


Case descriptions
Case 1
A 21-year-old man presents to your emergency department at 2:50 AM with 8-out-of-10 pleuritic, retrosternal chest pain that radiates to his back. He admits to drinking a few beers the previous night but denies drug use. With the exception of a recent upper respiratory tract infection, he has been healthy and his past medical history is unremarkable. On examination you find him to be a fit-looking young man who is in obvious discomfort. He has an axial temperature of 37.9° and he is diaphoretic, but findings of his examination are otherwise normal. A 12-lead electrocardiogram (ECG) reveals 2 mm of ST-segment elevation in multiple leads (Figure 1). About an hour later you learn that his serum troponin level is 7.82 μg/L, his chest pain is worsening, and his ECG is unchanged.

A 12-lead electrocardiogram with features typical of those seen in stage 1 pericarditis: Note the concave (like a happy face) ST-segment elevation in multiple leads without reciprocal ST-segment depression.
Case 2
A 32-year-old man presents to your emergency department at 8:00 PM with sudden onset of 6-out-of-10 chest pain that started while he was unloading his truck. The pain peaked after 5 minutes and improved with rest. He describes his current pain as a “dull ache.” He also has a cough, which he blames on a recent upper respiratory tract infection. His medical history is relevant for smoking and obesity, and there is a family history of premature cardiovascular illness. His examination findings are completely unremarkable. Electrocardiography reveals 1 to 2 mm of ST-segment elevation in leads II, III, and aVF (left foot), and reciprocal depression in aVL (left arm) (Figure 2). Bloodwork results reveal a troponin level of 1.64 μg/L. He tells you his pain is almost completely gone and he wants to go home.
A patient presenting to the emergency department with sudden-onset chest pain, ST-segment elevation on his or her ECG, and elevated cardiac biomarkers should alert any clinician to the possibility of acute myocardial infarction (AMI). However, acute pericarditis, myocarditis, or myopericarditis are also associated with these findings. The lack of a true criterion standard for diagnosing pericarditis and myocarditis makes it challenging to differentiate these diseases from AMI.1,2 Early recognition of AMI is crucial for timely initiation of revascularization protocols. Therefore, having a systematic approach to differentiating pericarditis and myocarditis from AMI can help the clinician initiate the appropriate management without delay. The purpose of this article is to review basic features of acute pericarditis and myocarditis and to provide an approach to help clinicians make a timely diagnosis.

A 12-lead electrocardiogram with features of an inferior ST-segment elevation myocardial infarction: Note the horizontal ST-segment elevation in leads III and aVF with reciprocal depression in aVL.
Causes
Acute pericarditis occurs when the bilayered pericardial sac becomes inflamed. In most cases, the cause of pericarditis is idiopathic or is assumed to be due to a viral infection.1,3 There are several less common infectious and noninfectious causes of pericarditis, but most patients with acute pericarditis present with a history suggestive of recent or concurrent viral illness. Finding the cause of acute pericarditis usually has little bearing on its management in the emergency department,1,3,4 and most cases resolve with no long-term sequelae. While pericardial effusions might develop as a result of pericarditis, they are usually minor and rarely result in cardiac tamponade.
Acute myocarditis can result from a focal or diffuse infection of the myocardium.2,5 Myopericarditis occurs when the inflammation extends to the pericardium and it can be very difficult to distinguish from pure myocarditis or pericarditis using routine emergency department tests. As is the case with pericarditis, viruses are the most common causative agents in myocarditis, but the cause can also be bacterial, fungal, or noninfectious. The clinical presentation of myocarditis can range from minor chest pain to cardiogenic shock. Indeed, myocarditis is associated with more serious long-term sequelae than pericarditis is, the most serious of which are dilated cardiomyopathy and heart failure.
