


Abstract
Objective To explore the reasons why long-term weight loss is seldom achieved and to evaluate the consequences of various weight trajectories, including stability, loss, and gain.
Quality of evidence Studies evaluating population weight metrics were mainly observational. Level I evidence was available to evaluate the influence of weight interventions on mortality and quality of life.
Main message Sustained weight loss is achieved by a small percentage of those intending to lose weight. Mortality is lowest in the high-normal and overweight range. The safest body-size trajectory is stable weight with optimization of physical and metabolic fitness. With weight loss there is evidence for lower mortality in those with obesity-related comorbidities. There is also evidence for improved health-related quality of life in obese individuals who lose weight. Weight loss in the healthy obese, however, is associated with increased mortality.
Conclusion Weight loss is advisable only for those with obesity-related comorbidities. Healthy obese people wishing to lose weight should be informed that there might be associated risks. A strategy that leads to a stable body mass index with optimized physical and metabolic fitness at any size is the safest weight intervention option.
Statistics show that of those who contract the habit of eating, very few survive.
George Bernard Shaw
The genesis of humankind from primates in sub-Saharan Africa, along with the evolution of human form and function, was influenced greatly by the availability of high-quality energy in the food supply. As our ancestors migrated out of Africa, they settled in fertile areas to the north where the Agricultural Revolution developed, enabling fewer people to look after the nutritional needs of many. Ensuing food security promoted rapid development of urbanization,1 knowledge, and innovation. Agriculture enabled increased consumption of carbohydrates from cereals and legumes, and saturated fats from domestic meats and dairy. Overweight and obesity were uncommon.2
In the late 18th century, continued success of the species and continued nurturing of the human brain2,3 brought about the Industrial Revolution. It became possible to easily remove fibre and germ from cereals. Refined sugars became more available; latterly, high-fructose corn syrup became a staple in the Western diet, with adverse metabolic consequences.4,5 It became possible to extract oils from seeds, leading to a relative increase in omega-6 over omega-3 fatty acids in the diet, diminishing the anti-inflammatory benefits of the latter.5,6 Hydrogenation of these oils produced novel and highly atherogenic trans isomers, which had never been found in traditional diets.7 Apart from their metabolic consequences, these manipulations have increased caloric density in our foods and greatly reduced the physical activity required to procure those foods.
It is popularly hypothesized that some of us evolved genetically to efficiently hold on to calories in times of famine (the thrifty genotype8). This might have occurred by means of a quick insulin “trigger,” which minimizes the renal wasting of glucose and encourages uptake into cells, including adipocytes, leading to hyperinsulinemia, obesity, and diabetes. This genetic subtype conferred survival advantages in times of episodic famine, but primitive genes did not have time to adapt in the context of a plentiful food supply. Those most adapted to survive intermittent famine and hardship were now at a disadvantage, and an environment of abundant processed foods and inadequate exercise has led to increased body size and chronic disease.9
Quality of evidence
A PubMed search was initially done using MeSH terms or text words including obesity or overweight and mortality and weight loss or weight trajectory, restricted to the past 10 years and to reviews or meta-analyses. Recent evidence from observational studies was preferred because of better statistical control over confounding variables. References from appropriate retrieved papers were used to obtain other interventional studies, with preference given to larger controlled prospective cohort trials or randomized controlled trials. Additional searches were carried out to clarify the effects of covariates, such as diet, exercise, and quality of life. Level I studies were preferred, but because diet and exercise interventions present difficulties with blinding and compliance, level II studies were deemed acceptable (Table 1).
Levels of evidence
Main message
Classification and prevalence of body size
The most common measure of body size is the body mass index (BMI), defined as the weight in kilograms divided by the height in metres squared. In adults, overweight is defined as a BMI in the 25- to 30-kg/m2 range. Values above 30 kg/m2 constitute obesity (Table 2).10,11 Classification in children is expressed as a BMI percentile based on the Centers for Disease Control and Prevention 2000 BMI-for-age growth charts. Values for BMI between the 85th and 95th percentiles are deemed overweight, while those above the 95th percentile are considered obese.12
Prevalence of overweight and obesity in adults
Rates of obesity and overweight are high among adults (Table 2)10,11 and children (Table 3)12 in both Canada and the United States. The rate of increase has moderated in both countries in the past several years.10–12 Educational interventions might have had some effect, but it also seems possible that our susceptible primitive gene pool is becoming saturated by the obesogenic effects of the current environment.
