


Abstract
Objective To identify the predictors of residential fire deaths in the Ontario pediatric population using systematically collected data from the Office of the Chief Coroner.
Design Retrospective cohort study.
Setting Ontario.
Participants Children younger than 16 years of age who died in accidental residential fires in Ontario between January 1, 2001, and December 31, 2006.
Main outcome measures The study retrospectively reviewed the coroner’s case files for 60 subjects who qualified according to the selection criteria. Reviewed documents included the coroner’s investigation statements, autopsy reports, toxicology reports, fire marshal’s reports, police reports, and Children’s Aid Society (CAS) reports. Information on a range of demographic, behavioural, social, and environmental factors was collected. Statistical tests, including relative risk, relative risk confidence intervals, and χ2 tests were performed to determine the correlation between factors of interest and to establish their significance.
Results Thirty-nine fire events resulting in 60 deaths occurred between 2001 and 2006. Fire play and electrical failures were the top 2 causes of residential fires. More fires occurred during the night (midnight to 9 am) than during the day (9 am to midnight). Nighttime fires were most commonly due to electrical failures or unattended candles, whereas daytime fires were primarily caused by unsupervised fire play and stove fires. Smoke alarms were present at 32 of 39 fire events (82%), but overall alarm functionality was only 54%. Children from families with a history of CAS involvement were approximately 32 times more likely to die in fires.
Conclusion Risk factors for pediatric fire death in Ontario include smoke alarm functionality, fire play, fire escape behaviour, and CAS involvement. Efforts to prevent residential fire deaths should target these populations and risk factors, and primary care physicians should consider education around these issues as a primary preventive strategy for families with young children.
Residential fire is a leading cause of unintentional death for young children at home and the fifth leading cause of unintentional injury-related death overall.1–3 In the United States, approximately 2500 children die as a result of residential fires and burns each year, while another 10 000 suffer permanent disability.3 Factors that increase a child’s risk of fire-related injury and death have been shown to include a range of environmental, behavioural, and social conditions. Studies in the United States and United Kingdom have identified maternal education, socioeconomic status, being from a single-parent household, housing regulations, lack of fire escape plans, smoke alarm functionality, and adequate adult supervision as important risk determinants.1,2,4–6
Despite the availability of US and UK data,1–5,7–10 few, if any, studies have established these associations in the population of Ontario. The identification of such risk factors is key to implementing effective and efficient provincial fire-prevention programs. Conclusions drawn from collected data can be used to evaluate current fire-prevention strategies and to make recommendations for future programs, including the consideration of a primary care physician’s role in identifying at-risk patients for fire safety education.
METHODS
Ethics approval for the study was obtained from the University of Toronto Ethics Review Board.
The study retrospectively reviewed all accidental residential fire deaths involving children younger than 16 years of age that occurred in Ontario between January 1, 2001, and December 31, 2006. Complete coroner’s files of 60 cases satisfying the inclusion criteria were obtained from the Ontario Office of the Chief Coroner (OCC) database, which indexes investigative findings from all nonnatural deaths, including fire deaths, in Ontario. Fire was determined to be the cause of death for all 60 children based on autopsy results, using established methods of tissue examination and biochemical analysis carried out by licensed pathologists. Reviewed documents within each file included the coroner’s investigation statement, the pathologist’s autopsy report, the toxicology report, the fire marshal’s report, the police report, and the Children’s Aid Society (CAS) report.
Information on a range of demographic, behavioural, social, and environmental factors was collected from the case files, including age, sex, date of death, geographic region of death, location of death, time of death, cause of death, smoke alarm status, cause of fire, and status of CAS involvement. A total of 53 complete case files were available for review. The 7 incomplete files contained cases of deaths from a single fire incident, for which no official inquest into the cause of the fire was made by the fire marshal (likely owing to family objection). Although the fire marshal’s report was missing from these files, the 911 report and various media reports were available for review, which provided information on the timing of the fire. Because this particular fire occurred in the middle of the night while the children were sleeping, the location of the fatalities was deemed to be the bedroom. The cause of the fire was coded as undetermined.
