


Spirometry in primary care [CD-ROM]. Toronto, ON: The Lung Association; 2007.
Clinical question
Does the commonly promoted spirometry interpretation algorithm1 allow clinicians to diagnose chronic obstructive pulmonary disease (COPD) and is the definition of reversibility of airflow obstruction used appropriately?
Reassessing a widely recognized algorithm
Members of the Primary Care Respiratory Alliance of Canada have undertaken a critical appraisal of a spirometry interpretation algorithm that is a component of an interactive CD-ROM titled Spirometry in Primary Care.1 This CD-ROM is produced by the Ontario Lung Association and endorsed by the Ontario Thoracic Society, the Ontario Respiratory Care Society, and the Family Physicians Airways Group of Canada. The interactive CD-ROM includes both didactic and case-based learning strategies. Physicians using the CD-ROM are eligible for Mainpro-C credits from the College of Family Physicians of Canada. It should be noted that this algorithm can be used for both adults and children, although some school-aged children might not meet international criteria for spirometry.2
Overview and analysis of CD-ROM algorithm
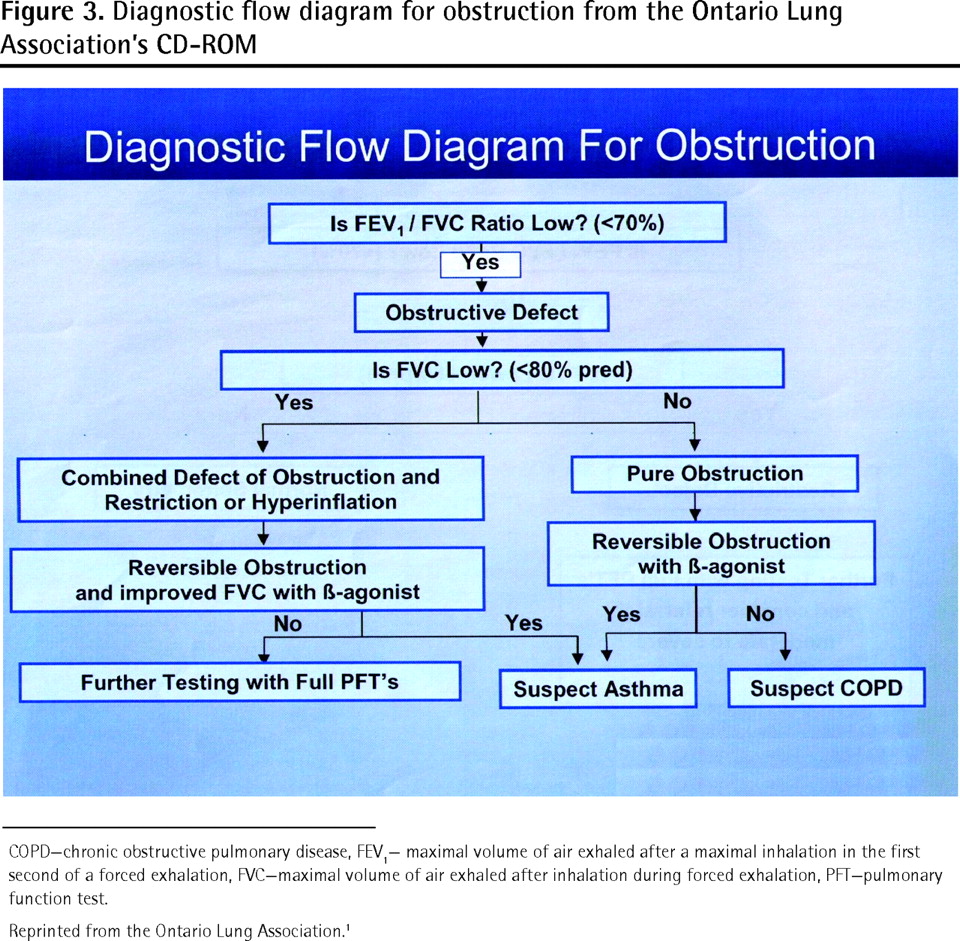
While the algorithm in question (Figure 3)1 identifies airway obstruction as a reduction in the ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) before bronchodilator challenge, there is no mention of the postbronchodilator FEV1-FVC ratio. As a result, a spirometric diagnosis of COPD cannot be established without an unprompted search for the postbronchodilator FEV1-FVC ratio measurement by the person interpreting the spirometry tests.

