


Article Figures & Data
Figures
- Figure 1
Cardiovascular Health Study data to determine hazard ratios for AF, by exercise levels: Circled data point indicates a statistically significant change from baseline.
AF–atrial fibrillation.
Data from Mozaffarian et al.35
- Figure 2
Physicians’ Health Study data to determine hazard ratios for AF, by PA per week: Circled data point indicates a statistically significant change from baseline.
AF–atrial fibrillation, PA–physical activity.
Data from Aizer et al.36
- Figure 3
National Walkers’ and Runners’ Health studies data to determine hazard ratios for arrhythmias: Circled data points indicate a statistically significant change from baseline.
Data from Williams and Franklin.41
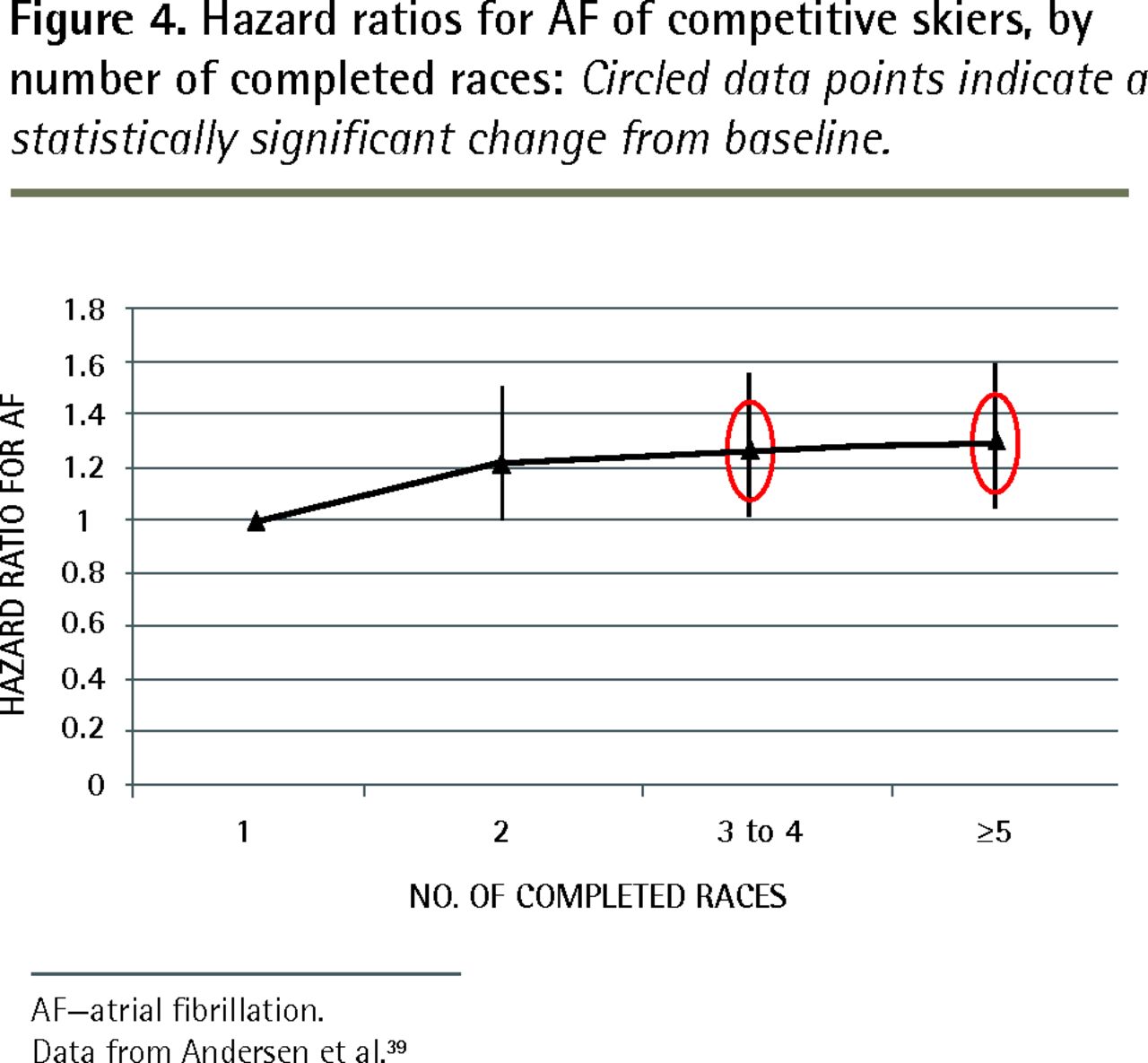
- Figure 4
Hazard ratios for AF of competitive skiers, by number of completed races: Circled data points indicate a statistically significant change from baseline.
AF–atrial fibrillation.
Data from Andersen et al.39
- Figure 5
Characteristics of endurance exercise speculated to promote AF
AF—atrial fibrillation.