Collected data were entered into Microsoft Excel 2007 and tabulated. Calculations of relative risk (RR), RR confidence intervals, and χ2 statistics were performed to determine the associations between 2 or more identified factors.
Children’s Aid Society statistics
To calculate the RR of fire death in children with CAS involvement compared with those with no CAS involvement, the following equation was used:
-
investigations and assessments—investigations of reports that children are or might be in need of protection,
-
protection—active protection cases, and
-
children in care—children who are in the temporary (court-ordered or through voluntary agreements) or permanent care of a CAS.
As of March 31, 2009, there were 12 268 open investigations, 25 713 open protection cases, and 18 377 children in care, for a total of 56 358 children involved with CAS (written communication, Ontario Association of Children’s Aid Societies, April 2009). Representatives from within the Ontario Association of Children’s Aid Societies were unable to provide statistics from previous years; however, year-to-year fluctuations are believed to be negligible when used in the calculation.
Of note, both open investigations and open protection cases are counted per family, not per child. Many children in care also have open family cases under investigation or protection and will be counted more than once in the summation. This is balanced by the fact that some families under investigation or protection will have more than 1 child. Overall, by including the number of open investigation cases, we are providing an overestimation of the number of children involved with CAS, which translates to a more conservative calculation of RR.
The total number of children not involved with CAS in Ontario per year is the difference between the total number of children in Ontario in 2006 (3 977 005 according to the 2006 Statistics Canada census report12) and the total number of children involved with CAS.
RESULTS
Demographics
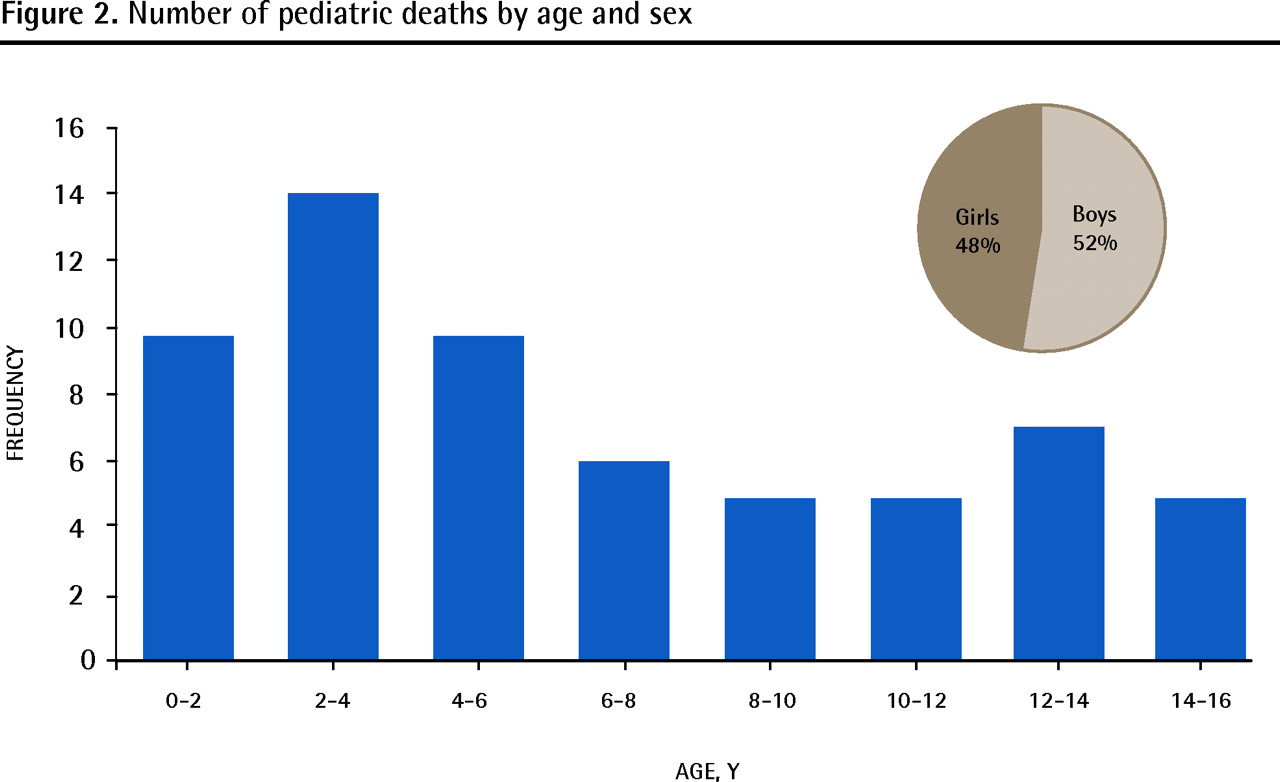