Diagnostic flow diagram for obstruction from the Ontario Lung Association’s CD-ROM
COPD—chronic obstructive pulmonary disease, FEV1— maximal volume of air exhaled after a maximal inhalation in the first second of a forced exhalation, FVC—maximal volume of air exhaled after inhalation during forced exhalation, PFT—pulmonary function test.
Reprinted from the Ontario Lung Association.1
A spirometric diagnosis of acute airway obstruction (assuming the ratio returns to normal) is also difficult to obtain without an unprompted search by the person interpreting the tests. Because the algorithm should serve as a stand-alone document, the absence of a logic string linked to the postbronchodilator FEV1-FVC ratio limits its usefulness, particularly because some clinicians might not be familiar with the spirometric criteria for COPD diagnosis.
In the interactive CD-ROM, reversibility is defined as an improvement in the prebronchodilator FEV1 value (that had been below normal levels) by 12% and 180 mL after β2-agonist challenge. This definition is used to guide the user to suspect either asthma or COPD; COPD is suspected if the reversibility criterion is not met. There are 2 problems with this approach: current COPD guidelines require a reduction in the postbronchodilator FEV1-FVC ratio for diagnosis, and changes in FEV1 after bronchodilator challenge are not included in the spirometric diagnostic criteria for COPD.3 It is well established that most patients who meet the spirometric diagnosis of COPD also meet the FEV1 reversibility criteria outlined in the algorithm and in asthma management guidelines.4 Given the phenotypic overlap between asthma and COPD, the current algorithm could lead the user to suspect asthma in many cases of COPD.
Relevance to family physicians
Spirometry provides the only simple, office-based objective test to distinguish between asthma and COPD. Guidelines on asthma management4 recommend an increase of 12% and of at least 200 mL in the FEV1 after bronchodilator challenge to support a diagnosis of asthma. A spirometric diagnosis of COPD is suspected when the FEV1-FVC ratio remains consistently below 0.70 after bronchodilator challenge.3 A spirometry interpretation algorithm should allow physicians to determine whether patients meet spirometric criteria for asthma4 and COPD3 or both and should recognize that spirometry alone cannot confirm a clinical diagnosis.
Application to clinical practice
Four brief spirometry cases, all meeting American Thoracic Society5 criteria for acceptability and reproducibility, highlight how the algorithm could influence interpretation of the spirometric data.
Case 1
The prebronchodilator and postbronchodilator FEV1-FVC ratios are 0.79 and 0.82, respectively (Figure 2 on page 1151). The CD-ROM algorithm (Figure 3) would consider the prebronchodilator FEV1-FVC ratio normal and would not indicate a bronchodilator challenge test. A newly proposed algorithm (Figure 1 on page 1149)6 would recommend bronchodilator challenge despite a normal FEV1-FVC ratio, revealing an improvement in FEV1 from 2.92 to 3.29 L (increase of 370 mL and 13%). The new algorithm6 indicates that these data are consistent with asthma given the improvements in FEV1 after bronchodilation. The patient in this case was a 45-year-old man who had never been a smoker. He had intermittent bouts of shortness of breath and chest tightness and normal results from cardiovascular workup. His response to asthma therapy was favourable.
Case 2
The prebronchodilator and postbronchodilator FEV1-FVC ratios are 0.48 and 0.50, respectively (Figure 2 on page 1151). The prebronchodilator and postbronchodilator FEV1 results are 1.52 and 1.88 L, respectively (increase of 360 mL and 24%). The CD-ROM algorithm would consider the reduction in prebronchodilator FEV1-FVC ratio as possibly being related to a combined defect of obstruction and restriction or hyperinflation because the FVC is also reduced (Figure 4). Given that the FVC improved and the FEV1 increased with use of a β2-agonist (according to reversibility criteria),4 the user is led to suspect asthma. The new algorithm6 recognizes the reduction in FEV1-FVC before bronchodilator use, but the postbronchodilator FEV1-FVC ratio is evaluated to determine whether there is a combined defect of obstruction and restriction or hyperinflation. Given that the FVC increased to more than 80% of the predicted value with bronchodilation, it becomes clear that hyperinflation contributed to the reduced prebronchodilator FVC measurement. Because the postbronchodilator FEV1-FVC ratio remains below 0.70 and the FEV1 reversibility criterion is met, the clinician is led to differentiate asthma from COPD using historical data.6 The patient in this case is a 73-year-old man with a 40-pack-year smoking history, no allergies to environmental factors, and a history of progressive shortness of breath over the past 10 years. The medical history and family history were otherwise unremarkable for asthma risk factors. The historical and spirometric data in this case are consistent with a clinical diagnosis of COPD.

