


Abstract
Objective To determine to what extent FPs teach and use pneumatic otoscopy and to identify the chief influences on this behaviour.
Design Mixed-methods descriptive study conducted between March and May 2011.
Setting The family medicine residency program at Laval University in Quebec city, Que.
Participants Directors of the family medicine teaching units (FMTUs), teachers, and residents.
Methods We used questionnaires to assess the availability of pneumatic otoscopy equipment in 12 FMTUs, current behaviour and behavioural intention among physicians (residents and teachers) to use or teach pneumatic otoscopy, and facilitators and barriers to these practices. We also conducted 2 focus groups to further explore the facilitators of and barriers to using pneumatic otoscopy. We used descriptive statistics for quantitative data, transcribed the qualitative material, and performed content analysis.
Main findings Eight of the 12 FMTUs reported having pneumatic otoscopy equipment. Four had it in all of their consulting rooms, and 2 formally taught it. Nine (4%) of 211 physicians reported regular use of pneumatic otoscopy. Mean (SD) intention to teach or use pneumatic otoscopy during the next year was low (2.4 [1.0] out of 5). Teachers identified improved diagnostic accuracy as the main facilitator both for use and for teaching, while residents identified recommendation by practice guidelines as the main facilitator for use. All physicians reported lack of availability of equipment as the main barrier to use. The main barrier to teaching pneumatic otoscopy reported by teachers was that they did not use it themselves. In focus groups, themes of consequences, capabilities, and socioprofessional influences were most dominant. Residents clearly identified role modeling by teachers as facilitating the use of pneumatic otoscopy.
Conclusion Pneumatic otoscopy is minimally used and taught in the family medicine residency program studied. Interventions to increase its use should target identified underlying beliefs and facilitators of and barriers to its use and teaching.
Otitis media—acute otitis media and otitis media with effusion—is the most common diagnosis in children consulting FPs.1–4 Establishing the presence of middle-ear effusion is a key criterion for an accurate diagnosis.5–9 Since 2004, all North American guidelines have recommended using pneumatic otoscopy to this end.10–13
Pneumatic otoscopy is a simple, inexpensive, reliable, and easily accessible tool for FPs. It enables us to evaluate the degree of mobility of the tympanum, a reliable sign of the presence of middle-ear effusion. The accurate diagnosis of otitis media is important, as middle-ear problems are overdiagnosed, leading to unnecessary and inappropriate use of antibiotics.14–16 Assessing the duration of effusion is essential to appropriately managing otitis media with effusion.
Little is known about the rate of current use of pneumatic otoscopy by FPs, but it appears to be low; in 2002, a survey conducted by MacClements et al of 193 family medicine residents in Texas and Oklahoma reported consistent use by 15% of FPs and occasional use by 66% of FPs.16 In pediatric practices, a recent study reported a low average use (33%) in the diagnosis of otitis media with effusion.17 However, the study assessed the combined use of pneumatic otoscopy with tympanometry, thus possibly overestimating the use of pneumatic otoscopy. Only MacClements et al have attempted to identify why pneumatic otoscopy might not be used; the most commonly cited reason in that study was lack of training and lack of availability of equipment.16 Although that study was informative, there is still a knowledge gap for those who aim to modify the clinical behaviour of FPs so that they implement pneumatic otoscopy as recommended in clinical guidelines.
Changing the clinical behaviour of health care professionals requires a better understanding of the underlying psychological determinants of behaviour. Based on a systematic review of 76 studies of sociocognitive theories applied to predicting health care professional behaviour, Godin et al proposed a theoretical framework for the study of health care professionals’ behaviour and intended behaviour, which identified the following determinants: beliefs about consequences (indicator of attitude), beliefs about capabilities (self-efficacy in performing the behaviour), socioprofessional influences (peer influence), moral norm (moral obligation felt toward the proposed behaviour), role and identity (professional role and self-standards), characteristics of the health care professional, and habit or past behaviour.18
Our study objectives were to determine the extent of use and teaching of pneumatic otoscopy in the family medicine residency program at Laval University in Quebec city, Que, and to use the framework of Godin et al to understand the determinants of this behaviour.18
METHODS
Study design
We conducted a mixed-methods descriptive study between March and May 2011, consisting of a survey of the directors of all 12 family medicine teaching units (FMTUs) affiliated with Laval University concerning pneumatic otoscopy equipment and teaching activities; a survey of FPs (teachers and residents) of the FMTUs concerning the technique; and 2 focus group discussions concerning the technique in 1 FMTU.