Thirty-nine fire events resulting in 60 deaths occurred in Ontario between 2001 and 2006 (for an average of 6.5 fatal fire events per year, 10 deaths per year, and 2.5 deaths per 1 000 000 children per year), with a general decline in fire incidents and deaths from 2001 to 2006 (Figure 1). The highest incidence of fire deaths occurred in those younger than 6 years of age, peaking in the 2-to 4-year-old age group (Figure 2). Slightly more boys than girls (52% vs 48%) died in house fires in the 6-year period.

Number of fatal pediatric fire incidents and number of pediatric fire deaths from 2001 to 2006
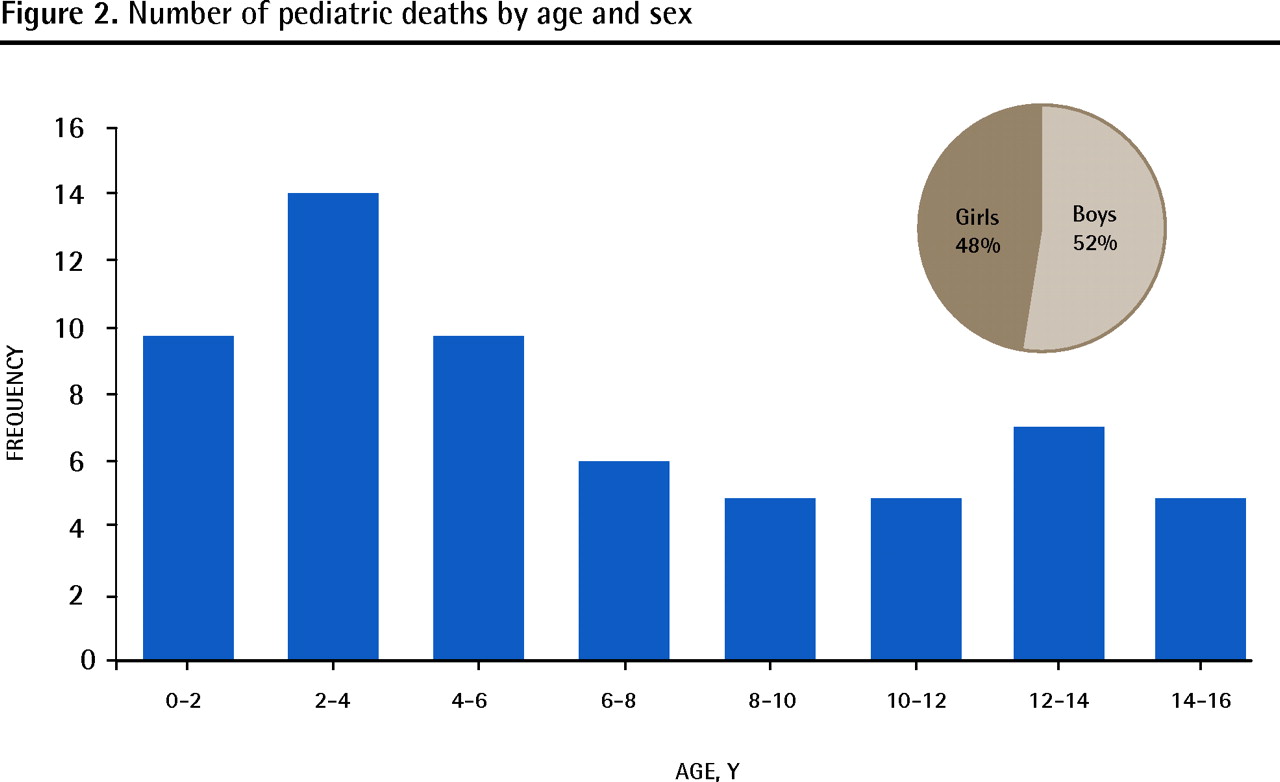
Number of pediatric deaths by age and sex
Timing of fire
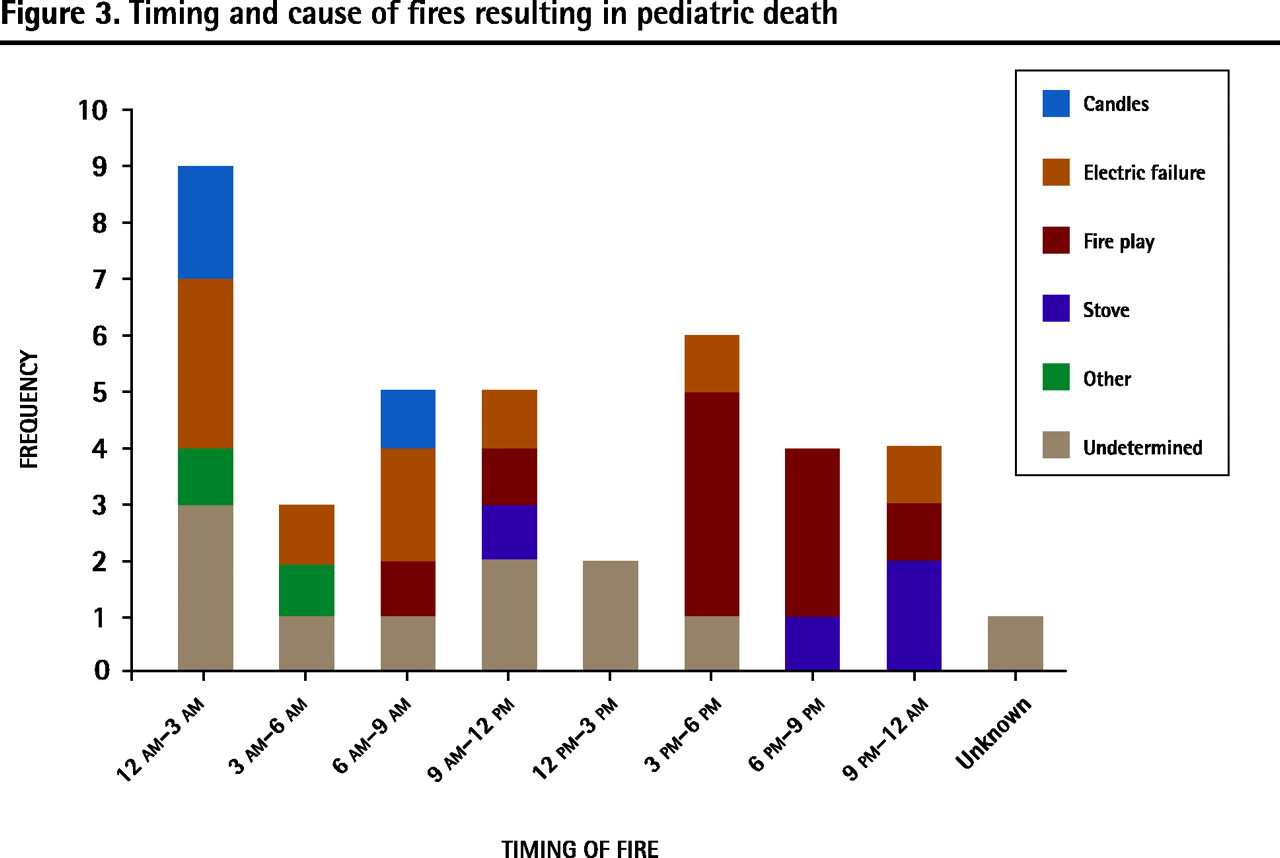
More fires occurred during sleeping hours (midnight to 9 am) than during the daytime (9 am to midnight). Nighttime fires were likely due to electrical failure or unattended candles, whereas daytime fires, particularly from noon to 6 pm, were mostly caused by fire play or stove fires (Figure 3).
