


Abstract
Objective To explore the perspectives of patients who live with multiple chronic conditions as they relate to the challenges of self-management.
Data sources On September 30, 2013, we searched MEDLINE, EMBASE, and CINAHL using relevant key words including chronic disease, comorbidity, multimorbidity, multiple chronic conditions, self-care, self-management, perspective, and perception.
Study selection Three reviewers assessed and extracted the data from the included studies after study quality was rated. Qualitative thematic synthesis method was then used to identify common themes. Twenty-three articles met the inclusion criteria, with most coming from the United States.
Synthesis Important themes raised by people living with multiple chronic conditions related to their ability to self-manage included living with undesirable physical and emotional symptoms, with pain and depression highlighted. Issues with conflicting knowledge, access to care, and communication with health care providers were raised. The use of cognitive strategies, including reframing, prioritizing, and changing beliefs, was reported to improve people’s ability to self-manage their multiple chronic conditions.
Conclusion This study provides a unique view into patients’ perspectives of living with multiple chronic conditions, which are clearly linked to common functional challenges as opposed to specific diseases. Future policy and programming in self-management support should be better aligned with patients’ perspectives on living with multiple chronic conditions. This might be achieved by ensuring a more patient-centred approach is adopted by providers and health service organizations.
Multimorbidity, or having multiple chronic conditions, is defined as the simultaneous occurrence of 2 or more diseases or medical conditions in one person.1 The burden of multiple chronic conditions in aging populations is rapidly increasing.2–4 The health outcomes are worse for such patients, with lower self-reported health, higher rates of health care visits, and higher risk of medication issues.5
The importance of supporting self-management for people with multiple chronic conditions is being increasingly recognized as a key component of improving the overall health of this population.6–10 Self-management relates to “the tasks that individuals must undertake to live well with one or more chronic conditions.”11 Self-management support uses collaborative goal setting and self-efficacy strategies to enable patients to carry out normal roles and activities and better manage the medical and emotional effects of their illnesses in partnership with health care providers.6 Self-management support interventions vary and can include such components as group meetings, motivational counseling, case management, patient education, and follow-up.
Multiple studies have evaluated the effectiveness of programs designed to support self-management in patients with chronic diseases. These studies often use quantitative methods and focus on clinical outcomes.12–15 However, issues related to self-management of chronic conditions should be examined not only from the perspective of providers and the health care system itself, but also from the perspective of patients.16,17 To our knowledge, there are no qualitative reviews that address self-management of multiple chronic conditions from patients’ perspectives.
Thus, the purpose of this paper is to gain a greater understanding of patients’ perspectives on living with multiple chronic conditions, specifically related to the barriers to self-management and subsequently any strategies adopted by people living with multiple chronic conditions. The results of this review should help inform both governments and the medical community to develop policy and programming in self-management support that are aligned with patients’ perspectives on living with multiple chronic conditions.
DATA SOURCES
We chose to examine the qualitative literature, as this type of research is most likely to provide patients’ perspectives with “conceptual depth about the patient experience.”18 Conversely, the quantitative literature on self-management focused largely on the effectiveness of various programs designed to promote self-management. There were several stages to the review, including development of the search strategy, application of inclusion and exclusion criteria, quality appraisal, and synthesis of the findings.
On September 30, 2013, we searched MEDLINE (In-Process and Other Non-Indexed Citations, and 1948 to present), EMBASE (Classic and 1947 to present), and CINAHL (1981 to present) using relevant key words including chronic disease, comorbidity, multimorbidity, multiple chronic conditions, self-care, self-management, perspective, and perception. In addition, we did a hand search of references and searched the International Research Community on Multimorbidity website.19
STUDY SELECTION
Quality rating was done based on the Critical Appraisal Skills Programme, an accepted rating tool for qualitative research.20 The Critical Appraisal Skills Programme provides researchers with checklists designed to appraise study quality. Articles with 1 or more unacceptable items and articles with more than 4 inadequate items were rated as poor quality and excluded.