Participants and data collection
Survey of FMTU directors
A self-administered questionnaire was sent by e-mail in March 2011 to the directors of the 12 FMTUs. The e-mail explained the purpose of the survey, showed a photograph of pneumatic otoscopy equipment, and asked 3 questions:
-
Is pneumatic otoscopy equipment available in your FMTU? (yes or no)
-
If so, where is this equipment available? (all consulting rooms or a separate location)
-
What educational activities on pneumatic otoscopy do you offer residents? (none, clinical supervision, or formal group teaching)
In the case of nonresponse, a follow-up e-mail was sent 1 week after first contact.
Survey of teachers and residents
We used a self-administered questionnaire to assess the intention to use pneumatic otoscopy among residents and teachers. The teachers’ questionnaire included additional items, as we were also assessing their intention to teach pneumatic otoscopy. We included 3 items assessing each behavioural intention of interest.19 We also included a list of facilitators of and barriers to using or teaching pneumatic otoscopy. All items on behavioural intention and facilitators or barriers were measured on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree).
Physicians were invited to complete the questionnaire on a voluntary basis. To ensure optimal participation, the questionnaire was distributed immediately before or after teaching or administrative activities. Physicians not attending these meetings were invited to complete the questionnaire at another time.
Focus group
For our qualitative survey, we sought discussion among both users and nonusers of pneumatic otoscopy. Our quantitative results showed that 2 FMTUs had the best balance of users and nonusers, and for feasibility reasons we chose only 1 of these 2 sites to conduct focus groups. We organized 2 distinct 1-hour focus groups at the selected FMTU: one for teachers and another for residents. We developed an interview guide and one of the authors (L.C.), who had extensive expertise in group facilitation, led the group discussion. Participants spoke freely about their experiences with pneumatic otoscopy, and after a short presentation of the quantitative survey results, they discussed how to promote use and teaching of pneumatic otoscopy. Three members of the research team acted as nonparticipant observers (E.O., M.L., and K.C.). Discussions were audiorecorded and transcribed verbatim.
Data analysis
Quantitative data
The mean score of intention to use or teach pneumatic otoscopy was calculated by averaging the score of the 3 relevant questions for each behaviour. The internal consistency of behavioural intention constructs was assessed with a Cronbach α coefficient. We explored the association between intention to use or teach and current behaviour using a χ2 test (current use was defined as reporting using pneumatic otoscopy with at least 1% of relevant patients).
Qualitative data
Two approaches were used to validate our interpretation of the qualitative data and maximize its credibility. First, for each focus group, a report, including comments by participants, observers’ perception of participants’ opinions, and general comments on group dynamics, was written by 1 of the observers, based on the notes of the 3 observers. These reports were reviewed by all team members and then further reviewed by 3 volunteer participants from each focus group (teachers and residents).
Second, transcripts of the focus group proceedings were coded independently by 2 individuals (E.O. and a research assistant) using the integrated sociocognitive framework proposed by Godin et al for the study of health care professionals’ behaviour and intention of behaviour.18 Codifications were compared and validated by another member of the research team (F.L.). Although we coded qualitative data according to predefined variables from the conceptual framework, we also used open codification to allow for emerging themes. NVivo software, version 9, was used to perform these qualitative analyses. Results of analysis using both deductive and inductive approaches and triangulation of coding, including member checking, were reviewed by 4 of the team members (E.O., F.L., M.L., and L.C.) and were found to be very similar. When there was disagreement, consensus was reached.
As all focus groups were conducted in French, verbatim excerpts presented in the Results section were translated into English by an independent translator and were independently reviewed by a multilingual person. The final version was obtained by consensus involving the principal investigator (E.O.).