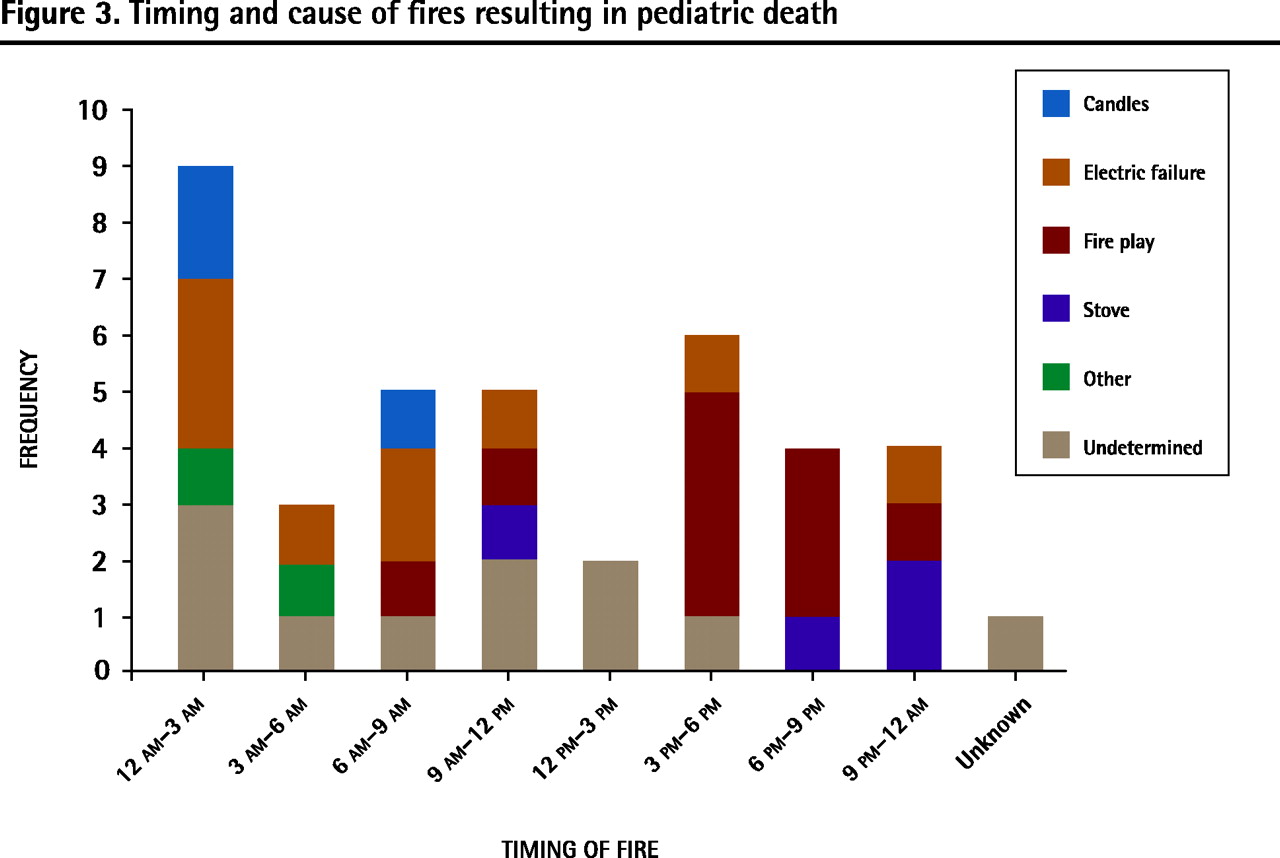
Timing and cause of fires resulting in pediatric death
Place of fire origin
As shown in Figure 4, most fires started in the living room (41%), followed by the bedroom (26%), kitchen (10%), and basement (8%).

