


Abstract
Objective To assess the feasibility and acceptability of administering the validated Case-finding Health Assessment Tool (CHAT) in Canadian family practice waiting rooms to identify risk factors for depression, anxiety, anger control, smoking, drinking, other drug use, gambling, exposure to abuse, and physical inactivity.
Design Cross-sectional survey.
Setting One urban academic family practice and one inner-city community health centre in British Columbia.
Participants Convenience sample of consecutive adult patients (19 years of age or older) and their attending family physicians.
Main outcome measures Rates of completion; positive responses to and wanting help with identified lifestyle and mental health risk factors; rates of objections to any questions; and positive and negative comments about the CHAT by participating physicians and patients.
Results A total of 265 eligible adults presented in the waiting rooms over 5 full days and 3 half-days, 176 (66%) of whom enrolled in the study; 161 (91%) completed the CHAT, and 107 (66%) completed acceptability feedback forms. The prevalence of risk factors among patients in the academic and inner-city practice samples was different, with 20% and 63%, respectively, recording positive responses to both depression screening questions, 34% and 60% positive for anxiety, 11% and 71% currently smoking, 6% and 22% feeling they needed to cut down on alcohol, 1% and 48% having used recreational drugs in the past year, and 11% and 65% with problems controlling anger. While many requested help with reducing risk factors, such as smoking (20%) and mental health symptoms (25% to 27%), a total of 35% (57 of 161) wanted help with an identified issue that day. Patients and physicians found the CHAT acceptable, with no patients objecting to any question except the alcohol question (2 objected). Most comments were positive.
Conclusion The CHAT allowed efficient identification of 9 risk factors, as well as identification of those wanting help. It could be used to screen all or targeted adult Canadian primary care patients in waiting rooms.
Physical and mental health and substance misuse are often interwoven.1 Therefore, preventive care in family practice should involve identifying and addressing both lifestyle and mental health risk factors. However, many at-risk behaviour patterns and conditions are not identified in routine practice.2 Mental health issues in particular are common in North America.3,4 In Quebec, 25% of family practice consultations are for mental health problems,5 and 10% of Canadians use services for their mental health annually, with family physicians being the most commonly consulted professionals.3 However, only 40% of those with mental health problems seek professional help.3 Further, identification of and subsequent intervention for modifiable risk factors such as smoking, problematic drinking, and physical inactivity can have a strong positive influence on many chronic conditions, such as heart disease, diabetes, chronic obstructive pulmonary disease, and lung cancer.6
In Canada, 85% of those aged 12 and older reported having a regular medical doctor in 2009.7,8 Family practice provides an ideal setting for identifying and addressing lifestyle and mental health risk factors. Routine screening for these potentially modifiable risk factors is likely to have much better coverage than opportunistic screening.9 However, given visit time restraints, routine screening rates for individual items such as depression can be low.10
The Case-finding Health Assessment Tool (CHAT) is a short, self-administered tool for lifestyle and mental health assessment of adult patients in family practice. The CHAT was developed by a multidisciplinary team (including family physicians, nurses, and psychologists) from the University of Auckland in New Zealand. The tool assesses for risky behaviour (smoking, drinking, other drug use, gambling, exposure to abuse, and physical inactivity) and mental health issues (depression, anxiety, and anger control) and can be administered in the waiting room in less than 5 minutes, before the physician visit. For each item, patients are asked if the issue is something they would like help with and, if the answer is yes, whether they want help that day. By combining substance use, other risky health behaviour including violence, and negative mood states, the CHAT recognizes the interrelationship of these domains and how intervening in one can have positive effects on another. The tool has undergone testing for acceptability (less than 1% of more than 2500 patients objected to any question), reliability,11–13 and validity in New Zealand. The addition of the question about help increases test specificity (reducing false positives).13–15 The multi-item nature also allows for assessment of comorbidities.16 It has been assessed with white, Maori, and Pacific Island11 and Asian peoples,13 with high patient acceptability in each group. Effective brief interventions that can be delivered in family practice are available for each of the risk factor areas.17–21 Before the CHAT is used and evaluated in the Canadian context, a study of the feasibility and acceptability of the CHAT content and process is required. The aim of this study was to assess the feasibility and acceptability of the CHAT, a brief validated lifestyle screening tool that can be administered in Canadian family practice waiting rooms. This paper presents the findings from this feasibility study.