Prevalence of overweight and obesity in children
Body-weight trajectory
Cross-sectional analyses of healthy populations show, on average and without intervention, a gradual increase in body weight with increasing age, with a gradual slowing of this trend in the fifth to sixth decades.13 Weight-gain velocity is greatest in men younger than 40 years and in women younger than 50 years. Maximum weight is achieved on average between ages 50 and 69. Beyond age 70, some weight loss is more common.14 Averaging all age groups, BMI tends to increase by 1.5% per decade.14,15 In Canadians, this translates to between 0.25 and 0.50 kg per year,10 enough to move most individuals into a higher BMI category over a lifetime. A disproportionate amount of this weight gain is seen in the class 2 and 3 obesity categories16,17 defined in Table 2.10,11
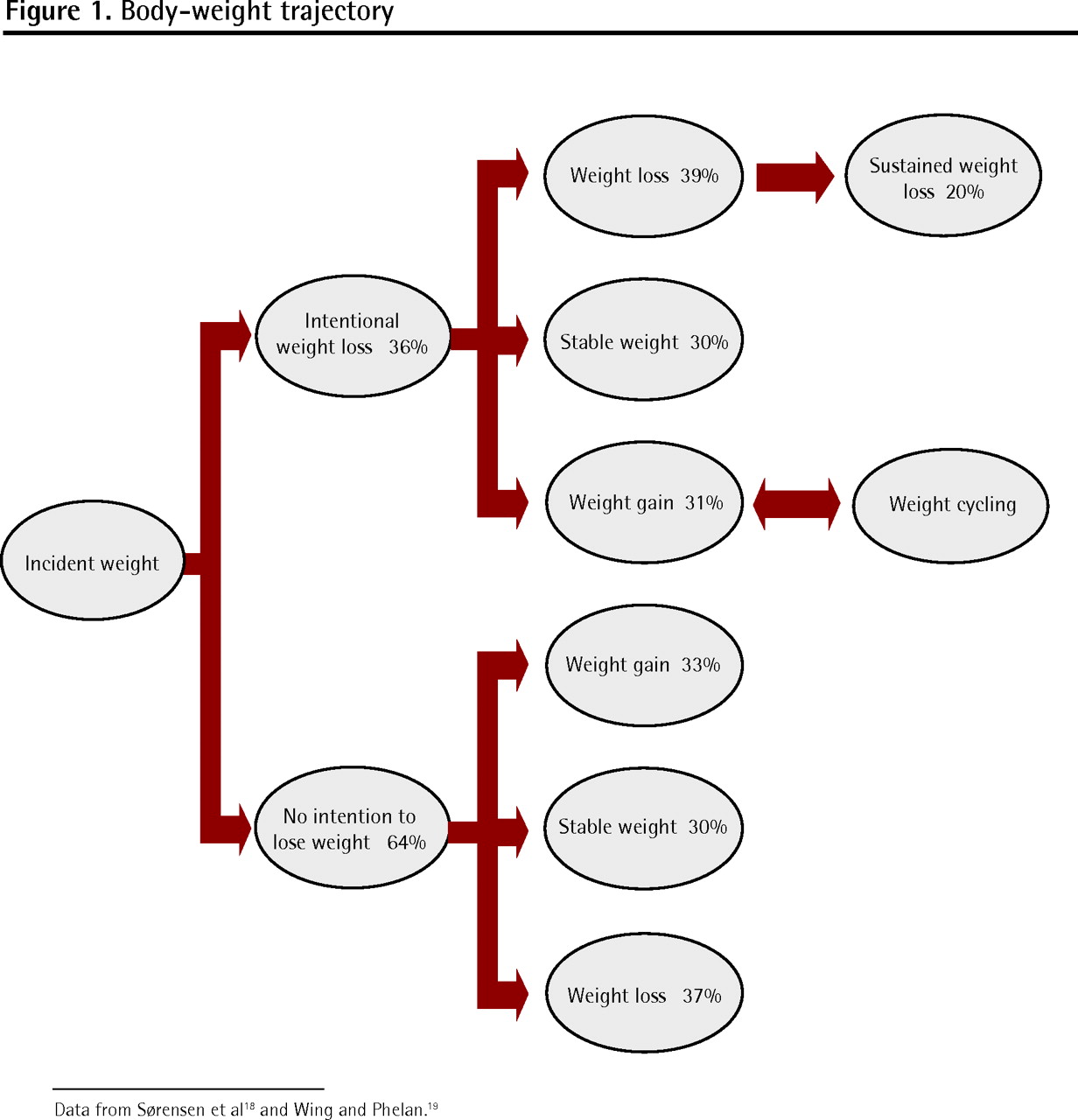
Sørensen et al,18 in a cross-sectional study of healthy adults, showed that at any given time, 36% of the population is attempting to lose weight, while 64% are taking no action to manage weight. Intervention in the weight trajectory, usually with diet and exercise, leads to weight loss, weight cycling with eventual gain, or weight stability. Remarkably, body-size outcomes are similar whether or not there is intention to lose weight—in both groups over the course of 6 years, 30% remain stable, 37% to 39% lose weight, and 31% to 33% cycle or gain weight (Figure 1).18,19

Approximately 17% to 20% of overweight or obese people intentionally lose at least 10% of their body weight and maintain this loss for more than 1 year.19,20
Physiology underlying the weight trajectory
Recent increases in dietary caloric load and reduction in activity level produce an energy mismatch potentially leading to weight gain. Genetics might contribute 25% to 40% of weight-gain susceptibility21; however, the rapid increase in incidence of obesity suggests additional environmental causes, as genetic changes would take much more time.22
In an evolutionary sense, it seems likely that metabolic patterns would be preserved that resist depletion of energy stores in order to promote reproductive success and survival. It follows, therefore, that mechanisms would exist that resist a tendency to intentionally lose weight. Reduced lean body mass requires less energy intake. There is less physical effort required to move that reduced mass and diminished inclination to exercise,23,24 which further reduces energy requirements. There are other metabolic compensations. Ghrelin produced in the stomach increases with fasting, promoting return to previous weight.25 Leptin, a peptide produced in adipocytes, is instrumental in conserving weight under conditions of energy depletion.26,27 Levels drop, producing reduced resting energy expenditure by reducing sympathetic stimulation and increasing vagal activation. Vagal activity enhances insulin secretion, which drives fat back into cells and promotes energy storage.
