


Article Figures & Data
Figures
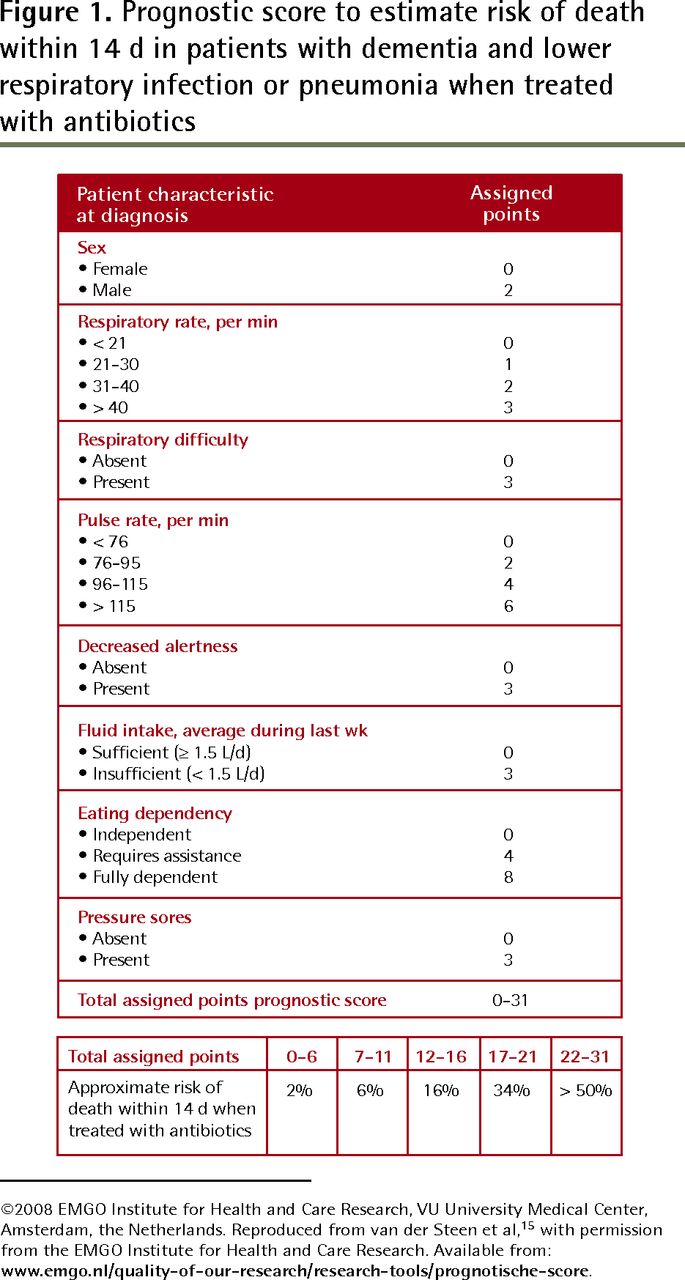
- Figure 1.
Prognostic score to estimate risk of death within 14 d in patients with dementia and lower respiratory infection or pneumonia when treated with antibiotics
©2008 EMGO Institute for Health and Care Research, VU University Medical Center, Amsterdam, the Netherlands. Reproduced from van der Steen et al,15 with permission from the EMGO Institute for Health and Care Research. Available from: www.emgo.nl/quality-of-our-research/research-tools/prognotische-score.