Presentation
Acute pericarditis and myocarditis are diseases that often present with nonspecific signs and symptoms, many of which might also be seen in AMI. Irritation of the pericardium typically causes acute retrosternal chest pain that radiates to the back, neck, or arms.1 The pain might be pleuritic and can be relieved when the patient sits upright or leans forward. Other symptoms suggestive of a recent or concomitant viral illness, such as fatigue, fever, chills, or respiratory or gastrointestinal symptoms, might also be present in either pericarditis or myocarditis. Dyspnea, decreased exercise tolerance, palpitations, or syncope are more suggestive of myocarditis.2,5 The development of a pericardial effusion can be characterized by an audible friction rub, but this sign is often difficult to appreciate in a noisy emergency department.1−3,5
Electrocardiogram findings
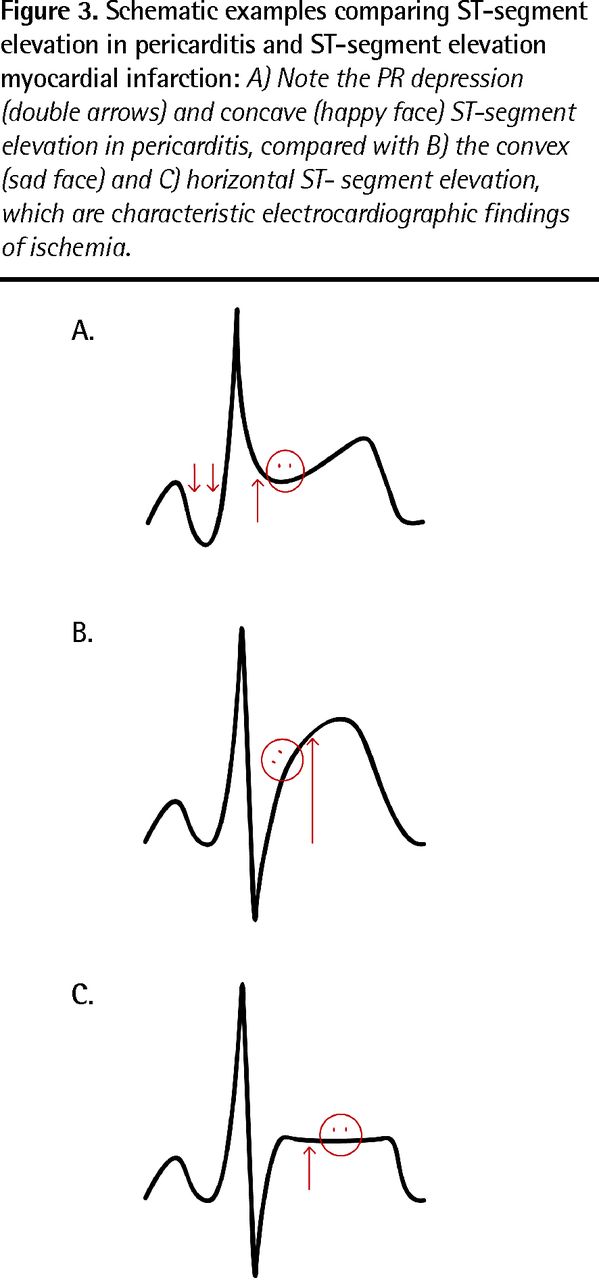
Patients with acute pericarditis or myocarditis usually present in normal sinus rhythm or with sinus tachycardia.2,3,6 The sensitivity of ECG for myocarditis is low.5 Electrocardiographic findings can range from nonspecific ST and T wave abnormalities to ST changes resembling ischemia. In contrast, pericarditis and myopericarditis are associated with characteristic 12–lead ECG findings classically described in 4 progressive stages.3,6 Stage 1 is encountered most often in the emergency department because it can last up to 2 weeks and might not progress to later stages if it is diagnosed and treated promptly (Figure 1). These include ST-segment elevation in multiple leads (measured from the TP segment to the J point) and PR depression. Minimal ST depression might be observed in aVR (right arm) (which is by definition a reciprocal lead) or V1,6 but reciprocal ST depression in any other lead represents ischemia. The morphology of ST segments is always concave (like a happy face) in pericarditis. In contrast, as seen in case 2 (Figure 2), horizontal or convex ST segments (like a sad face) represent ischemia until proven otherwise. Figure 3 shows schematic representations that illustrate these important differences. Stages 2, 3, and 4 ECG findings consist of ST-segment normalization and T wave flattening, T wave inversion, and normalization of T waves, respectively.
