


Sarcoidosis is a granulomatous multisystem disease of unclear pathogenesis that can affect any organ.1 The cutaneous manifestations are present in 20% to 35% of patients. Skin lesions are classified as specific or nonspecific depending on the presence of noncaseating granulomas on histologic studies. Specific lesions include maculopapules, plaques, nodules, lupus pernio, scar infiltration, alopecia, ulcerative lesions, and hypopigmentation, among other types of lesions. The most common nonspecific lesion is erythema nodosum. Other infrequent cutaneous manifestations include calcifications, prurigo, erythema multiforme, nail clubbing, and acute febrile neutrophilic dermatosis.2 We report a case of chronic urticaria of unknown cause that, after 6 months of treatment with antihistamines, displayed symptoms consistent with respiratory disease associated with systemic involvement.
Case
A 34-year-old man was followed in our department for chronic urticaria that responded poorly to 6 months of antihistamine treatment (Figure 1). During the last 2 months of antihistamine treatment, the patient had nonspecific constitutional symptoms including fever, weight loss, fatigue, dyspnea, and dry cough. Skin-prick tests were done with standard aeroallergens and foods. Laboratory tests (including measurement of angiotensin-converting enzyme [ACE] level), lung function studies, a tuberculin test, a chest x-ray scan, a computed tomography scan, and a lung biopsy were performed.
Skin-prick tests were performed using the most common aeroallergens in our epidemiologic area, including molds (Alternaria, Aspergillus, Cladosporium, and Penicillium spp); negative results were obtained for all tests. The tuberculin test also had a negative result. Lung function tests revealed a mixed disease process with no response to a bronchodilator and a moderate decline in diffusing capacity. Chest x-ray and thoracic computed tomography scans showed mediastinal and hilar lymphadenopathy, as well as diffuse and bilateral reticulonodular infiltration (Figure 2). A trans-bronchial lung biopsy revealed noncaseating granulomas. Bacterial and mycobacterial cultures had negative results. For the sputum tests, bacterial culture did not have any conclusive results, and potassium hydroxide fungal staining did not reveal any hyphae from filamentous fungi. Blood tests showed an ACE level of 141 μg/L.
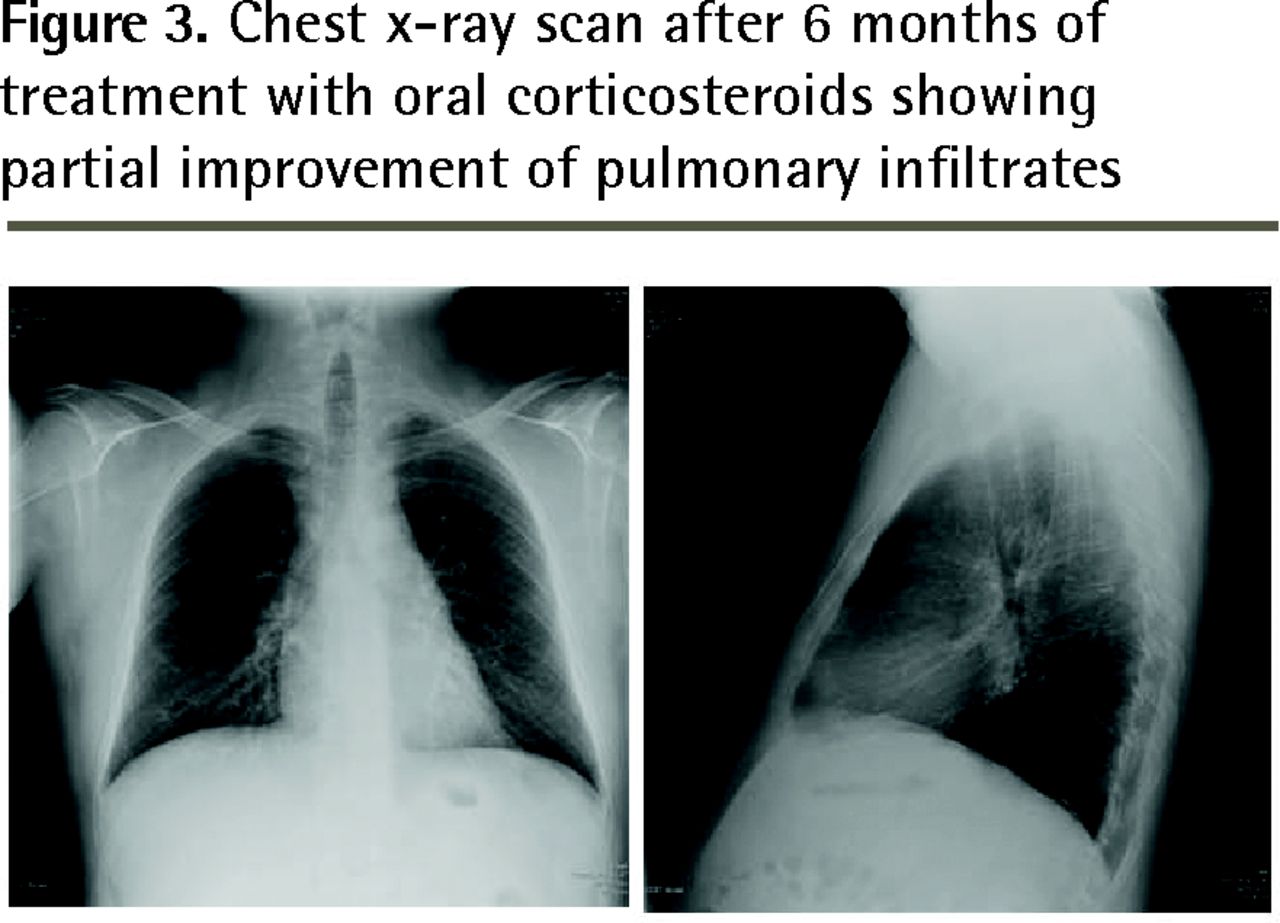
The changes in the lungs seen on the chest x-ray scan were consistent with stage 2 sarcoidosis. Figure 3 is a chest x-ray scan taken after 6 months of corticosteroid treatment; it shows partial improvement of the pulmonary infiltrates. After 12 months of tapered-dose treatment with oral corticosteroids, the patient had no cutaneous or respiratory symptoms, and had a normal ACE level. Of interest, 3 weeks after the end of corticosteroid treatment, the patient had increasing cough and intensification of dyspnea, which prompted re-admission to hospital owing to respiratory insufficiency and a diffuse nodular interstitial pattern on chest x-ray scan. His ACE level had increased 3-fold from the previous measurement, and cutaneous manifestations were absent.