In the obese state, levels of both insulin and leptin tend to be high, and leptin resistance is present,28,29 so that the mechanism to moderate body weight under conditions of energy repletion is ineffective. Obesity persists along with a state of hyperinsulinemia and continuing energy storage.
There has as yet been no identified mechanism of metabolic compensation to moderate body weight in the obese state. With intentional energy restriction and consumption by diet and exercise, both insulin and leptin levels drop and metabolic processes are initiated for return to original weight. A 10% weight loss can reduce resting energy expenditure by 15%.30 The obese individual who has lost this weight must then continue to diet and exercise even to stabilize at the lower weight,24 otherwise weight cycling occurs, with gradual gain in 80% of those originally attempting weight reduction. The 20% who are successful in maintaining weight loss might not have this marked metabolic compensation,31 and it might be easier for these individuals to maintain their loss over time.32
Optimal weight and the effect of weight trajectory on mortality (Table 4).10,14,33–50
Optimal weight to minimize all-cause mortality is either in the high-normal range14,33 or in the overweight range, in both Canada and the United States.10,34,35 A recent systematic review including 40 observational cohort studies even suggests there is no increase in mortality for those with class 1 obesity.35 Mortality is also minimized if weight remains stable at any level throughout adult life.36,37
Underweight status is associated with increased mortality.35,38 Mortality tends to rise progressively with class 2 and 3 obesity.35,39–43 The relative association of mortality with increased weight tends to decline with age,39 perhaps in part because obesity-related deaths have already occurred by the time elderly status is reached.
Weight gain is generally associated with mortality, particularly if it is excessive.44–46 One systematic review suggests avoidance of weight gain (or loss) of more than 4% in order to minimize effect on mortality. The exception to this is in the late middle years and old age, where a modest weight gain might be protective in those not already overweight or obese.36
Early observational studies suggested an association between weight loss and increased mortality, although these findings were not uniform and the studies did not do a good job of controlling for intentionality and comorbidities. A recent meta-analysis47 confirmed an 11% increase in all-cause mortality in healthy subjects who experienced weight loss. The same study identified a 13% reduction in all-cause mortality if the intentional weight loss occurred in those with weight-related comorbidities. Uniformly, unintentional weight loss is associated with increased mortality.
