


Abstract
Objective To document the management of and outcomes for patients receiving narcotic replacement and tapering with long-acting morphine preparations during pregnancy.
Design A prospective cohort study over 18 months.
Setting Northwestern Ontario.
Participants All 600 births at Meno Ya Win Health Centre in Sioux Lookout, Ont, from January 1, 2012, to June 30, 2013, including 166 narcotic-exposed pregnancies.
Intervention Narcotic replacement and tapering of narcotic use with long-acting morphine preparations.
Main outcome measures Prenatal management of maternal narcotic use, incidence of neonatal abstinence syndrome, and other neonatal outcomes.
Results The incidence of neonatal abstinence syndrome fell significantly to 18.1% of pregnancies exposed to narcotics (from 29.5% in a previous 2010 study, P = .003) among patients using narcotic replacement and tapering with long-acting morphine preparations. Neonatal outcomes were otherwise equivalent to those of the nonexposed pregnancies.
Conclusion In many patients, long-acting morphine preparations can be safely used and tapered in pregnancy, with a subsequent decrease in observed neonatal withdrawal symptoms.
Illicit narcotic use during pregnancy is a pervasive problem in northwestern Ontario. In 2010, 17% of pregnancies were affected by narcotic abuse and 29.5% of neonates from exposed pregnancies experienced some degree of neonatal abstinence syndrome (NAS).1 In 2013, the rate of narcotic abuse in pregnancy rose to 28% (P < .001).2
The Meno Ya Win Health Centre in Sioux Lookout, Ont, provides obstetric services to a catchment area of 28 000 primarily First Nations patients (Figure 1).3–5 None of these remote communities hosts a methadone maintenance program. In response to the high incidence of narcotic abuse in pregnancy, a narcotic replacement and tapering program using long-acting morphine preparations was instituted. The purpose of this study is to document the role narcotic tapering with long-acting morphine preparations can play in the management of narcotic abuse in pregnancy.
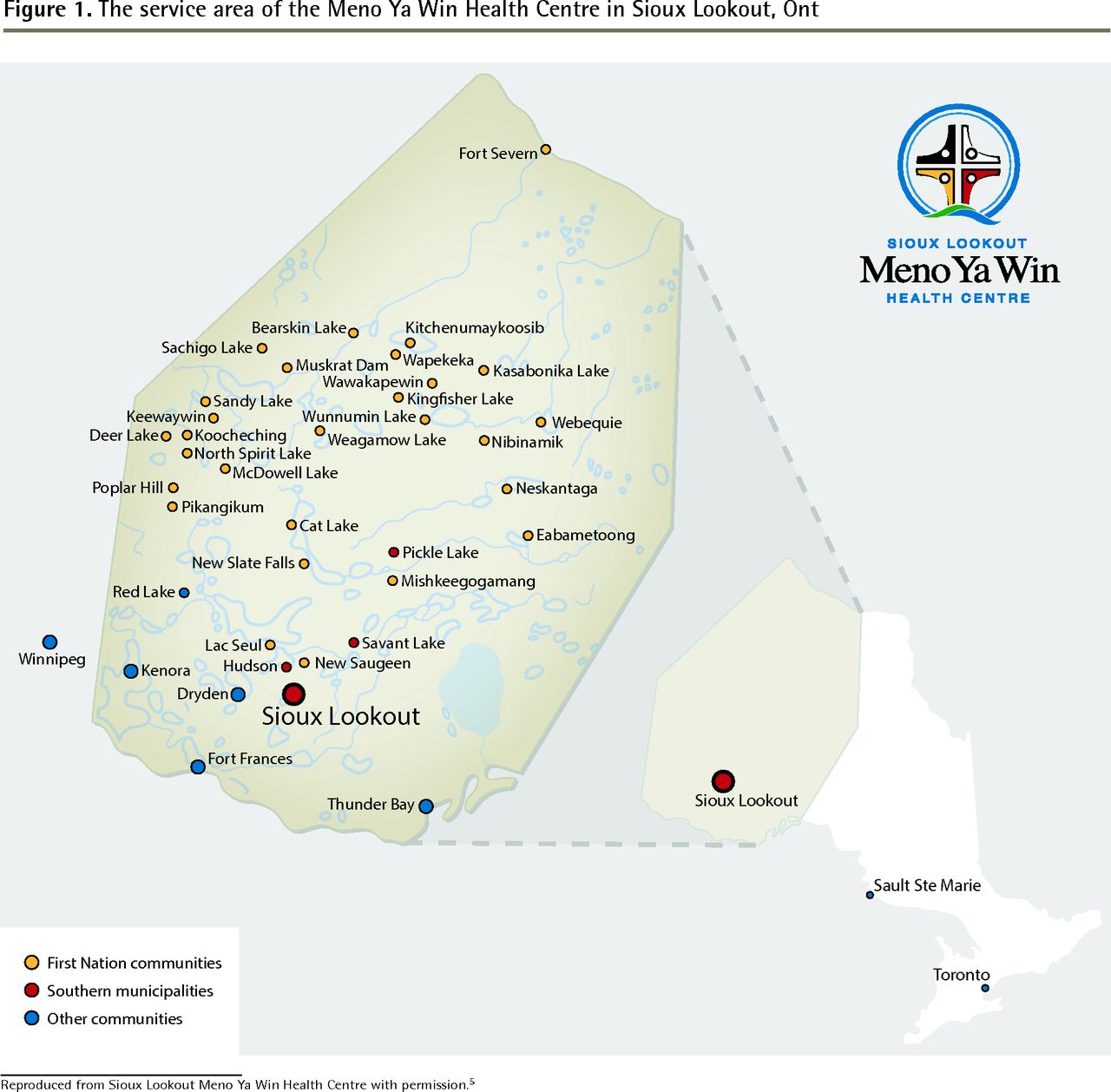
The service area of the Meno Ya Win Health Centre in Sioux Lookout, Ont
Reproduced from Sioux Lookout Meno Ya Win Health Centre with permission.5
METHODS
All 600 births occurring at Meno Ya Win Health Centre from January 1, 2012, to June 30, 2013, were prospectively studied. Data related to maternal attendance at the integrated prenatal clinics and specialized narcotic-in-pregnancy clinics were analyzed. In addition to typical prenatal data, information regarding type, amount, and route of drug abuse was documented. Birth outcome information including Apgar scores, birth weights, gestational age, and stillbirths was gathered, as were addiction-related outcome measures: Finnegan scores, incidence of NAS, and neonatal treatment. The Sioux Lookout Meno Ya Win Health Centre Research Review Committee granted ethics approval.