Diagnostic flow diagram for restriction from the Ontario Lung Association’s CD-ROM
FEV1— maximal volume of air exhaled after a maximal inhalation in the first second of a forced exhalation, FVC—maximal volume of air exhaled after inhalation during forced exhalation, PFT—pulmonary function test.
Reprinted from the Ontario Lung Association.1
Case 3
The prebronchodilator and postbronchodilator FEV1-FVC ratios are 0.47 and 0.50, respectively (Figure 2 on page 1151). The prebronchodilator and postbronchodilator FEV1 values are 1.65 and 1.94 L, respectively (increase of 290 mL and 18%). The CD-ROM algorithm guides the clinician to consider a pure obstruction because the prebronchodilator FEV1-FVC ratio is reduced and the FVC measurement is normal (Figure 3). The reversibility in FEV1 leads one to suspect asthma. The new algorithm6 recognizes the reduced FEV1-FVC ratio and the reversibility in FEV1 after bronchodilation and guides the clinician to differentiate asthma from COPD on the basis of historical factors as well.6 The patient in this case is a 36-year-old woman who has never been a smoker. She has numerous environmental allergies and has severe asthma that is well controlled with maintenance therapy. Cases 2 and 3 highlight the spirometric overlap between asthma and COPD and the limitations of using FEV1 reversibility to help distinguish asthma from COPD.
Case 4
The prebronchodilator and postbronchodilator FEV1-FVC ratios are 0.64 and 0.78, respectively (Figure 2 on page 1151). The prebronchodilator and postbronchodilator FEV1 values are 2.17 and 2.74 L, respectively (increase of 570 mL and 26%). The CD-ROM algorithm guides the clinician to consider a pure obstruction based on the reduced prebronchodilator FEV1-FVC ratio and the normal prebronchodilator FVC value. The increase in FEV1 meets the reversibility criterion and the clinician is led to suspect asthma. The new algorithm6 quickly excludes a spirometric diagnosis of COPD on the basis of the normal postbronchodilator FEV1-FVC ratio, and the increase in FEV1 would be consistent with a spirometric diagnosis of asthma. This case underscores the importance of using the postbronchodilator FEV1-FVC ratio to quickly exclude COPD. The patient in this case is a 19-year-old man with a history of childhood asthma and β2-agonist use increasing over several months. The algorithm in question lacks a logic string linked to the postbronchodilator FEV1-FVC ratio, making it impossible to confirm a spirometric diagnosis of COPD on the basis of current guidelines.3 The focus on changes in FEV1 after bronchodilator challenge to separate asthma from COPD could result in disease misclassification given the substantial phenotypic overlap between these 2 diseases. Further, the exclusion of bronchodilator challenge in patients with a normal FEV1-FVC ratio in the algorithm in question could translate into a missed opportunity for asthma diagnosis and to undertreatment. The limitations outlined above are addressed in a new algorithm described in an accompanying paper (page 1148).6
Acknowledgments
We thank Deborah D’Urzo, Devra D’Urzo, and Vasant Solanki for their valuable assistance in preparing this manuscript.
Notes
BOTTOM LINE
-
The interactive CD-ROM spirometry interpretation algorithm does not facilitate spirometric diagnosis of chronic obstructive pulmonary disease as outlined in current guidelines because it lacks a logic string linked to the postbronchodilator ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC).
-
Reversibility in the interactive CD-ROM relates only to changes in FEV1 and not to the FEV1–forced vital capacity ratio.
-
Reliance on changes in FEV1 after bronchodilation to separate asthma from chronic obstructive pulmonary disease can result in disease misclassification.
POINTS SAILLANTS
-
L’algorithme d’interprétation de la spirométrie sur CD-ROM interactif ne facilite pas le diagnostic de la maladie pulmonaire obstructive chronique tel qu’il est expliqué dans les guides de pratique actuels, parce qu’il y manque une chaîne logique reliée au volume expiratoire maximal par seconde (VEMS) par rapport à la capacité vitale forcée (CVF) après usage d’un bronchodilatateur.
-
La réversibilité dans le CD-ROM interactif concerne seulement les changements dans le VEMS et non au ratio VEMS par rapport à la capacité vitale forcée.
-
Se fier aux changements dans le VEMS après bronchodilatation pour distinguer l’asthme de la maladie pulmonaire obstructive chronique peut entraîner des erreurs de classification de la maladie.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}