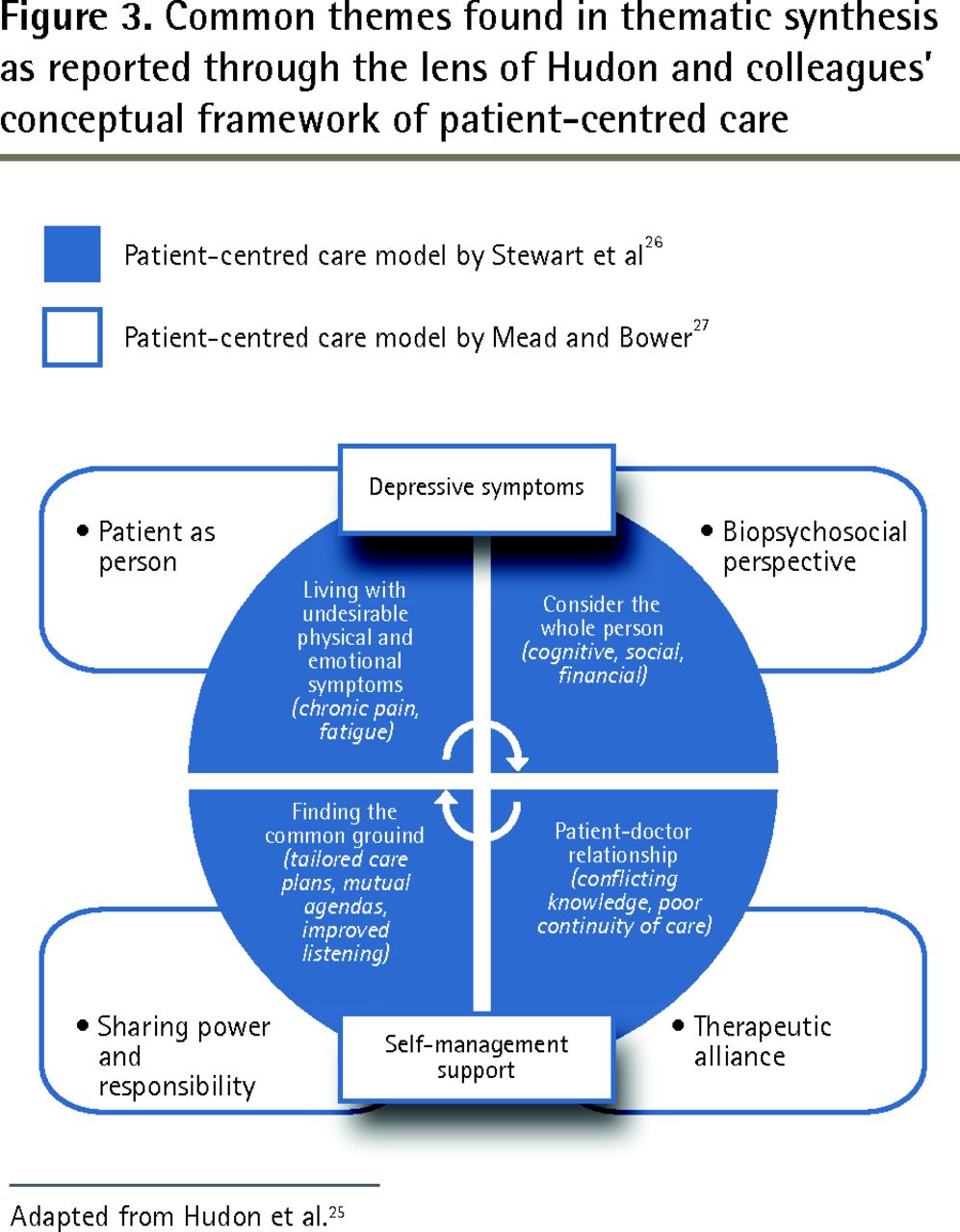
A thematic synthesis method was used to analyze the articles.21,22 Three researchers independently read and open-coded relevant sections of each article, looking for barriers and strategies identified by patients. Using these codes, descriptive themes were constructed, followed by the development of analytic themes.23 While researchers were familiar with the published literature in the field, they did not start the analysis with explicit potential factors and themes in mind; rather, they identified the emergent themes from the articles.24 The research team regularly met during the analysis to discuss the themes, cross-check evidence back to the original studies, and identify any disconfirming evidence. As a final step, we applied Hudon and colleagues’ conceptual framework of patient-centred care25 as an explanatory framework for the important themes. It is based on the model of patient-centred care by Stewart et al26 and is integrated with a conceptual model of the doctor-patient relationship by Mead and Bower.27 Hudon et al created this framework for their systematic review of tools to measure patients’ perceptions of patient-centred care. The framework identifies 4 dimensions of patient-centred care grounded in aspects of the doctor-patient relationship: the patient as a person (disease and illness experience); the biopsychosocial perspective (whole person); the therapeutic alliance (patient-doctor relationship); and sharing power and responsibility (common ground).25
SYNTHESIS
We found 256 records using the search strategy, and 7 additional articles were included from hand searching references. Once duplicate removal, relevance screening, and quality appraisal were done, a final 23 articles were included in our synthesis (Figure 1).