Tables
STUDY STUDY CHARACTERISTICS MEAN AGE OF PARTICIPANTS, Y DEFINITION OF HIGH-INTENSITY EXERCISE AND END POINTS OUTCOMES LIMITATIONS RISK OF BIAS Karjalainen et al,31 1998 • Top-level veteran orienteers (ie, runners)
• 228 in orienteer group vs 212 in control group; 100% men
• 10-y follow-up47.5 • High position in veteran ranking is an indicator of y of intense training
• Lone AF• AF developed in 5.3% of orienteers vs 8.9% of control group (RR = 5.5; P = .012) • Men only
• Cohort information insuffcient
• No correction for confounding
• Unreliable outcome assessment
• Potential recall biasHigh Frost et al,32 2005 • Danish Diet, Cancer, and Health Study data
• 19–593 (51%) men and 18 807 women
• Mean 5.7-y follow-up56 • Heavy physical workload (self-report)
• AF or atrial futter• No differences between the sexes*
• No differences overall*• Few subjects exposed to heavy work or vigorous PA
• Relied on registry outcomes
• Could not separate AF from atrial futter
• Potential recall biasModerate Heidbuchel et al,33 2006 • 137 patients after ablation for atrial futter; 83% men
• 31 of the 137 patients regularly engaged in sports before ablation
• Mean 2.5-y follow-up58 • Intense competitive activity ≥ 3 h per wk
• Development of AF after ablation for atrial futter• AF development in high PA (HR = 1.81; P = .02)
• No differences between the sexes• Status after ablation not comparable
• Higher rate of cardiovascular disease
• Potential for recall bias
• No correction for confoundingModerate Molina et al,34 2008 • 252 Barcelona marathon runners vs 305 sedentary men; 100% men
• Retrospective cohort study
• Mean 11.6-y follow-up39 • Marathon running
• Lone AF• Endurance sport practice associated with higher risk of lone AF (HR = 8.80, 95% CI 1.26 to 61.29; P = .028)* • Men only
• Control group recruited from different population
• 5-y difference in follow-up duration
• Risk of recall bias
• All AF events not consideredModerate Mozaffarian et al,35 2008 • Cardiovascular Health Study Medicare eligibility lists in US communities
• 5446 participants; 42% men
• Post hoc analysis of RCT
• 12-y follow-up73 • ≥6 MET† of intensity
• ≥ 1840 kcal/wk (self-report)
• AF on annual examination or electrocardiogram• Graded reduction in AF with light to moderate PA intensity*
• No reduction in AF with high PA intensity(RR = 0.87, 95% CI 0.64 to 1.19)* • With an older cohort, there was less high-intensity PA
• No sex differences examinedLow Aizer et al,36 2009 • 16–921 men in Physicians’ Health Study
• Post hoc analysis of RCT
• 12-y follow-up51 • Suffcient to “work up a sweat” 5–7 d/ wk (self-report)
• AF• RR for 0 vs 5–7 d/wk (joggers) of vigorous exercise was 1.20 (95% CI 1.02 to 1.41; P = .04)*
• Elevated risk observed if aged < 50 y (RR = 1.74, 95% CI 1.23 to 2.47;
P < .01)• Men only
• Some retrospective subgroup analysis
• Association seen at 3-y evaluation but not at 9 yLow Pelliccia et al,37 2010 • 114 Olympic athletes vs 97 people in control group; 78% n
• 8.6-y follow-up22 • Participation in Olympic-endurance disciplines and having multiple games experience
• Cardiac symptoms or events• No cardiac events developed for more than 8 y
• Reduced incidence compared with general population• Very young study cohort
• Small group and therefore few potential outcomes
• Screening of multiple cardiovascular systems before enrolment
• Control group was very ft; had participated in 1 Olympic gameHigh Everett et al,38 2011 • 34 759 women who had been part of the Women’s Health Study
• 20-y follow-up57.5 • ≥ 6 MET† of intensity
• ≥ 15 MET† h/wk
• AF• No difference in incident of AF among quintiles after adjusting for hypertension and obesity* • Women only
• Very few women underwent strenuous activity
• Self-assessment of PA intensity
• Self-assessment of outcomesLow Andersen et al,39 2013 • 52 755 Swedish participants in a 90-km cross-country skiing event; 87% men
• Mean 9.7-y follow-up38.5 • Fast finishing time or high number of races completed
• AF or atrial flutter• Higher risk of AF among those who completed > 5 races (HR = 1.29, 95% CI 1.04 to 1.61) and among those who had the fastest relative fnishing times (HR = 1.20, 95% CI 0.93 to 1.55)* • Outcomes include AF or atrial futter
• Cohort was still extremely active and not representative of general populationLow Thelle et al,40 2013 • 309 540 Norwegians in a public health screening program; 48% men
• 4-y follow-up41.4 • Frequent hard training or competitive PA
• Flecainide prescription• Increase in AF in men with high intensity PA (HR = 3.14, 95% CI 2.17 to 4.54)* • High attrition rate over time
