recommended for all restrictive procedures and is a lifelong requirement for combined or malabsorptive procedures. Bloodwork is recommended to detect and monitor for vitamin and mineral deficiencies with attention to iron (ie, complete blood count with differential, ferritin, iron, total iron-binding capacity, and percent of oxygen saturation), folic acid (folate), bone health (25-hydroxyvitamin D, calcium, and parathyroid hormone), and vitamin B12. Referral to a registered dietitian for nutrition counseling and supplementation is recommended.
Conclusion
The commonly held belief that obese individuals can lose weight by simply “eating less and moving more” is flawed and not supported by the literature.6 Bariatric surgery should be considered for patients who have not achieved adequate weight loss with lifestyle and medical management who are at high risk of morbidity and mortality, and who are suffering from the complications of obesity. Success with bariatric surgery is more likely when multidisciplinary health care providers, in conjunction with primary health care providers, assess, treat, monitor, and evaluate individuals both before and after surgery.4,6,7,9 Family physicians should use the expertise of their multidisciplinary care team to promote and manage the health of their bariatric surgical patients. Further information that outlines procedures offered and referral methods can be obtained from the Canadian Obesity Network (www.obesitynetwork.ca) and the Canadian Association of Bariatric Physicians and Surgeons (www.cabps.ca).
Notes
EDITOR’S KEY POINTS
-
The rising incidence of obesity, as well as the increasing number of those who have undergone bariatric procedures, will lead to more family physicians seeing more patients with questions about bariatric surgery.
-
Lifestyle change is critical to success following surgery, and patients will require lifelong support to achieve this.
-
A high index of suspicion is essential when abdominal pain, nausea, or vomiting occur in patients who have had bariatric surgery. Referral to an obesity clinic is recommended.
-
Patients must remain on the recommended supplements for a lifetime. Routine laboratory assessment is essential to determine nutritional status.
POINTS DE REPÉRE DU RÉDACTEUR
-
Compte tenu de l’augmentation de l’incidence de l’obésité et du nombre croissant de personnes ayant subi une intervention bariatrique, les médecins de famille auront de plus en plus à répondre à des questions au sujet de ces interventions.
-
Un changement du mode de vie est essentiel pour que ces interventions réussissent, et les patients auront besoin de support toute leur vie pour y arriver.
-
Il y a lieu d’être extrêmement attentif chez un patient qui présente douleur abdominale, nausées ou vomissements après une intervention bariatrique. Un tel patient devra être dirigé à une clinique d’obésité.
-
Les patients doivent respecter les suppléments recommandés pour le reste de leur vie. Des examens de laboratoire doivent aussi être faits régulièrement pour vérifier leur état nutritionnel.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Contributors
All authors contributed to the literature search and preparation of the article for submission.
-
Competing interests
None declared
-
This article is eligible for Mainpro-M1 credits. To earn credits, go to www.cfp.ca and click on the Mainpro link.
- Copyright© the College of Family Physicians of Canada





{kind=link}