Statistical analysis was performed using SPSS, version 21.0 for Windows. Data were initially analyzed descriptively, including means and standard deviations for continuous data and frequencies and percentages for categorical data. Independent-samples t tests were used for continuous data to compare the tapered and nontapered exposed pregnancies, and the nonexposed pregnancies. Pearson
 tests were used to compare the groups for categorical data.
tests were used to compare the groups for categorical data.
Modified Finnegan scoring was used by the treating physician or obstetric nurse as the practical measure of neonatal symptoms of withdrawal from opioids.6
Prenatal care in the 31 remote First Nations communities in our catchment area is initiated at the nursing station by local nurses and visiting family physicians who fly in 1 week each month. The integrated prenatal program based at the Meno Ya Win Health Centre holds daily clinics for patients near term or those referred earlier for potential complications. The number of narcotic-use referrals required the institution of twice-weekly narcotic-in-pregnancy clinics as well. These are staffed by a family physician, a nurse, a social worker, and a lactation consultant. Four family physicians are currently involved, 3 of whom also provide cesarean section coverage. The same family physicians also provide intrapartum and postpartum care of mothers and neonates. All narcotic-exposed patients receive their prenatal and narcotic management at the Meno Ya Win Health Centre, with direct observed therapy for prescribed narcotics. A standardized questionnaire about addictions is completed and written informed consent is obtained. Other nonexposed pregnancies also receive their prenatal care at the centre.
When the program began, 2 types of controlled-release morphine (MS Contin or M-Eslon) were commonly used twice daily for replacement and tapering; currently Kadian is typically used owing to its simpler once-daily dosing. Patients are seen daily as needed. Narcotic carries are seldom prescribed. If return to a northern community is undertaken, community nurses or reliable family or community members are contacted for in-community dispensing. Urine drug screening is performed for every patient. Counseling by family physicians, social workers, and First Nations mental health workers is offered on a case-by-case basis. All services—obstetric services, ultrasound scans, narcotic substitution or tapering, delivery, and daily 7-to 10-day postpartum follow-up—are provided at the Meno Ya Win Health Centre. Prenatal and narcotic management, including care of partners and, at times, other children, are integrated into the one setting.
