


Abstract
Objective To document the perceptions that family medicine residents have of patient management.
Design Bilingual, quantitative questionnaire consisting of 10 questions.
Setting Quebec.
Participants All (n = 747) family medicine residents in Quebec.
Main outcome measures The questionnaire was designed to capture residents’ perceptions of patient management, their plans to incorporate patient management into their practice, and how they thought this aspect of family medicine practice should be promoted.
Results In all, 289 residents (38.7%) completed the questionnaire. Of these, 201 reported that they planned to accept patients during their first 5 years of practice. The most common inhibiting factors were the difficulty of taking time off, complex cases, and the responsibilities that come with continuity of care. Neither Quebec’s regional medical staffing plans nor its specific medical activities emerged as important inhibiting factors. Respondents indicated that raising the profile of family medicine could be achieved by promoting it to medical students, changing the institutional culture, and increasing the visibility of family medicine residents and supervisors on the teams working in training settings.
Conclusion Quebec residents plan to include patient management in their practices. However, solutions must be found for the heavy burden of responsibility that comes with an office practice and for continuing to make patient management appealing to young family physicians.
The cornerstone of family medicine is patient management. And yet, in spite of the efforts that have been made to make the inclusion of patient management in one’s medical practice attractive, it is a different story in the field. In a study of physicians in general practice conducted by the Fédération des médecins omnipraticiens du Québec in 2006 and 2007,1 64% of young physicians had chosen to work primarily in secondary care settings. In addition, although 60% of family physicians practised primary care, more than 64% had been in practice for longer than 20 years, compared with 14% who had practised for less than 10 years.1 Data collected in 2010 show that family physicians with 15 years of practice or less work in hospitals 70% of the time.2 The shortage of Quebec physicians delivering patient management is alarming: 1 in 5 Quebec residents does not have a family physician.3 Secondary medical care is just as important to the proper functioning of Quebec’s health care system as primary care is. Reconciling these 2 aspects of the system, which are so closely linked when family medicine is promoted, is essential to the survival of this specialty, which affects both the delivery of patient care in the physician’s office and the practice of general medicine in a hospital setting.
Because most young physicians decide during their residency whether they will provide patient management, we believe that it is important to know what students currently doing their residency plan to practise, and to ask them how patient management could be portrayed as a stimulating and enriching way to practise family medicine. We also believe that it is important to highlight factors that, according to residents, could help to promote family medicine, with patient management as a central focus. To begin evaluating these complex, yet important, aspects, we asked the 2011 and 2012 cohorts of family medicine residents about their plans regarding patient management and their perceptions of the value placed on family medicine.
METHODS
A bilingual questionnaire consisting of 10 questions was created by the author (M.R.B.L.) in SurveyMonkey and edited by the resident coordinators and directors in the various training settings of each of Quebec’s 4 faculties of medicine. The questionnaire was distributed to all of the family medicine residents in Quebec in the spring of 2011; ie, a total of 747 residents. The quantitative format of the questionnaire meant that it could be completed in less than 10 minutes and respondents’ comments could also be solicited. The questionnaire was initially sent to the first- and second-year residents at one faculty of medicine; a few weeks later, it was sent to those at the other 3 faculties of medicine in Quebec. The residents were given 1 week to complete the survey.
We used a quantitative approach to enable respondents to express their opinions and to make the data easier to analyze. A comments section was included with the questions to support the quantitative results and to make it possible to determine whether we had inadvertently excluded important issues when developing the survey. We analyzed the results using the SurveyMonkey database. The questionnaire results were combined in an Excel table and checked by the author (M.R.B.L.) and another person (Dr Olivier Drouin). We analyzed the comments by looking for recurring terms, then corroborating these results and the quantitative results. Qualitative analysis was limited, given the format of the questionnaire. The comments were only used to inform the results. However, our conclusions are based on both the comments and the results when they coincided.
RESULTS
Patient management
In all, 289 residents completed the survey, yielding a response rate of 38.7%. Figure 1 shows the response rate for each of Quebec’s 4 faculties of medicine. Of 284 respondents, 201 (70.8%) indicated that they planned to accept patients in their first 5 years of practice, and 73.4% planned to accept patients in their first year of practice. For most, patient management would constitute one aspect of a mixed practice: 19.8% thought that patient management would represent slightly less than a quarter of their practice; 31.5% said between a quarter and less than half of their practice; and 24.1% said between half and three-quarters of their practice. Overall, 88.9% planned to accept patients in Quebec. Only 18.9% did not plan to practise patient management (Figure 2).