• Surrogate outcome (fecainide) for lone AF
• Self-assessment of PA intensity
• Risk of recall biasModerate Williams and Franklin,41 2013 • 46 807 participants in the National Runners’ and Walkers’ Health studies; 41% men
• Age range was 33–72 y
• 6.2-y follow-upNA • ≥ 6 MET† of intensity
• ≥ 5.4 MET† h/d
• Any cardiac arrhythmia• Arrhythmia risk declined by 4.8% each MET† h/d over baseline for runners and walkers*
• Beneft was higher for those aged < 50 y• Self-report of PA intensity
• Self-report of physician diagnosis
• No differentiation of arrhythmia type
• Risk of selection bias
• Incomplete statistical reportingModerate Bapat et al,42 2014 • Participants from MESA database NA • Highest of 3 PA intensity categories was > 2383 MET† min/wk
• AF• At highest intensity PA in 1 model, HR = 0.79, 95% CI 0.61 to 1.02; P < .05* • There are insuffcient data to properly evaluate this study High Drca et al,43 2014 • 44 410 Swedish men
• Mean follow-up of 12 y60 • Any leisure-time PA of > 5 h/wk
• AF or atrial futter• Walking or cycling at age 30 y showed beneft in AF reduction
• Risk of AF increased at age 30 y for > 5 h/wk of PA (RR = 1.19, 95% CI 1.05 to 1.36; P = .008)*• Men only
• Risk of recall bias
• Self-assessment of PA intensity
• Outcomes included AF and atrial futterModerate Ghorbani et al,44 2014 • 28 169 US men
• 8-y follow-up68 • PA > 6 MET† with high MET h/wk • No correlation between AF and PA* • Men only
• Self-assessment of PA intensity
• Self-report of physician diagnosis
• Participation and dropout rates were unclearModerate Knuiman et al,45 2014 • 4267 adults from Busselton, Western Australia; 44% men
• 15-y follow-up52 • Vigorous exercise in a usual week
• AF• Higher level of PA associated with non-signifcant trend to reduced AF* • 57% survey response
• Self-assessment of PA intensity
• Risk of recall biasModerate Myrstad et al,46 2014 • 2366 Norwegian men participating in 56-km cross-country ski race vs 1179 men from general population
• 9-y follow-up66 • Endurance PA for > 30 min > 3 times per wk
• AF or atrial futter• Increased risk of AF for 10 y of vigorous PA (HR = 1.16, 95% CI 0.06 to 1.28) in skiers* • Men only
• Controls from different population
• Self report of recent PA
• Risk of selection biasModerate AF—atrial fibrillation, HR—hazard ratio, MESA—Multi-Ethnic Study of Atherosclerosis, MET—metabolic equivalent task, NA—not available, PA—physical activity, RCT—randomized controlled trial, RR—relative risk.
↵* After adjustment for confounding variables.
↵† A physiologic measure of energy cost of a physical activity: 1 MET = 1 kcal/kg/h.
STUDY STUDY TYPE TYPE OF ATHLETES AF OUTCOMES RISK OF BIAS Andersen et al,39 2013 Cohort Swedish cross-country skiers for 90-km event • HR = 1.29 (95% CI 1.04 to 1.61) for > 5 completed races
• HR = 1.20 (95% CI 0.93 to 1.55) for those with fastest times
• 87% of study participants were menLow Baldesberger et al,47 2008 Case control Former Swiss elite cyclists • AF developed in 10% of cyclist group and in 0% of control group (BGD P value of .028)
• Study included only menHigh Grimsmo et al,48 2010 Cross sectional Elite-level Norwegian cross-country skiers • AF prevalence of 16.7% was found
• Lone AF prevalence of 12.8% was found
• Study included only menHigh Karjalainen et al,31 1998 Cohort Top-level orienteers (runners) • AF developed in 5.3% of orienteers vs 8.9% of control group (RR = 5.5; P = .012)
• Study included only menHigh Molina et al,34 2008 Retrospective cohort Runners in Barcelona Marathon • Endurance sport practice associated with higher risk of lone AF (HR = 8.80, 95% CI 1.26 to 61.29; P = .028)
• Study included only menModerate Myrstad et al,46 2014 Cohort Norwegian crosscountry ski racers for 56-km event • Increased risk of AF for 10 y of vigorous PA (HR = 1.16, 95% CI 0.06 to 1.28)
• Study included only menModerate Myrstad et al,49 2014 Cross sectional Participants in Birkebiner crosscountry ski race—a course of 54 km and 1000 m uphill • AF in men currently practising endurance sport (OR = 1.81, 95% CI 1.04 to 3.14)
• Study included only men
• 78% of study participants were menHigh Pelliccia et al,37 2010 Cohort Olympic athletes • No cardiac events developed for more than 8 y
• Reduced incidence compared with general populationHigh Van Buuren et al,50 2012 Cross sectional Elite German handball players • AF prevalence of 30.3% in former athletes
• Study included men onlyHigh AF—atrial fibrillation, BGD—between-group difference, HR—hazard ratio, OR—odds ratio, PA—physical activity, RR—risk ratio.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.