RESULTS
In the 18 months of the study (January 1, 2012, to July 1, 2013), 600 births were attended, including 166 (27.7%) narcotic-exposed pregnancies (Table 1). Eighty-six of these narcotic-using pregnant women (51.8%) participated in the narcotic-in-pregnancy tapering program. Despite being off the market since early 2012, 85% of the narcotic abuse we encounter involves OxyContin.2,7 Polysubstance abuse included cocaine (9 patients), morphine (5 patients), methadone (3 patients), benzodiazepines (2 patients), and methamphetamines (2 patients). No changes were made in our prenatal clinic during the time frame of the study other than instituting the formalized narcotic replacement and tapering program. Urine drug screening was universal in the narcotic tapering program.
Maternal characteristics
Each patient and couple was assessed individually. With the exception of some occasional users, all narcotic users were offered participation in our narcotic replacement and tapering program.
The 86 patients tapered with long-acting morphine included 24 who received MS Contin (or M-Eslon) and 48 who received Kadian. Eight patients who were already started on buprenorphine in their northern communities also participated and were tapered on that medication (Table 2). Morphine-equivalent doses of narcotics were calculated by standard methods, and each patient was changed to an oral starting dose and seen daily until clinically stabilized. A daily dose of 90 mg of Kadian orally was a common starting dose (the average morphine dose was 54 mg), and the dose was slowly titrated or maintained as the patient tolerated. The eventual end dose for most (58.5%) of the tapered patients was between 0 and 10 mg of long-acting morphine per day; the average morphine end dose for the total tapering cohort was 16 mg (Table 3). The length of the weaning varied based on patient comfort and degree of dependence, and ranged from 7 to 238 days (mean [SD] of 101 [67], median 98).
Comparison of tapering agents
Tapering profile: N = 86.
By delivery, 91.9% of the tapered patients had quit (9.3%) or decreased their substitute narcotic doses (82.6%) (Table 4). Of the tapered patients who decreased their doses, 53.3% used only the taper drug at delivery; others still occasionally used some oxycodone. Quit rates were based on self-reporting, supported by urine drug screening. Of the 30 urine screening test results that were positive for oxycodone close to delivery, only 3 were in patients who professed having “quit” narcotics, and they were all in the taper program. Most of the urine test results positive for oxycodone were in tapered patients who admitted to ongoing but decreased use of illicit narcotics who were therefore expected to have ongoing positive urine test results (18 of 30). Urine drug screening was not performed for the neonates.
Rates of narcotic quitting and dose decrease
The narcotic-exposed mothers who did not participate in tapering or who were not offered replacement and tapering were generally only occasional users. Offering them long-acting morphine, even with tapering, would have, in effect, increased their narcotic intake. This group of 80 patients who also attended the integrated prenatal clinic also had high quit (40.0%) or decrease (22.5%) rates.
The incidence of any NAS experienced by narcotic-exposed infants was 18.1% in 2013. The proportion of infants with high Finnegan scores who required pharmacologic therapy (morphine or phenobarbital) for their symptoms (2 consecutive Finnegan scores ≥ 8) was low, at 1.5% of total births. All infants roomed in with their mothers. Other neonatal outcomes were largely similar to those of the nonexposed pregnancies (Table 5).
Neonatal characteristics
Thirty men were also treated with taper protocols similar to their pregnant female partners. After hospital discharge, families are housed for 7 to 10 days at the attached 100-bed First Nations hostel. They are followed daily for maternal and neonatal health, weight gain, and any signs of narcotic withdrawal or need for further treatment as inpatients or outpatients. The length of hospital stay was statistically longer for narcotic-exposed, tapered pregnancies (P < .001).
In this 18-month study, 15 deliveries occurred out of hospital (typically, precipitously back home in the nursing station), and only 2 of these were in narcotic-exposed pregnancies, neither of which were being tapered.
Postpartum women from communities that had developed buprenorphine maintenance programs were transitioned into those programs.
DISCUSSION
The narcotic replacement and tapering program using long-acting morphine facilitated a significant decrease in neonatal withdrawal. The incidence of NAS in narcotic-exposed pregnancies fell from 29.5% in 2010 to 18.1% in 2013 (P = .003).1,2 Despite the overall proportion of narcotic-exposed pregnancies rising from 17% to 28%, neonates requiring pharmacologic management, as a percentage of total births, fell from 2.5% to 1.5% (P = .403).1,2
Neonates from tapered pregnancies did have significantly lower birth weights (P = .001), but the difference was not thought to be clinically relevant, with an average birth weight of 3301 g in the tapered cohort.
This prenatal narcotic-tapering program is unique in 3 ways: the use of long-acting morphine preparations, the tapering of narcotics in pregnancy, and care delivered by generalist family physicians.