Location of the start of fires resulting in pediatric death
Location of fatality
Figure 5 outlines the locations of fatalities. Most (62%) children died in their bedrooms, with the remainder dying in the living room (12%), basement (8%), hallway (7%), bathroom (3%), or other areas (3%).

Location of fatalities occurring as a result of fires
Cause of fire
Fire play (26%) and electrical failure (20%) were the top 2 causes of fire in our population (Figure 6), followed by unattended candles (15%), stove fires (5%), and cigarette fires (3%). A cause was not identified in 28% of fires. Fire play, most often involving lighters or matches, led to 10 fires and 12 deaths. All fires in this group took place during waking hours (11 am to 11 pm) and occurred in the absence of adult supervision. Children who died as a result of fire play were associated with a personal or sibling history of fire play (4 deaths), having smokers in the house (3 deaths), and CAS involvement (7 deaths). Ten of the 12 children were younger than 6 years of age. Electrical failure was the cause of 8 fire incidents and 15 deaths, with cord overheating and heater malfunctions being the most common causes. All electrical failure events occurred during the night or when the victims were asleep.

Causes of fires resulting in pediatric death
Smoke alarm status
Smoke alarms were found at the scene of 32 out of 39 (82%) fire incidents in our study population. Alarms were either absent or not working in 46% of fire incidents. Alarm functionality was not associated with the timing of fires (ie, sleeping hours [midnight to 9 am] vs daytime [9 am to midnight]; P = .49 by χ2 test).
Involvement by CAS
Nineteen out of 60 children (32%) came from families with a history of CAS involvement. These children were more than 30 times as likely to die in fires as those who were not involved with the CAS (RR = 32, 95% confidence interval 18.7 to 55.5; P < .0001).
No association was found between CAS involvement and smoke alarm function (P = .50). All CAS internal investigations concluded that the agency’s involvement did not contribute to any of the reviewed fire deaths, nor could it have prevented any death operating under the CAS’s current mandate.
DISCUSSION
Factors predisposing children in Ontario to fire-related deaths were examined in this study. Environmental factors that predisposed children to fire deaths in our sample included smoke alarm functionality and electrical safety, while behavioural factors included a child’s fire-play history, his or her behavioural response to fire, and the absence of rehearsed fire escape plans. A history of CAS involvement was the main social factor, associated with a 32-fold increased risk of fire fatality.
The sex difference and peak age range in fire deaths in our population are consistent with numbers from the US National Center for Child Death Review, which reports that boys aged 0 to 4 are at the greatest risk of fire-related injuries and death.14 Younger children are more at risk of residential fire deaths and injuries owing to their limited ability to react promptly and rationally to fires.2 The 1998 public health reports found that fire escape planning was uncommon across all age groups, with less than 20% of households reporting that they had practised fire escape plans with family members.15 In our population, the children’s unfamiliarity with fire escape plans, in addition to their fire-response behaviour, severely reduced their likelihood of escape.