Response rate in Quebec’s 4 faculties of medicine
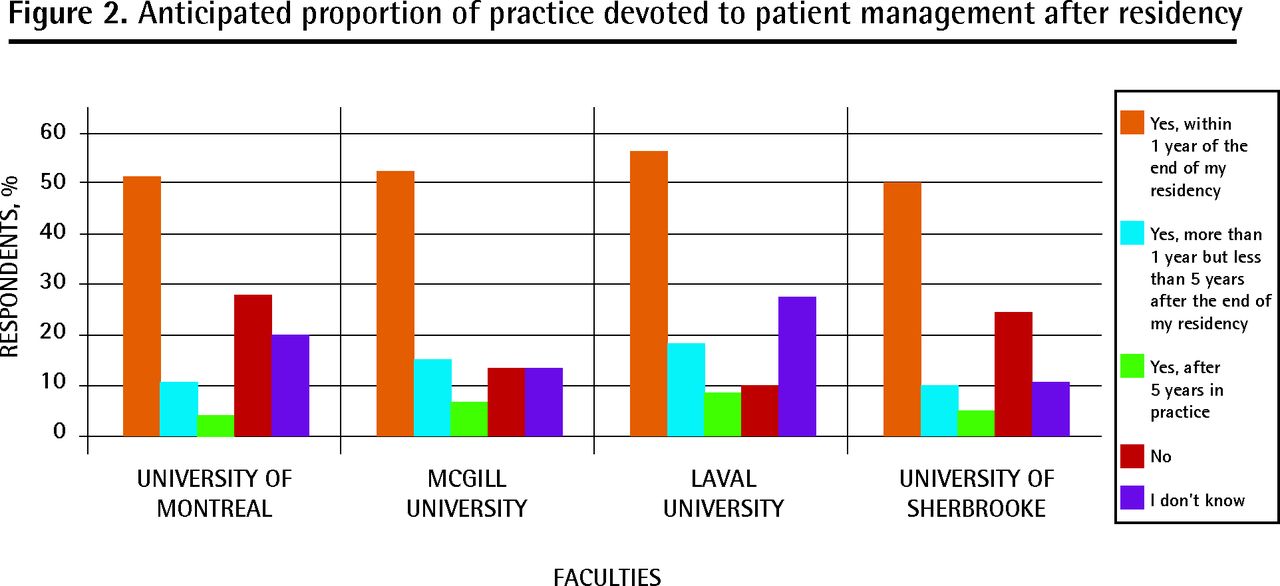
Anticipated proportion of practice devoted to patient management after residency
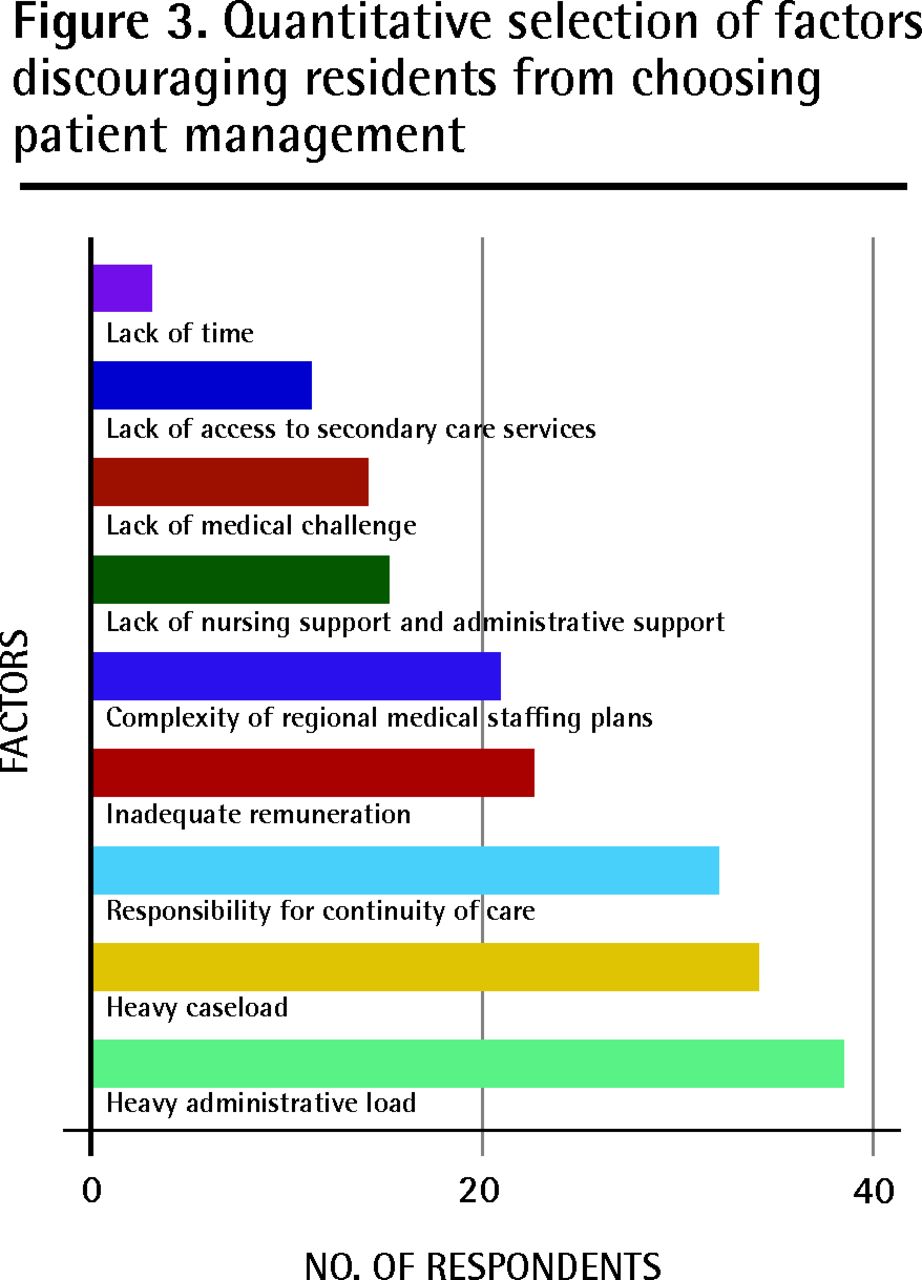
Patient acknowledgment, a diverse practice mix, and flexible scheduling were the most common reasons cited for practising patient management. Among respondents who did not plan to practise patient management, the most common reasons cited were the burdens related to patient management, the administrative demands, and the responsibility of providing continuity of care. Figure 3 shows the importance the respondents ascribed to these reasons.

Quantitative selection of factors discouraging residents from choosing patient management
When all of the residents were asked open-ended questions, their comments reflected the same concerns. Reasons for trepidation included the difficulty of taking time off or moving, the complexity of some patients’ cases, and the responsibilities that come with continuity of care. One resident referred to “increasing patient demands and requirements,” a sentiment expressed by many residents. Although less common, a number of other factors that cause resident physicians to feel trepidation about office practices came up several times in the residents’ comments: the lack of professional support staff such as nurses and physiotherapists, the administrative work involved, and the difficulty of obtaining the services of, and communicating with, specialists.
Quebec’s regional medical staffing plans (plans régionaux d’effectifs médicaux) dictate a limited number of positions in family medicine for each of the province’s regions. Newly certified family physicians must obtain plans through a region’s health and social services agency to set up practices in the region; this limits their choice of regions. Because of this, it was surprising to note that only 19 respondents who did not plan to include patient management in their practice believed that the regional medical staffing plans were an inhibiting factor, and only 2 respondents actually referred to the plans or to Quebec’s specific medical activities (activités médicales particulières) in their comments. Specific medical activities are, for the most part, performed in health institutions (emergency medicine, obstetrics and gynecology, hospitalization of patients) and were created to address needs identified as priorities by the Quebec government. Family physicians are required to perform a certain number of specific medical activity hours per week, based on their years of practice. Physicians who fail to perform their specific medical activities are penalized financially.