Elevated levels of troponin I are reasonably specific for pericarditis and myocarditis, but they are not sensitive for either syndrome.1,2,5 Higher levels are suggestive of myocarditis. Other elevated serologic markers including white cell count, erythrocyte sedimentation rate, and serum C-reactive protein have limited diagnostic value.
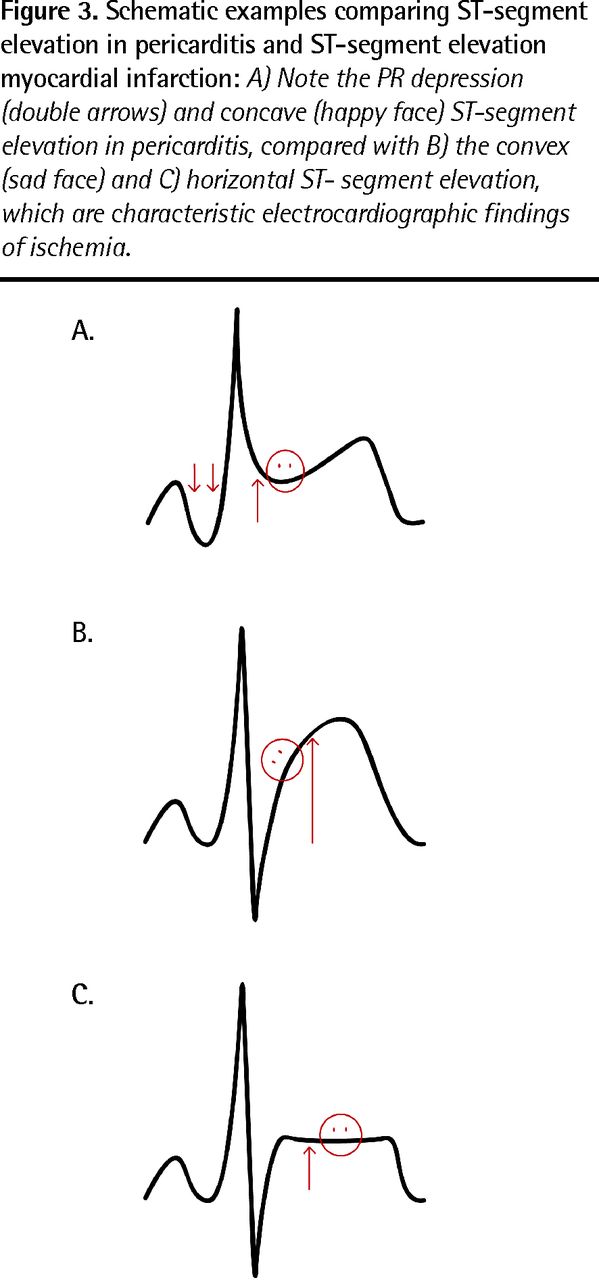
Schematic examples comparing ST-segment elevation in pericarditis and ST-segment elevation myocardial infarction: A) Note the PR depression (double arrows) and concave (happy face) ST-segment elevation in pericarditis, compared with B) the convex (sad face) and C) horizontal ST-segment elevation, which are characteristic electrocardiographic findings of ischemia.
Back to our cases
Case 1
The patient is diagnosed with pericarditis based on his ECG findings and clinical presentation. His pain continues to worsen despite generous analgesic and anti-inflammatory medications, and serial measurement of troponin levels reveals an upward trend that peaks at 14.36 μg/L. The cardiology department is consulted. Later that morning, results of an angiogram reveal pristine coronary arteries. He is admitted to hospital for several days and is discharged with the diagnosis of myopericarditis.