Flow diagram: Articles retrieved through search up to September 30, 2013.
All included studies contained qualitative data. Most were recently published (range 2003 to 2011) and conducted in the United States, with the remainder from Australia and the United Kingdom (Table 1).7,8,28–48
Characteristics of publication examining the perspectives of patients living with multiple chronic conditions
The common themes that emerged through our review can be viewed through the lens of the conceptual framework for patient-centred care described above. Figure 2 provides a visual depiction of Hudon and colleagues’ framework and Figure 3 illustrates the framework overlaid with our findings.25–27 Our findings are reported below, using the 4 dimensions outlined by Hudon and colleagues’ framework (patient as person, biopsychosocial perspective, therapeutic alliance, and sharing power and responsibility) as a guide.

Hudon and colleagues’ conceptual framework of patient-centred care
Data from Hudon et al.25
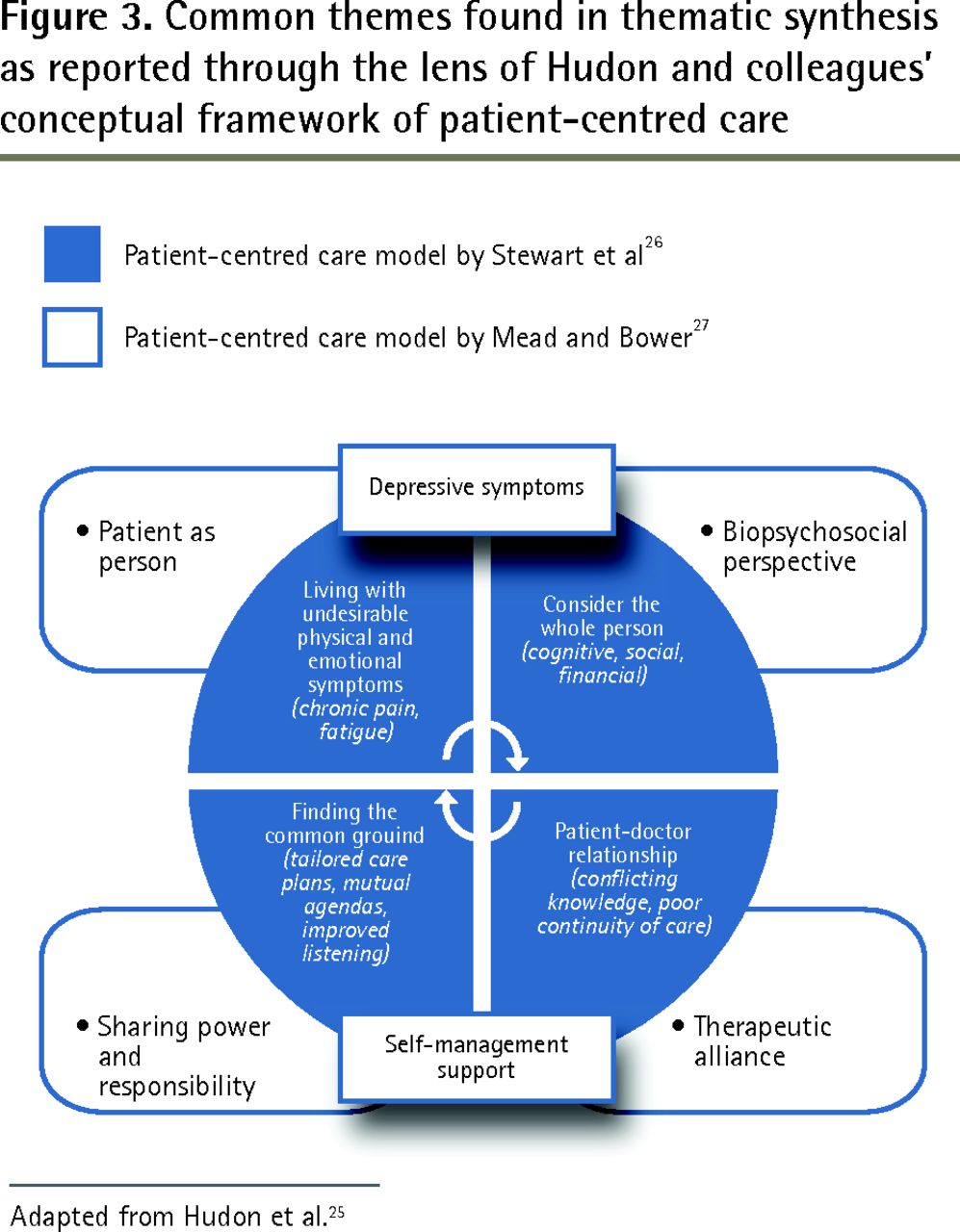
Common themes found in thematic synthesis as reported through the lens of Hudon and colleagues’ conceptual framework of patient-centred care
Adapted from Hudon et al.25
Patient as person
Our main findings pertaining to the patient-as-person dimension involved the experience of disease and illness.
People with multiple chronic conditions experienced a great deal of suffering from physical and emotional symptoms (eg, depression). Undesirable physical and emotional symptoms and impaired physical functioning can directly prevent patients from carrying out normal daily activities, including tasks required to appropriately and successfully self-manage.28–30 In people with multiple chronic conditions, physical and emotional symptoms can compound and build off of each other, resulting in a larger negative effect on their daily lives.28,30–32 These symptoms are interdependent and symptoms of one condition can be aggravated by the symptoms, treatment, or medications of another condition. Some symptoms might overshadow others and reduce the patient’s ability to manage his or her care.7 For example, many patients reported that their pain8,28–30,32–37 was one of the biggest factors limiting their ability to self-manage effectively.
Depression featured prominently for people with multiple chronic conditions.8,28,31,32,37–44 Many felt emotionally unstable; lacked motivation or self-discipline8,28; or experienced anxiety, sleep disturbances, lack of energy, worry, fear of activity,28,30 and fear for personal health31,32,37,42,44 and of death.28,30,38,39,45
Biopsychosocial perspective