Skin lesions and chest x-ray scan with negative results at first presentation with urticaria

Chest x-ray and computed tomography scans after 6 months of unsuccessful antihistamine treatment for urticaria: Scans show mediastinal and hilar lymphadenopathy, as well as diffuse and bilateral reticulonodular infiltration.

Chest x-ray scan after 6 months of treatment with oral corticosteroids showing partial improvement of pulmonary infiltrates
Discussion
We performed an extensive review of the literature by using the MeSH terms urticaria and sarcoidosis in PubMed and selecting articles from 1997 to 2011. Determining the pathogenesis of chronic urticaria represents a clinical challenge in most patients. Chronic urticaria can be the first manifestation of diverse systemic infectious and inflammatory diseases. Sarcoidosis is a granulomatous syndrome characterized by the presence of noncaseating granulomas. Its prevalence is estimated at 40 cases per 100 000 persons in Europe, with northern European countries reporting higher incidences of sarcoidosis than southern European countries. Skin manifestations of sarcoidosis are estimated to occur in approximately 25% of patients and show a variety of cutaneous signs.3 Maculopapules seem to be the type of lesion most closely related to acute sarcoidosis. In our experience, chronic urticaria is a rare manifestation of sarcoidosis. The prevalence of urticaria as an extrapulmonary form of sarcoidosis is unknown. Most patients with systemic diseases eventually develop cutaneous symptoms.4 Therefore, all patients with cutaneous noncaseating granulomas should be assessed for systemic sarcoidosis and reevaluated periodically. However, the decision to treat might be complicated given the unpredictable course of the disease, which shows spontaneous remission in up to two-thirds of patients. Systemic corticosteroids should be used as second-line agents when local therapy fails or is impractical. Data on the efficacy of systemic corticosteroids are scarce.5 Considering cutaneous sarcoidosis in the clinical differential diagnosis of urticaria requires physicians to associate urticaria with systemic involvement or extracutaneous single-organ involvement. The potential of histopathologic analysis of the skin to diagnose sarcoidosis might be studied in the future.
Conclusion
Sarcoidosis is a treatable disease that should be considered in the differential diagnosis of chronic urticaria. Patients should be reevaluated by their family physicians on a regular basis to discern exceptional causes of urticaria.
Acknowledgments
This work was partially supported by a grant from Comunidad de Madrid (S2010/BMD-2502 MITIC).
Notes
EDITOR’S KEY POINTS
-
Chronic urticaria can be the first manifestation of diverse systemic infectious and inflammatory diseases, including sarcoidosis.
-
Most patients with systemic diseases eventually develop cutaneous symptoms. Therefore, all patients with cutaneous noncaseating granulomas should be assessed for systemic sarcoidosis and reevaluated periodically.
-
The decision to treat sarcoidosis might be complicated given the unpredictable course of the disease, which shows spontaneous remission in up to two-thirds of patients. Systemic corticosteroids should be used as second-line agents in the treatment of sarcoidosis when local therapy fails or is impractical.
Footnotes
-
This article is eligible for Mainpro-M1 credits. To earn credits, go to www.cfp.ca and click on the Mainpro link.
-
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro de juin 2014 à la page e308.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.