Long-acting morphine is the most accessible narcotic in rural Canada. Methadone clinics and facilities are largely urban. Accessing federal funding and stock for methadone and buprenorphine in remote First Nations communities can be problematic, especially with the clinical immediacy of narcotic use and withdrawal in a pregnant patient. Fischer et al demonstrated the equivalency of long-acting morphine versus methadone in a small randomized study in 1999 (N = 48).8 A 2013 Cochrane review also found equivalency to methadone.9 The Society of Obstetricians and Gynaecologists of Canada clinical practice guidelines allow for the use of long-acting morphine, as do the 2012 Ontario provincial guidelines, particularly where methadone programs are not available.10,11 These latter guidelines noted the epidemic of narcotic use in our region, and although methadone maintenance was generally recommended, the guideline authors recognized that our region might need to consider narcotic replacement and tapering with long-acting morphine preparations.12
Tapering narcotics in pregnancy raises the twin concerns of precipitating maternal and fetal withdrawal.13 Geographic factors in our region, with dozens of isolated remote communities, interrupt the supply chain of many commodities, including illicit narcotics. We have many patients who use intermittently owing to availability as well as poverty, making narcotic withdrawal a common challenge. Once we have initiated a long-acting morphine replacement, our tapering schedule is very gradual. The recommended 10% weekly reduction is typically spread out over a longer period of time according to patient preference, withdrawal apprehension, and physical symptoms.14 McCarthy has discussed the possibility of intrauterine fetal withdrawal in an urban context, which might be more likely to involve multidrug and daily heroin users.13 In this context methadone maintenance makes good sense. The absence of any common test for intrauterine withdrawal renders it a real concern, but without clear implications in our setting. Our finding that many of our patients decreased or quit narcotic use without documented measurable neonatal adverse effect is an important one. A US study in 2013 of inpatient detoxification of 95 pregnant women being treated with decreasing doses of methadone resulted in a 56% success rate and no neonatal adverse outcomes.15 In 2012, Ontario guidelines and the Centre for Addiction and Mental Health both identified our catchment area as one where traditional methadone maintenance programs would not be able to address the scope of the problem.10,12,14 The Ontario guidelines specifically acknowledge that, in our setting, opioid tapering might be a useful approach.12 The Centre for Addiction and Mental Health’s 2012 health alert attests: “based on recent evidence, there is minimal risk associated with tapering opioids during pregnancy.”14 All patients regularly using opioids in our study were offered tapering. Those who declined continued to be offered routine prenatal care, including fetal surveillance with regular biophysical profiles and supportive counseling. It is recommended that tapering occur in the second and third trimesters, and that is when most of our tapering occurred. However, patients were tapered so gradually with our approach that it was initiated in the first trimester (and completed in the second trimester) if the patient expressed a wish to begin reducing her narcotic use. Because decreasing the incidence of NAS was one of our program goals, we offered tapering to all regular narcotic users, and the patient ultimately decided by her comfort level whether she was maintained or slowly tapered. Patients who were occasional users constituted a large component of the exposed, nontapered cohort. This group had high quit rates and lower rates of NAS, presumably owing to self-directed narcotic management or response to the program’s supportive addiction treatment environment. All quit determinations were self-reported, supported by urine drug screening.
Another of the unique aspects of our program is the involvement of generalists with a broad scope of practice.4 These family physicians are involved in prenatal, intrapartum, postpartum, and neonatal care of the mother, child, and partner. They have become experienced in addiction management and can treat mother, father, and neonate. This multirole perspective, common in rural and urban family medicine, allows for an integrated approach early in pregnancy to safely reducing the incidence of NAS.16 It also reduces the need for long-distance travel to urban centres for care, which further disrupts families already dealing with addiction issues.
The rural First Nations population we serve differs from opioid-dependent patient populations encountered in the literature. Baewert and colleagues, in their subanalysis of the multicentre MOTHER [Maternal Opioid Treatment: Human Experimental Research] study, noted a difference between rural and urban settings that suggested women in urban areas were more severely affected.17 Additionally, the epidemic of oxycodone abuse encountered in our region is currently a pervasive social as well as medical issue. Clearly this is a whole-community problem, and it is being addressed directly by community-based initiatives across northwestern Ontario.18–20 It does not just involve an isolated sector of society. This might both allow more openness in discussing the topic as well as facilitate creative, workable solutions that are a good fit for dealing with opioid dependence in pregnancy.