Three key themes emerged related to the biopsychosocial perspective: the effect of cognitive approaches, the complexity of social support, and lack of financial resources.
Effect of cognitive approaches
For many patients, changing their cognitive approach to their illness was the best way to deal with their physical and emotional symptoms and limitations.41,44,46 Multiple cognitive strategies were raised including prioritizing conditions,34,39 reframing and regulating the amount of attention given to their situation,30 dealing with it, engaging in life and body listening,40 relinquishing control to another source (eg, doctor, God),46 and changing their beliefs (eg, assigning new meanings to daily chores or activities).30 Living with multiple chronic conditions became a way of life for people, who reported fluctuating between “living a life and living an illness.”44
Despite some people reporting being overwhelmed at times, many more seemed resilient and determined to persevere in spite of their challenges.8,43 In some cases, the more conditions someone had, the better they considered themselves at self-management because they already had developed skills such as self-monitoring and self-advocacy,40 or they became more motivated because of the heightened risk.30,46 Additional conditions were more readily accommodated if people established a cognitive link between existing management practices.40,41
Complexity of social support
Lack of social support was described as a barrier.7,28,30,32,33,37,43,46,47 Having appropriate social support, or at least knowing you could have it if you needed it, was very often referred to as a strong enabler to successful self-management.28,30,43,44 However, social support was also seen as a barrier to self-management when family or friends interfered with treatment plans or independence. Sometimes the intended support and help that family and friends tried to provide hindered patients’ ability to self-manage or feel confident in managing their conditions.30,33,47
Lack of financial resources
Lack of insurance for care, including the need to pay for medications and associated financial strain of expensive medications, was reported by patients.29–32,34,38,46,47 Additionally, the physical symptoms and frequent medical appointments associated with multiple chronic conditions might reduce employees’ productive time,40,45 occasionally leading to short- or long-term unemployment.45
Therapeutic alliance
Our main theme pertaining to therapeutic alliance was that the doctor-patient relationship was not always therapeutic. Patients cited contradictory knowledge, poor access, and challenges with medication as barriers to care.