Promoting family medicine
Overall, 67.7% of respondents believe that family medicine is not perceived as a speciality and needs to be more positively promoted (Figure 4). When surveyed quantitatively, the respondents offered the following suggestions to promote family medicine most often: promoting family medicine more effectively to medical students, changing the institutional culture around family medicine, and raising the profile of resident physicians and family medicine supervisors on the care teams in training settings (Figure 5).

Respondents’ opinions of the perception of family medicine as a speciality
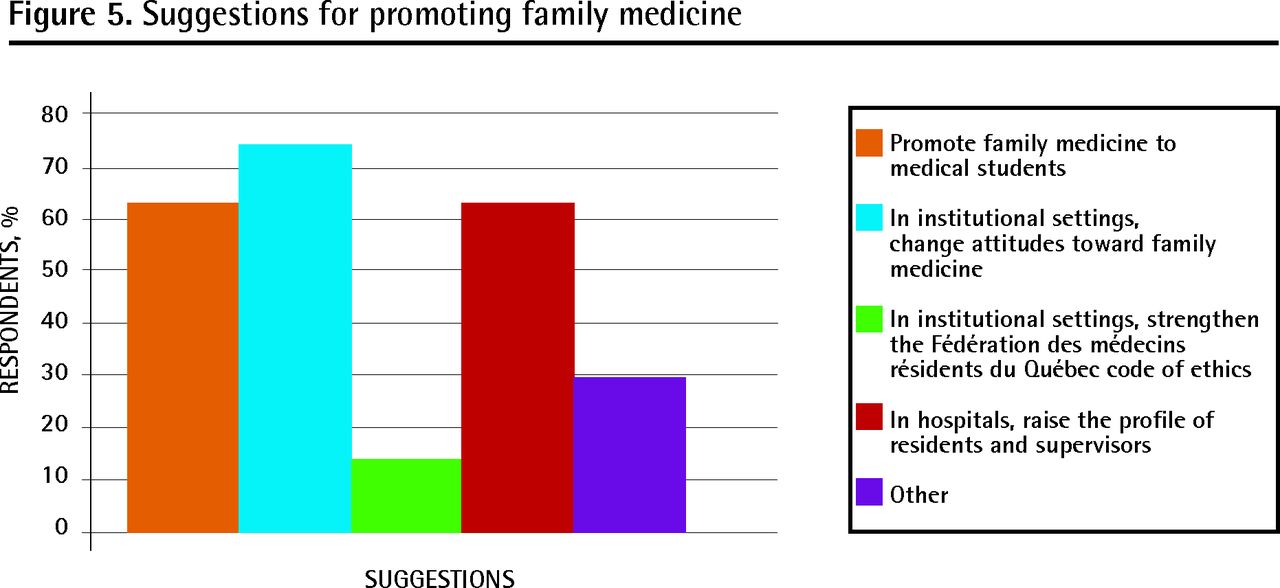
Suggestions for promoting family medicine
In their comments, the resident physicians stated that it was important to increase family physician involvement within faculties of medicine, to make specialists aware of the importance of family physicians, and to offer family physicians adequate remuneration.
DISCUSSION
To date, this is the largest study of its kind to document Quebec resident physicians’ perceptions of patient management. This study calls into question a number of assumptions that are made by the press and in our faculties of medicine. First, a large proportion of resident physicians do plan to include patient management in their medical practice and overwhelmingly, most do plan to stay in the province in which they trained (ie, Quebec). Most plan to make patient management part of a mixed practice; this was also a finding in a study of Quebec resident physicians published in 2008.4 As mentioned above, resident physicians have trepidations; they prefer to introduce patient management gradually over the first 5 years of their practice. In training settings in Quebec, the requirement that physicians perform 15 hours of specific medical activities and the limits imposed on medical practice by the regional medical staffing plans are frequently cited as irritants.2,5 Yet, they did not emerge clearly as such in the context of this study.
The 3 main solutions offered by respondents are the following: 1) recognition from colleagues in other specialties both during residency and later, during medical practice; 2) greater involvement of family physicians in academic roles and activities at the predoctoral and postdoctoral levels, as a means of promoting family medicine to medical students; and 3) adequate remuneration.