FINDINGS
Survey of FMTU directors
Each director of the 12 FMTUs responded to the questionnaire. Eight (67%) of the 12 FMTUs had pneumatic otoscopy equipment. Four directors said it was available in all the consulting rooms and 4 said it was only available in some. Pneumatic otoscopy was not taught in 6 of the FMTUs. Teaching pneumatic otoscopy was reported to occur only during clinical activities in 4 FMTUs, while 2 (17%) offered both formal and clinical teaching of pneumatic otoscopy.
Survey of teachers and residents
Among 318 eligible physicians from the 12 FMTUs, 211 (111 residents and 100 teachers) completed the survey (66%). Table 1 shows the characteristics of the participants.
Sociodemographic characteristics of participants:N = 211.
Frequency of use and teaching of pneumatic otoscopy
Although 98% of FPs reported seeing patients with middle-ear problems during a 1-month period of regular practice, only 9 (4%) of them (3 residents and 6 teachers) reported regular use of pneumatic otoscopy. Five (2%) FPs (all residents) admitted not knowing what pneumatic otoscopy was. Eighty-four percent of participants reported never using pneumatic otoscopy when seeing patients with middle-ear problems during a 1-month period of regular practice, 13% used it in 1% to 20% of these patients, and 3% used it in more than 20% of these patients.
Twice as many teachers as residents (38% vs 19%) stated that they had received training on how to use pneumatic otoscopy. One-quarter of teachers stated they had never taught pneumatic otoscopy. Among residents who had not been trained in the use of pneumatic otoscopy, most believed that the technique should be taught (Table 2).
Reported pneumatic otoscopy teaching activities in the family medicine residency program at Laval University in Quebec city, Que: N = 211.
Intention to use and teach pneumatic otoscopy
The mean (SD) scores for intention to use pneumatic otoscopy in the next year among residents and teachers were 2.5 (0.9) and 2.3 (1.1) out of 5, respectively. This means that, in terms of proportion, 12% of residents reported their intention to use pneumatic otoscopy in the next year and less than 1 teacher out of 5 intended to use or teach it in the same period (Table 3). Strong or very strong intention to use pneumatic otoscopy was associated with current use (44% of those with strong or very strong intentions were current users vs 9% of those without such strong intentions, P < .001). Among teachers, the mean (SD) score for intention to teach the technique was 2.4 (1.0). Strong or very strong intention to teach pneumatic otoscopy was associated with current teaching (48% vs 5%, P <.001).
intention to use or teach pneumatic otoscopy in the next year among residents and teachers in the family medicine residency program at Laval University in Quebec city, Que: Cronbach coefficients for the 3 measures of intention were .92 for intention to use pneumatic otoscopy among residents, .93 for intention to use it among teachers, and .94 for intention to teach it; N = 211.
Facilitators and barriers
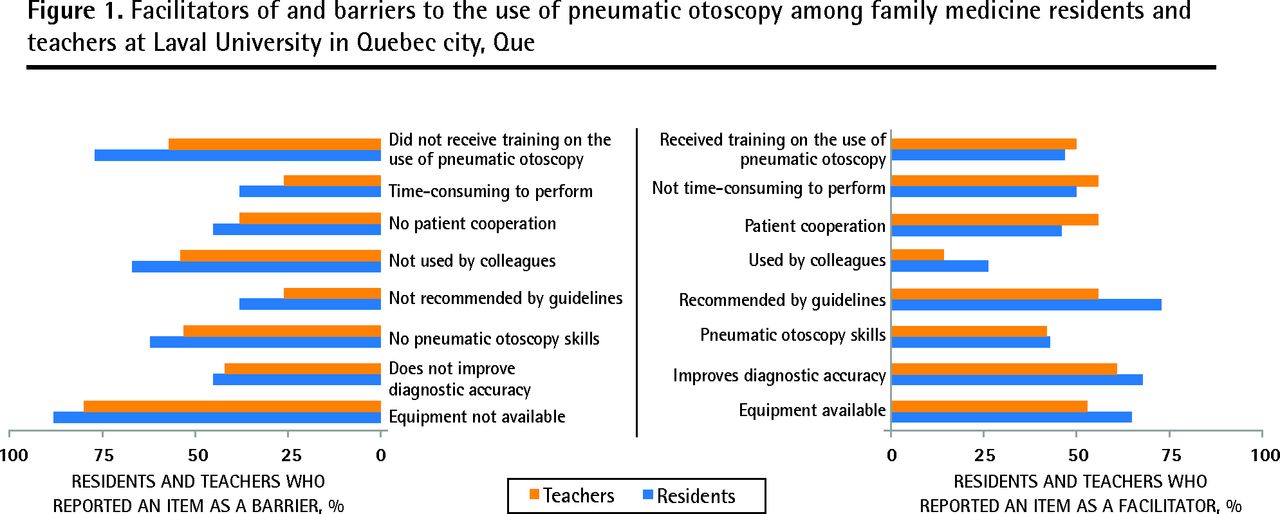