Contradictory knowledge
Patients wanted to be knowledgeable enough about their situation to be able to look out for themselves,33,35,40 to be able to prioritize their conditions,34 and to be more informed, assertive, and self-reliant when interacting with their providers.32 However, many reported confusion and contradictory information about conditions,41 as multiple information sources exist.35,38,39 When consulting various providers, patients often received conflicting instructions about their individual needs, priorities, and management strategies.30,32,34,35,39,41,42
Poor access
People with multiple chronic conditions seemed to emphasize their medical needs, resulting in a greater reliance on health care providers,33 but convenient access to providers was often limited and no one was readily available to answer or clarify small questions as well as urgent concerns.29,32,38 In addition, where access was available, more frequent encounters with health care providers were reported as a barrier.7,28,38 Patients believed that they were not listened to when they raised concerns,32,38 and that providers were nonsupportive and often disagreed on priorities.32,39
Challenges with medication
Problems related to medications were specifically highlighted as a barrier to self-management.7,30,32 Patients understood the importance of using medications correctly but lacked the skill to address issues related to side effects, coordination of medication, and overreliance on medications.8,28,31 A troubled emotional state and anxiety (a prominent symptom) were also found to alter patients’ ability to understand and receive information, which can lead to medication noncompliance.31,42,48
Sharing power and responsibility
The key theme that emerged relating to sharing power and responsibility was the importance of finding common ground between patients and providers.
Several factors were identified by patients to assist in overcoming the barriers associated with the doctor-patient relationship such as being able to ask doctors questions and seek answers to their health concerns.33 Patients wanted to be listened to and have their individual, fluctuating needs appreciated.29 Tailored, written information and care plans that are mutually agreed upon and respect for the patient’s priorities and agendas were specifically identified as helpful.38,46 Written information should be kept simple.48 Individualized, integrated care plans should be explained to clarify and address potentially conflicting treatment strategies.29,35
People also wanted to be assisted with locating resources.48 In particular, better access to mental health care resources and the close monitoring of patients’ emotional states by their physicians were seen as helpful.28,31,39,46
DISCUSSION
In our systematic review of the qualitative literature examining patients’ perspectives of living with multiple chronic conditions, we found that patients were able to clearly identify challenges associated with self-management and develop strategies to address these factors. The barriers to self-management are many and yet common among people with many different diseases. However, while most studies were disease-specific, we found that discussion among patients that related to specific medical conditions and disease-specific symptoms was strikingly absent. People did not complain about lack of skill to manage medical tasks such as injecting insulin or blood pressure monitoring; rather, they reported difficulties in dealing with physical and emotional symptoms, with depression, pain, and fatigue being prominent. In addition, issues related to knowledge about self-management of conditions commonly arose because of confusing and often contradictory information provided by multiple health care providers.
Yet medical task management and patient education remain the focus of the medical community, with much of the programming targeted toward disease groups and optimizing care for target control of a specific condition (eg, hemoglobin A1c for people with diabetes).8,49,50 Thus, there is a need to support more programming such as the group generic Chronic Disease Self-Management Program,51 which remains the most widely adopted self-management support program internationally. The generic approach highlights active goal setting, problem solving, adoption of healthy lifestyles, navigating the medical system including communication with providers, and medication management within the context of general symptoms, such as pain, fatigue, and stress. It aligns very well with the body of literature relating to the experiences of people living with multiple chronic conditions.