METHODS
Consecutive adult patients 19 years of age or older attending a family practice on the days of the study were invited to participate by a research assistant in the waiting room. Those who appeared obviously unwell as judged by any of the practice staff, or those unable to read or understand English or the contents of the study information were not invited. Those who had previously completed the CHAT were excluded. The study setting was 2 family practices in British Columbia. One practice is a university-affiliated practice providing care to patients of middle to high socioeconomic status in a teaching clinic environment with medical students, residents, and pharmacy students; the other is a block-funded inner-city health centre providing primary care for adults without medical coverage, many of whom suffer from mental health issues, addictions, or other chronic health problems. The study was carried out over 3 half-days and 3 full days at the first practice and over 2 full days at the second practice. Family physicians from the participating practices were also invited to provide feedback about the CHAT.
After providing informed consent, patients completed the CHAT in the waiting room, which took less than 5 minutes. The patient then brought the completed CHAT to the physician consultation. The physician had the opportunity to discuss the results with the patient and address any issues, if desired.
The measures of feasibility included the proportions of consecutive eligible patients who agreed to participate in the study and the questions completed. The rates of positive answers to each domain were also recorded. Acceptability of the CHAT to patients and physicians was assessed by the proportion of objections to questions in each domain and by open-ended questions on feedback forms. Feedback forms were filled out following completion of the CHAT form either before or after the physician visit.
Sample size calculations were not carried out, as this was a feasibility study; however, the investigators aimed to enrol 50 to 100 patients from each of the 2 practices. Numbers and percentages of each of the outcome measures and the open-ended question responses are presented.
The study was approved by the University of British Columbia Behavioural Research Ethics Board.
RESULTS
During the study period, 282 adults attended the practices; 265 (94%) patients were eligible to participate and 176 (66%) were enrolled (Figure 1). The CHAT was completed by 161 (91%) enrolled patients before their consultations after they provided informed consent. Of those, 107 (66%) also completed the acceptability feedback form. Eight physicians were involved. There were also several residents in the academic practice, but they did not participate in the feedback.
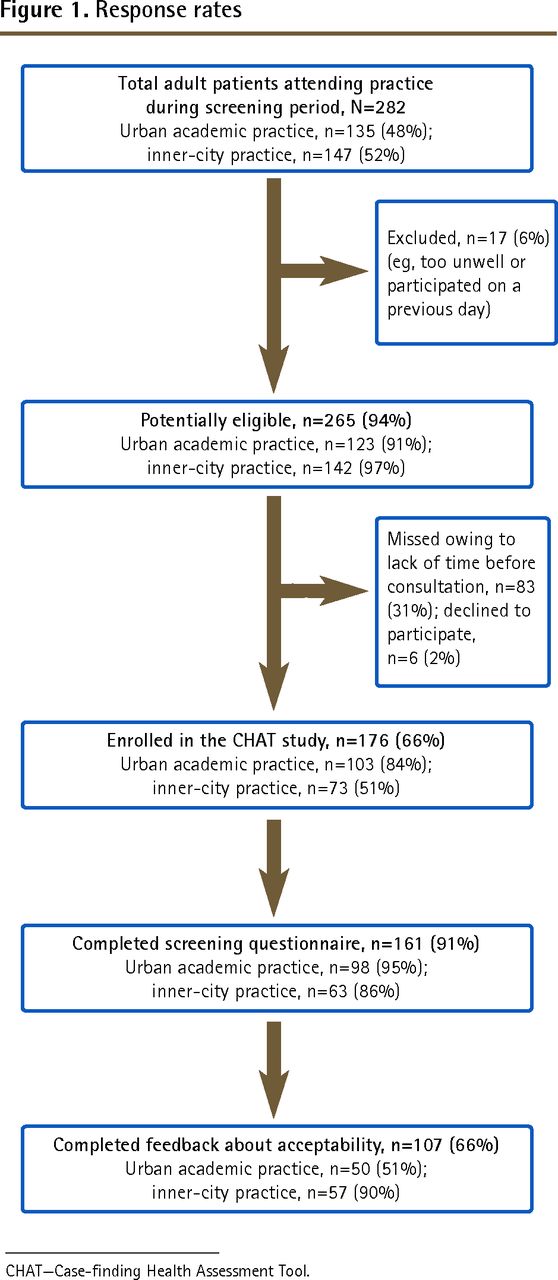
Response rates
CHAT—Case-finding Health Assessment Tool.
The rates of positive responses to questions about mental health and lifestyle risk were very different in the 2 practices (Table 1). Just 11% of the patients from the urban academic practice currently smoked, and only 1% reported ever having used nonprescription or recreational drugs. Corresponding rates in the inner-city community health centre were 71% and 48%, respectively. The identification of risk factors for depression and anxiety was high in both practices, with 60 of 161 (37%) answering yes to both depression screening questions and 42 of 161 (26%) requesting help for this. Overall, 9% (14 of 161) reported that there was someone in their lives they were afraid of; who wanted to hurt them; or who controlled them, preventing them from doing what they wanted. Only 2% reported problematic gambling. Table 2 presents the aspects of patients’ lives that caused them stress, with money and health being the most common stressors. There were high rates of some risk factors, and a number of people indicated that they would like help (Table 3). The highest rates for requesting assistance were for smoking (20%), depression (26%), and anxiety (25%). Overall, 77 patients (48%) reported that they wanted help with at least 1 risk factor; however, only 57 individuals (35%) wanted help that day.