Tables
SYMPTOM MANAGEMENT Dyspnea Identify cause -
Pneumonia is the most frequent cause; sometimes pulmonary edema
-
Antibiotics might improve comfort (reduce secretions) but prolong dying. Discuss goals of care. If goal of care is comfort but no life prolongation, then “no antibiotics” is appropriate and necessitates good symptom management
Use opioids, as they are the most effective treatment-
Start with either 0.5 mg of hydromorphone SC every 4 h as needed or 2–2.5 mg of morphine SC every 4 h in opioid-naive patients
-
If dyspnea is persistent, give doses every 4 h with breakthrough doses (10% of total daily opioid dose given every 1 h)
Use 20–40 mg of furosemide (SC or IV) if there is evidence of fluid overload
Use oxygen
-
Oxygen might improve oxygen saturation but it does not improve dyspnea, as it is related to respiratory muscle fatigue. Use oxygen only if the patient is hypoxic and it appears helpful (can be stopped if patient is actively dying and comatose)
If dyspnea remains severe, prescribe-
5–10 mg of midazolam SC plus morphine or hydromorphone 1.5 times the usual 4-h dose plus scopolamine 0.4–0.8 mg and repeat morphine or hydromorphone and midazolam after 20 min as needed
Prescribe nonpharmacologic therapy-
Providing a cool draft from an open window or fan and maintaining a calming presence are also helpful
Terminal rales (“death rattles”) Reposition the patient, as this is often the best strategy
-
Avoid suctioning except superficially without causing gagging. This can be done after lowering the head of the bed for a short time (if tolerated)
Start pharmacologic treatment-
0.2–0.8 mg of scopolamine* SC every 4–6 h as needed (maximum dose is 0.8 mg SC every 2 h)
-
Scopolamine might be more effective if given on a regular basis
-
0.2 to 0.4 mg of glycopyrrolate SC every 4 h might be preferred (less sedative)
-
20–40 mg of furosemide SC might help if there is fluid overload
Pain Prescribe opioid (oral or SC administration) -
Hydromorphone might be preferable because of fewer active metabolites, diminishing risk of opioid toxicity
-
Start opioid slowly: 0.25-0.5 mg of hydromorphone every 4 h (can be given as needed; however, when the patient cannot communicate, low-dose regular medication is often preferable); or 1–2.5 mg of morphine SC every 4 h (second choice)
-
After 24 h, calculate the daily dose needed and give regularly in divided doses with breakthrough doses (half of regular dose) every 1 h
-
Increase regular dosage if > 3 breakthrough doses daily
Agitation Consider treatable causes of pain (eg, full bladder, fecaloma, dry mouth)
Consider the following:-
Often irreversible (might be due to opioid toxicity. Reduce morphine dose or change to hydromorphone, which has fewer active metabolites)
-
Antipsychotics are normally the first choice in delirium (eg, 2.5–5 mg of methotrimeprazine every 6 h as needed), but if agitation is mild to moderate in an actively dying patient, benzodiazepines given regularly (0.5–1 mg of lorazepam SC every 4 h regularly for palliative sedation) might be more useful than antipsychotics
-
If benzodiazepines are ineffective or cause paradoxical excitation, change to 12.5–50 mg of methotrimeprazine over a 24-h period in divided doses every 4–6 h, or 0.5–2 mg of haloperidol SC every 30 min until agitation is controlled, then give regularly every 4–6 h
Myoclonus (frequent side effect of morphine) Change morphine to hydromorphone and add 0.5 mg of lorazepam every 4 h as needed or regularly -
IM—intramuscular, IV—intravenous, SC—subcutaneous.
-
↵* Use of scopolamine or other antimuscarinics in this situation is controversial. Some authors believe that this symptom is not burdensome for the comatose patient and that the treatment might not be in the patient’s interest if used only to comfort family.2
-
Data from van der Maaden et al,2 Ferris et al,11 Twycross et al,19 and Néron.20
-
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Limits of advance directives in decision-making around food and nutrition in patients with dementia
- A patients experience in dementia care: Using the "lived experience" to improve care
- Lexperience dune patiente qui recoit des soins pour la demence: Utiliser << lexperience vecue >> pour ameliorer les soins
- Enjeux de fin de vie dans les cas de demence avancee: 1re partie : objectifs des soins, processus de prise de decision et education des proches
- End-of-life issues in advanced dementia: Part 1: goals of care, decision-making process, and family education