The effects of multiple chronic conditions on a person are not always linear. Multimorbidity might have a dual role in self-management support. While most studies suggest that the coexistence of medical conditions might lead to inadequate self-management, some have found that multimorbidity improves patients’ self-management.52,53 Patients often have to prioritize conditions or reconcile their physicians’ advice.34,39,42 These “coping” mechanisms are the result of the lived experiences of being a person with multiple chronic conditions.6 The use of cognitive techniques such as diversion, normalizing, and changing beliefs was commonly reported by patients. It is possible that repeated poor health and increasing suffering create a tipping point for patients, whereby they are able to take charge of their health more effectively, despite having multiple chronic conditions.43,49,54
Policy and practice implementations
Our findings aligned well with Hudon and colleagues’ conceptual framework for patient-centred care25 and highlighted the importance of patient-centred care for people with multiple chronic conditions, which requires a “willingness to become involved in the full range of difficulties patients bring to their doctors, and not just their biomedical problems.”26 Viewing the patient as a whole person and trying to see the world through their eyes55 is essential when establishing a therapeutic alliance with people who live with multiple chronic conditions. This whole-person approach is supported by recent work by Smith et al who, in a review of interventions for managing patients with multimorbidity, found that programs targeting specific areas of concern, such as functional difficulties, were more effective than other programs.50
Primary care providers can play a foundational role in supporting patient self-management, especially for people with multiple chronic conditions, as 95% of Canadians with a chronic illness report having access to a regular family physician.56
However, finding common ground and sharing power and responsibility requires a fundamental shift of the patient-caregiver relationship into a collaborative partnership to support the patient.57 Providers need to be ready to support patients when they need it. There has been much emphasis on the implementation of the chronic care model leading to the activated patient. However, unless providers within the system are also at that stage of readiness, their efforts will fall short.53,58
In our review, beyond the cognitive strategies identified by patients, better communication and continuity were requested by the patients, with acknowledgment of the patient’s experience, including knowledge.29,38,41,48 Improved care coordination such that each provider in the circle of care works collaboratively and in an integrated manner with minimal conflicting recommendations is needed. Establishing continuity of relationships with physicians and regular visits to patients’ primary care physicians are essential components in avoiding re-education of providers on patients’ complex care needs.25,37,43 The movement to create a patient-centred medical home (PCMH) in primary care should support these efforts.59 The PCMH model helps reorganize the care practices provide, focusing specifically on team care, care coordination, access, and a systems-based approach supported by health information technology. Although the PCMH is an emerging model, it is closely linked with the chronic care model approach and is grounded in a patient-centred orientation that also highlights self-care, active decision making, care plans, and good communication—all themes identified in our review and key elements of self-management support.29,41,46 In addition to implementing the PCMH model, many regions are actively striving to improve coordination of care for high-needs patients such as seniors and people with chronic diseases. For instance, the Ontario government has already taken steps to support this approach through the establishment of community health links.60
Limitations
Our focus on the qualitative literature enabled us to capture papers that reported in depth on patient perspectives of living with multiple chronic conditions. The synthesis methods for qualitative literature are still under development and there are limited formal guidelines available,22 so where possible we built our approach based on other published qualitative reviews. We might have missed other relevant papers owing to lack of validation of the terms related to multimorbidity, and by excluding the quantitative research in this area as well as limiting included publications to the English language only.
Most of the included studies are from the United States and this limits the generalizability of the findings, especially related to financial aspects, although employment-related challenges due to frequent medical appointments would be relevant in other countries and are not only related to the health system. There was a higher proportion of women (56%) across most of the included studies and this might be because women are more likely to report multiple conditions.61
Finally, several important variables that might have contributed to the ability of patients to self-manage were not always reported by the research studies. These included social determinants of health such as socioeconomic status, educational level, disease duration, and patient self-efficacy. A small body of quantitative research has found that social disadvantage and lower levels of education are associated with a reduced likelihood of patients engaging in self-management.62,63 However, qualitative research examining these variables from patients’ perspectives would be valuable, and additional research should be conducted to further explore the effects of social determinants of health on self-management.