Positive responses to mental health and lifestyle screening questions of consecutive adult patients attending 2 family practices in British Columbia
Responses to the question about life stress
Screened patients requesting assistance with identified risk factors
Of the 107 patients who completed the feedback form about the CHAT, 2 people (2%) objected to the alcohol questions. There were no objections identified to any other questions. Fifty-two participants (49%) wrote comments in response to the question, “What (if anything) did you like about the assessment form?” Participants commented that they thought the CHAT questions were simple, clear, thorough, relevant, and important; raised awareness of the issues; and showed concern. Seventeen participants wrote comments about what they did not like about it. Some thought the questions were too general; lacked flow; were not long enough; or should include other options such as sometimes, whether the issue was already being addressed, or room for comments. Some patients found the questions difficult to read and required their reading glasses. One respondent commented that the CHAT raised hopes of actually getting help. Another was concerned that his or her feelings of depression might have been an appropriate response rather than a “mental problem,” and one other thought the number of prescription drugs was also an issue that the CHAT should explore. Some thought that not much could be done about tobacco cessation or wanted more specific questions about the number of cigarettes smoked.
Eight physicians completed a feedback form about the CHAT, 7 of whom made positive comments. They liked that it facilitated discussion about potentially sensitive issues that otherwise might not have been talked about, and that patients had the option of “naming” an issue but indicating that they did not wish to discuss it now. Five made comments about possible disadvantages or suggestions for improvement, such as adding a place for the date, other screening tools, or the option being addressed for each issue. One thought it would not be useful for follow-up and another thought it too simple. The physicians did not think that patients would object to any questions. All physician respondents stated that they would use such a form, if available. Three thought they would screen all adult patients, one would use it opportunistically, and 4 said they would use another approach, such as targeted administration to new patients.
DISCUSSION
This study showed that it was feasible to screen for several mental health and lifestyle risk factors in the waiting room of 2 family physician practices with different patient profiles. There were high rates of adult patients at risk of depression and high rates of other risk factors identified, such as smoking, exessive alcohol consumption, and gambling, particularly in the inner-city practice; however, overall rates were similar to those found in previous studies in New Zealand.12 The study also found that a portion of the patients with such risk factors were ready to make a behavioural change and indicated that they wanted help that day.
Overall there were 102 risk factors self-identified for which patients requested “help today” during 161 consultations (38 issues at 98 consultations in the urban academic practice and 64 issues at 63 consultations in the inner-city practice). If many of these issues were over and above the reason for the consultation, this might present an extra demand on time, either of the physician or of other health care providers. Even if patients were not ready to address the issues, the form provided information about risk factors that could be addressed sometime in the future. This information would also provide statistics about the practice prevalence of these risk factors if the CHAT form were used on all or randomly selected adult patients from the practice.
The CHAT was also found to be acceptable, with few objections to any of the questions. Participants liked the brevity and practicality of the CHAT and appreciated that the medical professionals cared. Participant comments suggested that the form also acted to increase awareness of the issues and provided an impetus for self-reflection, which in itself might represent an intervention. However, it is important to acknowledge the expectations of patients; as one patient stated, the CHAT might “rais[e] hopes on actually getting help.”
The physicians found the CHAT useful in bringing relevant issues forward and commented that it would be particularly useful for new patients. One physician suggested the addition of another screening tool for abuse.
Compared with the literature
The questions in the CHAT have been validated in consecutive patients.22 The 2 depression questions in the CHAT have 96% sensitivity and 69% specificity22 for diagnosing major depression, and 73% sensitivity and 98% specificity23 for those who also request help. Rates were similar for the anxiety screening question.22,23 Therefore, the rates of 26% and 25% of patients who requested help for depression and anxiety, respectively, in this study are consistent with the estimated prevalence of mental health conditions, such as depression and anxiety, seen both in the Canadian population24 and among those visiting their family physicians.3
It has become increasingly clear in recent years that addiction and mental health disorders often coexist,25 and there has been a move from single-condition instruments toward screening tools that assess several mental health issues such as depression, anxiety, and somatisation26; generalized distress27; serious mental illness28; and mental illness and trauma.29,30 However, none of the other multi-item instruments is a generic primary care tool offering casefinding for both lifestyle factors and mental health issues. They deal with specific conditions such as substance abuse or mental distress, disease states like cancer or heart disease, or populations such as adolescents, the elderly, or pregnant women.