Case 2
The patient is diagnosed with an inferior ST-segment elevation myocardial infarction based on his ECG findings (ST elevation in the inferior leads with reciprocal changes in aVL), elevated troponin levels, and history of the presenting illness. He is referred to cardiology for an urgent angiogram, which reveals 90% occlusion of his right coronary artery. Following stenting and an unremarkable hospital course, he is discharged home with the diagnosis of ST-segment elevation myocardial infarction.
Further reading and resources
For physicians
Dr. Smith's ECG blog. Minneapolis, MN. Available from: http://hqmeded-ecg.blogspot.com.
C3 Project: pericarditis and tamponade with Dr Amal Mattu [podcast]. In: Emergency medicine: reviews and perspectives. Burbank, CA: EMRAP Inc; 2011 August. Available from: www.emrap.org/episode/2011?link=episode-guide.
Punja M, Mark DG, McCoy JV, Javan R, Pines JM, Brady W. Electrocardiographic manifestations of cardiac infectious-inflammatory disorders. Am J Emerg Med 2010;28(3):364–77.
For patients
MedicineNet [website]. Pericarditis. New York, NY: WebMD; 2012. Available from: www.medicinenet.com/pericarditis/article.htm.
MedicineNet [website]. Myocarditis. New York, NY: WebMD; 2012. Available from: www.medicinenet.com/myocarditis/article.htm.
Acknowledgment
We thank Mr Ramin Eshraghi-Yazdi for producing Figure 3. He designed the images in this figure for this article and they have been reproduced with his expressed consent.
Notes
BOTTOM LINE
-
Acute pericarditis and myocarditis usually present with features suggestive of viral illness and with chest pain that is pleuritic and retrosternal, and that radiates to the back or neck. This pain is often relieved when the patient sits upright or leans forward.
-
Pericarditis is usually self-limiting and resolves with no longterm sequelae; however, myocarditis can lead to serious cardiac pathology.
-
The most common electrocardiographic finding in acute pericarditis and myopericarditis is concave (like a happy face) ST-segment elevation in multiple leads. Horizontal or convex (like a sad face) ST elevation with reciprocal ST depression are features of ischemia.
-
While serum troponin I levels might be elevated in pericarditis and myocarditis, serology results alone should not be used to make the diagnosis.
POINTS SAILANTS
-
La péricardite et la myocardite sous forme aiguë se présentent habituellement avec des caractéristiques laissant présager une maladie virale et comportant des douleurs thoraciques pleurétiques et rétrosternales qui irradient vers le dos ou le cou. Cette douleur est souvent soulagée quand le patient s'assied le dos droit ou se penche vers l'avant.
-
La péricardite est habituellement résolutive et se résorbe sans causer de séquelles à long terme; par contre, la myocardite peut entraÎner des cardiopathies sérieuses.
-
Le tracé sur les électrocardiogrammes le plus courant dans les cas de péricardite et de myopéricardite aiguës est une élévation du segment ST concave (comme un visage souriant) en répétitions multiples. L'élévation du ST horizontale ou convexe (comme un visage triste) avec une dépression du ST réciproque sont des caractéristiques d'une ischémie.
-
Si les dosages de la troponine I sérique peuvent être élevés dans les cas de péricardite et de myocardite, les résultats sérologiques à eux seuls ne devraient pas être utilisés pour poser le diagnostic.
Emergency Files is a quarterly series in Canadian Family Physician coordinated by the members of the Emergency Medicine Program Committee of the College of Family Physicians of Canada. The series explores common situations experienced by family physicians doing emergency medicine as part of their primary care practice. Please send any ideas for future articles to Dr Robert Primavesi, Emergency Files Coordinator, at robert.primavesi{at}mcgill.ca.
Footnotes
-
Competing interests: None declared
- Copyright © the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.