Despite increasingly stringent smoke alarm legislation,16 almost half of the sites of fires leading to death in our study population did not have functioning smoke alarms. Smoke alarm functionality remains a common problem in other parts of the industrialized world, with US and UK studies reporting functionality in less than 20% of installed alarms.8,17 A statistical association between CAS involvement and smoke alarm functionality was not found in our population. However, CAS involvement is only one of many indicators of a potentially unstable family environment; some children in our study lived in substandard conditions with nonfunctional smoke alarms but were not involved with the CAS.
Fire play was shown to be the number one cause of fire death in our population, consistent with results from previous studies.18–20 More than 80% of children in our study who died because of fire play were in the preschool age group. This corroborates data from the US National Fire Protection Association, which reports that more than half of children who play with fire are between the ages of 4 and 9 years.19 Young children have limited understanding of the consequence of playing with fire and do not comprehend the potential of a small candle flame for destruction.21 Although older children might have more insight, they often overestimate their ability to control fires.21 Furthermore, caregivers’ actions toward fire are crucial in influencing a child’s fire behaviour. Caregivers who light their cigarettes in front of their children and carelessly place lighters and matches in easily accessible places can inadvertently normalize children’s attitudes toward fire.21
The second most common cause of fire deaths in our study population was electrical failure. The US National Fire Protection Association reports 485 deaths per year caused by electrical failure, with most such fires caused by misuse and poor maintenance of electrical appliances, old wiring, running cords under rugs, and overloaded circuits and extensions.19 Electrical fires are more common during the winter, when children are more likely to be indoors and the use of electrical heating equipment is prevalent.19
The high rate of CAS involvement in our study population was expected, and indicates that children from potentially unstable families are at much higher risk of fire deaths and, thus, in need of better fire protection, prevention, and education. Children from poor and unstable families have multiple risk factors for fire mortality: they are more likely to reside in dwellings with small or no windows and in poorly maintained houses with unsafe wiring and nonfunctional smoke alarms5; they have less supervision; and they are more likely to be exposed to smokers in the house and to display fire-play behaviour.6,21 In our data set, 7 of 12 children who died as a result of fire play had a family history of CAS involvement. This is consistent with findings from the 2002 Portland Report, which showed that 80% of children with fire-setting behaviour lived in divided families, with 54% of the families earning less than $30 000 (US) annually.22 Furthermore, evidence suggests that caregivers in low-income families are more likely to disable working alarms owing to annoyance with false alarms from cooking or cigarette smoke in overcrowded living spaces.17 The prevalence of CAS involvement in our population suggests that there could be a role for the CAS in lowering the high incidence of fire fatalities in at-risk children. For example, it might be advisable for CAS and other support staff who make regular home visits to review the presence, location, and functionality of smoke alarms. Any noncompliance should be reported to the fire marshal for further investigation and education.
Limitations
Several limitations exist with our data collection and analyses. First, in severe fires where residual evidence was poor, factors of interest to the study, including the cause of fire, the location of death, and the smoke alarm status, could not be determined. Second, although data on individual victims were systematically collected by trained authorities, they were collected for other purposes in the death investigation process and might not include all possible factors predisposing children to fire deaths in this population. Without a negative control group, the study cannot provide quantitative evidence to definitively conclude that the identified environmental and behavioural factors are correlated with the risk of fire death. Third, CAS involvement was used in this study as an indicator of socioeconomic status and household stability. While such correlations have been proven, it would be ideal if more comprehensive sociodemographic information, such as household income, parental education level, and housing type, were available for analysis. Fourth, census information used to calculate the RR of fire death in children with CAS involvement was not available in all the years included in the study. Although year-to-year fluctuations in the population are proportionately small, the accuracy of certain RR calculations might be compromised. Finally, the relatively small population size of 60 limits the power of the statistical findings and the external validity of the study results.