Among residents, the 3 main facilitators of using the technique were use recommended in clinical practice guidelines (73% agreed or strongly agreed the factor was a facilitator), contribution to improving diagnostic accuracy (68%), and availability of equipment (65%). For teachers, contribution to improving diagnostic accuracy was the most frequently identified facilitator (61%). Tied for second place were speed of the technique, practice guidelines recommendations, and patient cooperation (all 56%). Residents and teachers identified similar barriers to using the technique: unavailability of equipment, lack of training, and nonuse by colleagues (Figure 1).

Facilitators of and barriers to the use of pneumatic otoscopy among family medicine residents and teachers at Laval University in Quebec city, Que
The main facilitators of teaching pneumatic otoscopy were its contribution to improving residents’ diagnostic accuracy, patient cooperation, and its speed of teaching (Figure 2). The main barriers to teaching were that teachers did not use it themselves, lack of availability of equipment, and the fact that few colleagues taught it.

Facilitators of and barriers to teaching pneumatic otoscopy among family medicine teachers at Laval University in Quebec city, Que
Focus groups
Nine teachers and 8 residents (7 first-year residents and 1 second-year resident) agreed to participate in the focus groups. Key themes that emerged were classified according to 4 sociocognitive constructs: beliefs about consequences, beliefs about capabilities, socioprofessional influences, and habit or past behaviour. Some beliefs were classified as knowledge (emerging theme), but we did not classify any beliefs according to the following 2 constructs: role and identity, and characteristics of the health care professional. Most observations were classified under 3 categories: beliefs about consequences, beliefs about capabilities, and socioprofessional influences. Most of them translated into a decreased likelihood of using and teaching pneumatic otoscopy.
Key themes identified within relevant domains
Ten beliefs mapped to the beliefs about consequences construct, almost all of which related to factors decreasing the likelihood of using and teaching pneumatic otoscopy. The FPs (especially teachers) were not convinced of the advantage of pneumatic otoscopy for diagnostic accuracy:
You’d have to really convince me that it’s worth it ... will it really change my practice?
(Teacher)
The advantages have to be clear ... if we’re going to use it, we have to know what more it offers us.
(Teacher)
We know it’s useful but if we were shown how it could really help us in our diagnosis ...
(Resident)
One person admitted that for otitis media with effusion, it might be of some advantage: “[I]t sometimes gives you a better idea if it’ll get better quicker.” (Teacher)
Beliefs about capabilities (7 beliefs) were expressed in both groups, although more often among residents. All of them related to factors that decreased the likelihood of using and teaching pneumatic otoscopy: lack of training, non-operational equipment, uncooperative patients, and lack of standardized teacher training:
I tried it and found it hard to use with children, especially young children: they cried and fought. It was so complicated; it took a lot of time, especially in walk-in clinic, so I dropped it, perhaps partly because of lack of practice, even though I did find it useful.
(Resident)
I use it with adults, but I don’t use it with children; I find it annoying—they cry, they move around. (Teacher) It’s hard to teach it when I’ve never been taught it myself.