An electronic version of the CHAT, completed on tablet computers in waiting rooms, with results transmitted into the electronic medical records of family physicians at the point of care, has also been developed and is being trialed in New Zealand.31–33 It incorporates a tree structure with added scored tools triggered where applicable: the Alcohol, Smoking and Substance Involvement Screening Test for smoking, alcohol, and other drug use34; the Patient Health Questionnaire module for depression35; and the Generalized Anxiety Disorder Assessment for anxiety.36 It also incorporates 3 Alcohol Use Disorders Identification Test Consumption questions on alcohol.37 For positive domains, the physician has electronic access to stepped-care clinical decision- support tools to guide decision making, including problem solving, goal setting, brief coaching, patient education, medications, and referrals.
Strengths and limitations
The main reason for non-participation was that patients were missed owing to a lack of time before the physician consultation. However, the exclusion of non-English-speaking patients, who might also be immigrants and have lower socioeconomic status, might have introduced a systematic bias. When used in practice, the screening tool alone would take less time without the study procedures, so a greater coverage is likely. In addition, the CHAT can be used annually, just for new patients, or only in those considered to be high risk, depending on the preference and profile of the practice. Of interest, there were few patients in either practice who declined to participate.
The study was a feasibility study within only 2 practices; thus “prevalence rates” of each risk factor are only relevant for the practices themselves and will not be representative of actual rates across family physician practices.
Conclusion
Mental health and lifestyle risk factors are often not detected or addressed during physician visits owing to time constraints.2 The CHAT allowed efficient identification of 9 risk factors, as well as identification of those wanting help, and could be used in waiting rooms to screen all or targeted adult Canadian primary care patients (eg, patients new to the practice; those not seen for 2 years; antenatal patients; or those with pre-existing, long-term conditions, mental health issues, or substance misuse). The tool allows patients to prioritize the areas that they would like addressed and facilitates a conversation with their physicians for shared decision making.32 Repeating the CHAT at a later date allows ease of tracking of patients’ progress over time.
In addition to time constraints, mental health and lifestyle risk factors are also often not detected either because patients do not know that these are concerns to bring to their physicians or because they might feel threatened if they are asked directly. Because sensitive questions are embedded in the CHAT, it increases the acceptability of such questions to patients. Physicians are also cautious about stigmatizing patients by direct questioning, and the CHAT brings the issues into the open and initiates the patient-physician conversation, reducing barriers for patients to seek and accept help.
Notes
EDITOR’S KEY POINTS
Mental health and lifestyle risk factors are often not detected or addressed owing to time constraints. This study aimed to assess the feasibility and acceptability of administering the validated Case-finding Health Assessment Tool (CHAT) in Canadian family practice. The CHAT is a short, self-administered tool for lifestyle and mental health assessment of adult patients, which can be completed in the waiting room before the physician appointment.
The CHAT allowed efficient identification of 9 risk factors, as well as identification of those wanting help. High rates of several of the risk factors were identified, and about a third of the patients with such risk factors were ready to make behavioural changes and indicated that they wanted help that day.
The CHAT was also found to be acceptable, with few objections to any of the questions. Participants liked the brevity and practicality of the CHAT and appreciated that the medical professionals cared. Participant comments suggested that the form also acted to increase awareness of the issues and provided an impetus for self-reflection.
POINTS DE REPÈRE DU RÉDACTEUR
Souvent, les facteurs de risque liés à la santé mentale et au mode de vie ne sont pas détectés ou pris en charge en raison des contraintes de temps. Cette étude voulait vérifier s’il était faisable et acceptable d’utiliser un outil déjà validé, le Case-finding Health Assessment Tool (CHAT) dans un contexte de médecine familiale au Canada. Le CHAT est un outil court et auto-administré qui vise à évaluer le style de vie et la santé mentale de patients adultes et qui peut être complété en salle d’attente avant la rencontre avec le médecin.
Le CHAT a permis d’identifier de façon efficace 9 facteurs de risque, mais aussi d’identifier les patients recherchant de l’aide. Des taux élevés ont été observés pour plusieurs des facteurs de risque et environ un tiers des patients qui présentaient de tels facteurs étaient disposés à modifier leur comportement et indiquaient qu’ils voulaient de l’aide ce jour-là.
Le CHAT était jugé acceptable, avec seulement quelques objections à une question. Les participants ont apprécié le fait que le CHAT était court et pratique et que les professionnels de la santé se préoccupaient d’eux. Les commentaires des participants suggéraient que cet outil avait pour effet de les rendre plus conscients de leurs problèmes et constituait un incitatif à l’autoréflexion.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
All authors contributed to the concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}