Conclusion
Interventions are most effective when directed at the groups at the highest risk. Efforts in the past decade by district school boards, working with local fire-protection agencies, have reduced fire deaths, but these efforts might now require additional, more focused strategies to ensure effectiveness in high-risk groups. Primary care physicians should be cognizant of their role in the education of young families with children regarding fire safety. At a minimum, assessment of home fire safety using screening questions could be implemented during parent or child periodic health examinations. Physicians should also educate smoking parents to keep their matches and lighters out of their children’s reach, as well as encourage them to stop smoking altogether. Inquiry into children with fire-setting or fire-play behaviour should be made, with subsequent referral to appropriate fire-education counselors or psychiatrists. Finally, physicians need to recognize that families with child welfare involvement might require considerable education about fire safety. Family physicians in trusting and supportive therapeutic relationships with children and their families are the most fitting educators in this regard. Residential fire death has become a highly preventable cause of mortality. We hope that physicians will use the results of the study to identify at-risk children in their practices and subsequently direct those children and their families to appropriate community resources to receive focused fire-prevention education and programs.
Notes
EDITOR’S KEY POINTS
-
This study aimed to identify predictors of residential fire deaths in the Ontario pediatric population. The authors found that risk factors included smoke alarm functionality, fire play, and fire escape behaviour. Notably, children from families with a history of Children’s Aid Society (CAS) involvement were 32 times more likely to die in fires than children with no CAS involvement were.
-
Interventions are most effective when directed at groups with the highest risk. Primary care physicians can help educate families about fire safety, including assessing home fire safety using screening questions during parent or child periodic health examinations. Physicians should also educate smokers to keep matches and lighters out of children’s reach, as well as encourage them to stop smoking altogether. Inquiry into fire-setting or fire-play behaviour should also be made, with subsequent referral to appropriate fire-education counselors or psychiatrists.
-
Families with CAS involvement in particular might require considerable education around fire safety. Family physicians in trusting and supportive therapeutic relationships with children and their families are the most fitting educators in this regard.
POINTS DE REPÈRE DU RÉDACTEUR
-
Cette étude voulait identifier les facteurs permettant de prévoir les décès résultant d’incendies résidentiels parmi la population pédiatrique de l’Ontario. Parmi les facteurs de risque identifiés, mentionnons l’état des détecteurs de fumée, le fait de jouer avec le feu et le comportement par rapport aux issues de secours. Fait significatif, les enfants de familles qui ont déjà eu affaire à la Société d’aide à l’enfance (SAE) étaient 32 fois plus susceptibles de mourir dans des incendies que ceux qui n’avaient pas eu affaire à la SAE.
-
Les interventions les plus efficaces étaient celles qui s’adressaient aux groupes les plus à risque. Les médecins de première ligne peuvent aider à éduquer les familles sur la prévention des incendies, incluant une évaluation des mesures de sécurité contre le feu à l’aide d’un questionnaire de dépistage à l’occasion de l’examen périodique de santé des enfants ou des parents. Le médecin pourrait aussi conseiller aux fumeurs de garder les allumettes et briquets hors de portée des enfants, en plus de les inciter à cesser carrément de fumer. On devrait aussi s’informer des comportements consistant à jouer avec le feu ou à mettre le feu, pour les diriger vers des conseillers spécialisés ou des psychiatres.
-
Les familles ayant eu affaire à la SAE pourraient nécessiter beaucoup de formation sur la prévention des incendies. Le médecin de famille qui maintient une bonne relation de confiance et un bon support thérapeutique avec les enfants et leurs familles est le mieux placé pour jouer ce rôle.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Contributors
Miss Chen completed the data collection, data analyses, and preparation of the draft manuscript. Ms Bridgman-Acker, Dr Edwards, and Dr Lauwers were supervisors for the study and contributed substantially to the concept and design of the study, made substantial revisions to the draft, and approved the submitted version to be published.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}