It can be argued that NAS has a known treatment with no known serious sequelae for the neonate and that avoiding it has limited value. The traditional approach to narcotic use of any type during pregnancy is to treat mothers with relatively high-dose methadone in the prenatal period and to provide prolonged neonatal care unit stays for the neonate postpartum. It is not generally acknowledged that this approach might unnecessarily cause a considerable disruption to family life and maternal-child bonding when a simpler approach might be effective.
Limitations
Owing to the busy nature of the obstetric program, some patient information was missing. Finnegan scoring is a user-dependent process but it is the commonly used standard in Canadian hospitals. In-house training sessions with physicians and obstetric nurses were undertaken to address our initial inexperience. During the time frame of the study, many First Nations communities were developing various buprenorphine-naloxone maintenance programs, and willing postpartum patients were transitioned into these programs upon their request. Community-based follow-up with addictions workers is also available to returning couples. Not all communities have equivalent local program support, and this remains one of the limitations of the spectrum of care in our region. Urine drug screening was universally done in the prenatal clinic but not routinely at time of delivery, so findings for the last prenatal urine collection were used in our results.
Conclusion
In the right setting, with appropriate patient screening and support, long-acting morphine can be safely initiated and tapered in pregnancy for patients abusing narcotics. Our program has safely lessened the incidence of NAS and plays an important role in the treatment of families with addiction during pregnancy in our region.
Acknowledgments
This study was supported by the Northern Ontario Academic Medicine Association Clinical Innovation Opportunities Fund.
Notes
EDITOR’S KEY POINTS
-
Illicit narcotic use during pregnancy is a pervasive problem in northwestern Ontario, affecting 28% of pregnancies in 2013. In response to this high incidence of narcotic abuse in pregnancy, the Meno Ya Win Health Centre in Sioux Lookout, Ont, instituted a narcotic replacement and tapering program using long-acting morphine preparations.
-
Approximately half of women using narcotics during their pregnancies agreed to participate in the program, and many patients decreased or quit narcotic use without documented measurable neonatal adverse effect. By delivery, 91.9% of participants had quit (9.3%) or decreased (82.6%) their long-acting morphine dose, although almost half of those who decreased their dose were still occasionally using oxycodone. The incidence of neonatal abstinence syndrome among participants decreased significantly (P = .003) from that found in a previous study in this setting. Other neonatal outcomes were similar to those of nonexposed pregnancies.
POINTS DE REPÈRE DU RÉDACTEUR
-
La consommation illicite de narcotiques durant la grossesse est un problème persistant dans le nordouest de l’Ontario; en 2013, il touchait 28 % des grossesses. En réponse à la forte incidence de cette narco-dépendance durant la grossesse, le centre de santé Meno Ya Win à Sioux Lookout, en Ontario, a instauré un programme de remplacement et de sevrage des narcotiques à l’aide de préparations de morphine à action prolongée.
-
Environ la moitié des femmes qui prenaient des narcotiques durant leur grossesse ont accepté de participer au programme et plusieurs d’entre elles ont réduit ou cessé leur consommation de narcotiques sans qu’on puisse documenter d’effets néonataux indésirables. Au moment d’accoucher, 91,9 % des participantes avaient abandonné (9,3 %) ou diminué (82,6 %) leur dose de morphine à action prolongée, quoique près de la moitié de celles qui avaient réduit leur dose consommaient encore de l’oxycodone à l’occasion. L’incidence du syndrome de sevrage néonatal chez les participantes avait diminué de façon significative (P = ,003) par rapport à celle observée dans une étude antérieure dans le même contexte. Les autres issues néonatales étaient semblables à celles des grossesses non exposées.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Contributors
Ms Kakekagumick, Ms Muileboom, Ms Dooley, and Ms Brunton performed the data collection and literature search and review. Ms Dooley also designed data collection software. Drs Dooley, Antone, Guilfoyle, and Gerber-Finn contributed clinical program development and management, data collection, and draft approvals. Ms Cromarty was Special Advisor on First Nations Health at the time of the study and ensured the project met community expectations of the First Nations for hospital-based research. Ms Hopman performed statistical analysis and data organization. Dr Kelly contributed to the overall research design and writing. All authors approved the final draft.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Addiction in the family: Two Indigenous families overcoming barriers to opioid agonist therapy
- First Nations hepatitis C virus infections: Six-year retrospective study of on-reserve rates of newly reported infections in northwestern Ontario
- Observational study of the safety of buprenorphine+naloxone in pregnancy in a rural and remote population
- Buprenorphine-naloxone use in pregnancy for treatment of opioid dependence: Retrospective cohort study of 30 patients