There is generally little evidence to support weight loss for mortality reduction in healthy subjects older than 60 years.48 There might be some benefit in the elderly with comorbidities such as osteoarthritis, coronary artery disease, and diabetes.49,50 Mortality in this age group has been shown to increase if weight reduction is unintentional, exceeds 5%, or reduces BMI to less than 22 kg/m2.50
Although there has been concern that weight cycling might be associated with increased mortality, there is currently no consensus, with various reviews presenting different conclusions.38,51–54
Weight trajectory and morbidity
Health-related quality of life tends to be lower at both ends of the weight spectrum.55,56 For women it is optimized in the normal weight range, but for men and the elderly it is optimized in the overweight range.56
It is generally agreed that weight loss in obesity can improve health-related quality of life57–59; in fact, if both diet and exercise interventions are employed, weight loss might not be required.60 Improvements to both diet and exercise give additive benefit,61 and exercise can produce improvements at any weight.62–64 Self-evaluated health is often rated higher by individuals who are obese and active than by those who are inactive at normal weight.64 While it is clear that obesity-related health problems are improved by weight interventions, there is disagreement as to whether there are psychological health benefits.
Intervening in the weight trajectory
While there is evidence for improved quality of life among obese patients who have lost weight, there is no evidence for mortality benefit unless there is weight-related comorbidity. Such comorbidity is common in class 1 to 3 obesity, affecting between 70% and 82% of individuals in these groups, depending on obesity severity.65 However, meta-analyses of the best cohort studies suggest that in other weight categories mortality increases with weight loss in otherwise healthy people (Table 4).10,14,33–50
The first priority is to stop excessive weight gain in children through behaviour modification, environmental change, reduction of dietary caloric density, and increased exercise (Table 5).66–68 Similar changes need to be applied for most adults to prevent the usual trajectory of gradual weight gain.
Measures for prevention of excess childhood weight gain
Dietary calorie restriction and compliance are the prominent issues for those attempting weight loss, as results tend to be similar despite manipulation of specific carbohydrate, fat, and protein macronutrients.69 The low-carbohydrate diet is most effective in moderating cardiac risk factors, and the Mediterranean diet provides the maximum benefit for glycemic control. Both tend to be superior to the low-fat diet in affecting these secondary end points.70 Several large prospective cohort studies, however, have raised concerns about increased long-term mortality with the low-carbohydrate diet.71–73 The Mediterranean diet is currently the only intervention consistently associated with reduced mortality.74–76
Exercise is particularly useful in ongoing weight maintenance77,78 and modification of cardiovascular risk factors.79–81 The particularly harmful inflammatory effects of visceral obesity and metabolic syndrome are substantially moderated by exercise.82,83 Ongoing social and environmental change will be necessary to make healthy food choices more available and to increase opportunities for exercise leading to aerobic fitness.21,84
There are some indications for planned weight loss (Table 6), and any strategy should involve thorough examination of harms and possible benefits, along with realistic appreciation of prospects for success. Because compliance is among the most important variables in weight intervention,69 and because the change needs to be lifelong, it is important to consult with the patient to craft a strategy that is likely to be followed. Weight loss, however, need not be a prerequisite to better health. Improved physical fitness, reduction of highly metabolically active abdominal fat, and improvement of cardiovascular risk factors can happen equally well at a stable elevated weight with a commitment to healthier food choices and appropriate exercise.80,82,85–88
Possible indications for intentional weight loss
Conclusion
Prescribed weight loss as a target for all-cause mortality reduction among the overweight and healthy obese is a failed concept both in terms of evidence for benefit and in terms of implementation. Weight reduction among obese individuals with comorbidities or diminished weight-related quality of life can be of demonstrated benefit. In all cases, the aim should be to avoid initial weight gain, prevent ongoing weight gain, and realize physical and metabolic fitness at any size.
Notes
KEY POINTS
Obesity and overweight are more common than “normal” weight in our society. Weight gain averages 0.25 to 0.50 kg per year. Metabolic pathways exist that resist intentional weight loss and that tend to return body mass to the obese state. Weight loss might increase mortality among the healthy obese. Mortality is actually minimized with body mass in the high-normal or overweight range, and the safest body-mass trajectory is weight stabilization with no further gain and optimized physical and metabolic fitness at any size. Initial and continuing weight gain must be avoided through mitigation of the toxic effects of poor diet and low physical activity levels common in our current environment.
Footnotes
-
This article has been peer reviewed.
-
This article is eligible for Mainpro-M1 credits. To earn credits, go to www.cfp.ca and click on the Mainpro link.
-
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro de mai 2012 à la page e246.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}