Limitations
The number of physician residents who completed the questionnaire is limited. This might reflect a bias, if we assume that the residents who responded are those most interested in the subject or those with the strongest opinions. Certain faculties and questions had higher response rates than others. Although developed quantitatively, the format of the survey might have steered respondents toward a positive or negative perception. We wanted to keep the questionnaire short; however, this might have limited in-depth exploration of an issue (eg, what residents mean when they say that the perception of family medicine as a specialty is negative). Perceptions were documented at a specific time and might have changed substantially in the months or years afterward. We surveyed a specific cohort and it is difficult to infer that previous or subsequent cohorts think the same way. It is also difficult to determine the extent to which the residents’ experiences of patient management—whether positive or negative—correlate with their experience of continuity of care once they are in practice and, above all, whether this colours their current perception of patient management. In terms of inhibiting factors, it is difficult to know which are attributable to the organization of care and which are attributable to teaching in the family medicine units.
Implications
In spite of these limitations, the data do make it possible to identify both factors that are detracting from the appeal of patient management and solutions to address them (Table 1). For example, the burdens associated with medical practice and complex cases that were raised frequently by the respondents could be addressed through various practice configurations, such as family medicine groups. Similarly, exposure to patient management during training should reflect what students will encounter in their practice, particularly where complex cases are concerned. Two plausible solutions are ensuring that residents do not take on a disproportionate number of complex cases and ensuring that the expectations around their involvement with patients reflect the reality of physicians in practice. The creation of multidisciplinary teams is another solution to the challenge of complex cases. Family medicine groups that consist of family physicians and other health professionals such as nurses and psychologists ensure that an entire group of professionals provides continuity of care, instead of a physician practising alone. These groups are partially funded by the government. In the United States, patient-centred medical homes follow a team-based continuity-of-care delivery model, with a physician as team leader. The same is true for Quebec’s local community service centres both in practice settings and teaching settings. A viable primary care system must include administrative staff and other health professionals, as well as adequate information technology services. Communication with and access to specialists are 2 very important points for further exploration.
Factors discouraging residents from incorporating patient management into their practices and possible solutions
Promoting family medicine is an important factor both for recruitment and for changing the way in which society as a whole perceives family medicine. To achieve this, we must continue to raise the profile of family physicians during training and when they are in practice. Administering a second survey to these respondents once they have begun their practices would make it possible to identify the factors that shaped their practices.
Once again, patient management is the cornerstone of family medicine. Placing greater importance and emphasis on the myriad aspects of family medicine practice will, in turn, promote the importance and value of patient management. In a parallel fashion, if we identify the obstacles to patient management and prepare residents adequately, they might be more inclined to make patient management the focus of their practices, adding further value to family medicine.
Conclusion
Most of the family medicine residents who are in training in Quebec and who responded to our survey plan to practise patient management in the first 5 years of their practice. Their reservations about doing so relate to the current structure of the system, both clinically and academically, and to the implications of providing continuity of care. In this study, the government policies that are currently in effect did not emerge as important factors. Respondents were primarily concerned with easing the load of patient management. Plausible solutions have begun to be implemented: group clinics in which the caseload is shared, adequate administrative support, and increased support from other health care professionals. Solutions to use during residency remain to be explored.
According to the respondents in this study, general acceptance and acknowledgment of the importance of family medicine depends upon the following: 1) recognition and acknowledgment from colleagues in other specialties; 2) getting family physicians more deeply involved in academic activities at the predoctoral and postdoctoral level, so that family medicine can be promoted to medical students; and 3) adequate remuneration. This is ambitious, yet completely realistic!
Acknowledgments
The authors acknowledge the contribution of Olivier Drouin MD CM MSc, who helped to analyze the data.
Notes
EDITOR’S KEY POINTS
-
The most common reasons cited for including patient management in one’s medical practice are patient acknowledgment and gratitude, patient mix, and flexible hours.
-
The main perceived drawbacks to patient management are the difficulty of leaving one’s practice for a break or to move, the complexity of the cases, and the responsibilities involved in providing continuity of care. The main perceived drawbacks to an office practice are the lack of professional support staff, the burden of administrative tasks, the difficulty of obtaining specialist services, and the difficulty communicating with specialists.
-
Close to 70% of respondents believe that family medicine is not seen as a specialty and that it needs to be promoted more positively.
Footnotes
-
This article has been peer reviewed.
-
Contributors
Dr B-Lajoie developed the research protocol, processed and analyzed the data, and wrote this article. Ms Carrier helped to collect the data and write the article.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}