(Teacher)
Fourteen beliefs were grouped under the domain of socioprofessional influences. Nonuse of pneumatic otoscopy by teachers (family physicians or other specialists) was a crucial factor that decreased the likelihood that residents would use it.
We are influenced a lot by what our teachers do.
(Resident)
If the teachers hardly ever use it or not at all, why would they teach us the technique?
(Resident)
I did a 2-month internship in pediatrics and we never, ever used it.
(Resident)
However, residents reported that incorporating pneumatic otoscopy into premedical courses (eg, when learning the ear, nose, and throat examination) could increase the likelihood of its use: “At least they should start pneumatic otoscopy training in premed so that in clerkship you know what it is.” (Resident)
Among teachers, many referred to the nonuse of the technique by colleagues as a factor that decreased the likelihood of their using and teaching the technique: “There aren’t a whole lot of people who are convinced that we should do it every time … and to what extent it would change our practice.” (Teacher)
Recent symposia promoting clinical guideline recommendations would increase the likelihood of its being used and taught: “For sure if we hear more and more about it in conferences we’ll use it.” (Teacher)
Some teachers claimed that the residency program should promote the use and teaching of the technique through standardized teacher training and as a learning goal for residents, while one teacher argued that it is the physicians’ responsibility to learn any evidence-based practices as part of continuing medical education and that this is not the responsibility of program directors.
With regard to habit or past behaviour, only 1 teacher reported regularly using and teaching pneumatic otoscopy and 1 resident reported occasionally using it when in doubt. The others had rarely or never used the technique in the past year.
With regard to knowledge, unfamiliarity or disagreement with the content of guidelines was the factor that emerged:
Yes, it’s in the clinical guidelines, but is it really worth it to spend the money [on the equipment for the FMTUs] and to put our energy into teaching the technique ... it won’t necessarily change much in terms of patient outcomes.
(Resident)
DISCUSSION
Our study aimed to determine and understand the extent of the use and teaching of pneumatic otoscopy in the family medicine residency program at Laval University. Pneumatic otoscopy is a technique that is very minimally used and taught in the program, and intention to use or teach it during the next year is low or moderate.
We were surprised by these results, as the validity of this technique has been clearly demonstrated, and it should be used as a routine examination. Many North American organizations strongly recommend using pneumatic otoscopy in practice.10–13 Even in Quebec, the Institut national d’excellence en santé et en services sociaux recommends assessment of eardrum mobility in its antibiotic treatment guidelines.20 If we consider our study as an evaluation of the quality of medical care using objective criteria, with practice guidelines of recognized organizations as the standards to follow, then performance is very weak.
The main reported barrier to the use and teaching of pneumatic otoscopy was lack of equipment. Only 4 of the 12 FMTUs had the equipment in all consultation offices. However, our results suggest that not having the equipment is closely related to negative attitudes about the technique, negative beliefs about capabilities, and negative social influences. If someone is unfamiliar or even disagrees with the usefulness of the technique and the recommendations of practice guidelines and does not know how to perform it—which we observed in both the quantitative and qualitative components of our study—he or she will not purchase equipment.
Our results suggest that the use and teaching of pneumatic otoscopy in the family medicine program is dependent on many factors. Physicians must be convinced of its merits and have the skills to use and teach it. It should be initially learned during premedical training and clerk-ship, and not during residency, where “fine tuning” learning should be integrated into other educational activities without cutting or adding to the current program content.
Teachers should be aware that they transmit a negative message by not using pneumatic otoscopy themselves in their practices. In this regard, it is surprising that 38% of teachers (twice as many as residents) said they had personally received training in pneumatic otoscopy, 25% said they had taught it, and only 6% reported using it regularly. Another important barrier to widespread use and teaching of the technique in Quebec is that the “champions” of pneumatic otoscopy are currently concentrated in just a few teaching units. As our conceptual framework attests,18 past behaviour of using and teaching the technique indicates an intention to continue.