Conclusion
There are many complexities to the delivery of care for people with multiple chronic conditions. The burden of suffering is great, as is the increasing burden to the health care system and society as a whole. This review provides a unique view into patients’ perspectives of living with multiple chronic conditions, which are clearly linked to functional challenges and are not disease specific. Future policy and programming in self-management support should be better aligned with patients’ perspectives of living with multiple chronic conditions and this might be achieved by ensuring a more patient-centred approach is adopted by providers and health service organizations.
Notes
EDITOR’S KEY POINTS
This review provides a unique view into patients’ perspectives of living with multiple chronic conditions, which are clearly linked to functional challenges and are not disease specific.
Patients were able to clearly identify challenges associated with self-management and develop strategies to address these factors.
People did not complain about lack of skill to manage medical tasks such as injecting insulin or blood pressure monitoring; rather, they reported difficulties in dealing with physical and emotional symptoms, with depression, pain, and fatigue being prominent. Issues related to knowledge about self-management of conditions commonly arose because of confusing and often contradictory information provided by multiple health care providers.
POINTS DE REPÈRE DU RÉDACTEUR
Cette revue est une occasion unique de savoir ce que les personnes souffrant de plusieurs maladies chroniques rencontrent comme défis, lesquels sont clairement reliés à des difficultés fonctionnelles et non à des maladies particulières.
Les patients pouvaient facilement identifier les problèmes liés à l’autogestion de leur santé et développer des stratégies pour y faire face.
Les patients ne se plaignaient pas d’un manque de compétences pour des tâches médicales, comme les injections d’insuline ou la mesure de la tension artérielle; ils mentionnaient plutôt avoir des difficultés à gérer certains symptômes physiques ou psychologiques, tels que la dépression, la douleur et la fatigue, qui constituent des problèmes particulièrement importants en rapport avec l’autogestion de leur condition à cause des renseignements confus et souvent contradictoires qu’ils reçoivent des nombreux soignants.
Footnotes
Contributors
All authors participated in the planning, execution, or analysis of this study. All authors have read and approved the final submitted version.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Drivers and barriers to promoting self-care in individuals living with multimorbidity: a cross-sectional online survey of health and care professionals
- Factors influencing the integration of self-management in daily life routines in chronic conditions: a scoping review of qualitative evidence
- Systematic review on the instruments used for measuring the association of the level of multimorbidity and clinically important outcomes
- Guideline deviation and its association with specific chronic diseases among patients with multimorbidity: a cross-sectional cohort study in a care management setting
- Protocol for development, calibration and validation of the Patient-Reported Inventory of Self-Management of Chronic Conditions (PRISM-CC)
- Prevalence of secondary care multimorbidity in mid-life and its association with premature mortality in a large longitudinal cohort study
- Facilitators and barriers to the self-management of COPD: a qualitative study from rural Nepal
- Relationship between life satisfaction and preventable hospitalisations: a population-based cohort study in Ontario, Canada
- Prevalence of anxiety and depressive symptoms and their association with multimorbidity and demographic factors: a community-based, cross-sectional survey in Karachi, Pakistan
- Preparing Chinese patients with comorbid heart disease and diabetes for home management: a mixed methods study
- Connecting People With Multimorbidity to Interprofessional Teams Using Telemedicine
- Combined impacts of multimorbidity and mental disorders on frequent emergency department visits: a retrospective cohort study in Quebec, Canada
- Characteristics of self-management among patients with complex health needs: a thematic analysis review
- Underlying mechanisms of complex interventions addressing the care of older adults with multimorbidity: a realist review
- Experiences of community-dwelling older adults living with multiple chronic conditions: a qualitative study
- Impact of educational attainment on the association between social class at birth and multimorbidity in middle age in the Aberdeen Children of the 1950s cohort study
- Patient work from a context and time use perspective: a mixed-methods study protocol
- Self-Care for the Prevention and Management of Cardiovascular Disease and Stroke: A Scientific Statement for Healthcare Professionals From the American Heart Association
- Older Patients Perspectives on Managing Complexity in CKD Self-Management