Our study has many strengths. First, our sample represents the entire network of the 12 FMTUs at Laval University. We obtained a high participation rate (66%) of eligible physicians. This is comparable with that obtained by MacClements et al16 and higher than usual response rates in surveys carried out in academia. In addition, the distribution of physicians according to their status and sex was similar among respondents and all the FPs associated with the residency program. Second, we used a mixed methodology (both surveys and focus groups) to better describe and understand the situation and to ensure the validity and credibility of the results. Questionnaires and analyses were based on a robust theoretical framework.18 As recommended, we triangulated data collection methods and interpretation of qualitative data in addition to verifying data interpretation by participants in focus groups.21
Limitations
The questionnaire on the facilitators and barriers of the technique seems to have been difficult to answer for some of the FPs. Careful analysis of combined data, taking into account the open-ended questions, found that respondents might have misinterpreted some questions. This led to an underestimation of some factors.
A social desirability bias might be the cause of the high proportion of residents (86%) stating that pneumatic otoscopy should be taught in the residency program. People who are learning naturally want to be taught everything that they might possibly need to know. Comments made during the resident focus group indicate that even if there is interest, the results should be interpreted with caution. Residents believe that pneumatic otoscopy should be taught before the residency and then integrated into relevant parts of the residency program, supervised by family doctors who practise the technique themselves.
We would have liked to include a larger number of users of the technique in our focus groups. Unfortunately, only 1 or 2 attended each meeting. However, as most physicians in the program do not use pneumatic otoscopy, thoughts and opinions expressed were more in line with those of physicians in average teaching units, although perhaps slightly affected by the “user subculture” of (absent) users working in their teaching units.
While our results accurately describe the situation in the family medicine residency program at Laval University, it is difficult to extrapolate to other family medicine educational settings in Canada. Anecdotal reports from residents who completed their undergraduate medical studies in other universities in Quebec suggest that the use and teaching of pneumatic otoscopy are also low elsewhere. Our study was used to assess and understand one situation in depth, but an e-mail survey of the directors of teaching units across Canada might paint a picture of the situation on a larger scale.
Conclusion
The marginal use and teaching of pneumatic otoscopy in one family medicine residency program in Canada demonstrates the complexity of the application of evidence in clinical practice. Even providing all practices with accessible and operational equipment would not guarantee that pneumatic otoscopy would be used and taught. An intervention to change behaviour in this context might be challenging. It should target the negative beliefs about the clinical utility of the technique and capacity to perform it, the negative socioprofessional influences, and the logistical barriers (eg, lack of operational equipment), while focusing on teachers as role models.
Acknowledgments
We thank Sun Makosso-Kallyth for help with statistical analysis.
Notes
EDITOR’S KEY POINTS
-
Pneumatic otoscopy is very minimally used and taught in the family medicine residency program at Laval University, and intention to use or teach it during the next year is low or moderate.
-
The main reported barrier to the use and teaching of pneumatic otoscopy was lack of equipment. Only 4 of the 12 family medicine teaching units had the equipment in all consultation offices.
-
An intervention to change behaviour in this context should target the negative beliefs about the clinical utility of pneumatic otoscopy and capacity to perform it, the negative socioprofessional influences, and the logistical barriers (eg, lack of operational equipment), while focusing on teachers as role models.
POINTS DE RÈPERE DU RÉDACTEUR
-
L’otoscopie pneumatique n‘est à peu près pas utilisée et très peu enseignée dans le programme de résidence en médecine familiale à l’Université Laval, et il y a peu ou pas d’intention de l’utiliser ou de l’enseigner au cours de la prochaine année.
-
Le principal obstacle à l’utilisation de l’otoscopie pneumatique et à son enseignement était le manque d’équipement. Seulement 4 des 12 unités d’enseignement en médecine familiale possédaient cet appareil dans les bureaux de consultation.
-
Afin d’améliorer la façon de faire dans ce domaine, il faudrait s’attaquer aux croyances négatives concernant l’utilité clinique de l’otoscopie pneumatique et la capacité de l’utiliser, aux influences socioprofessionnelles négatives et aux obstacles logistiques (p. ex. l’absence d’équipement), tout en insistant sur le modèle de rôle que doivent jouer les professeurs.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Contributors
All authors of this paper have directly participated in the planning, execution, or analysis of the study, and all authors have read and approved the final version submitted.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.