


Abstract
Objective To compare the perceptions of breast cancer survivors and primary care physicians (PCPs) about PCPs’ ability to deliver survivorship care in breast cancer.
Design Mailed survey.
Setting British Columbia.
Participants A total of 1065 breast cancer survivors who had completed treatment of nonmetastatic breast cancer within the previous year, and 587 PCPs who had patients with nonmetastatic breast cancer discharged to their care within the preceding 18 months.
Main outcome measures Breast cancer survivors’ and PCPs’ confidence ratings of PCPs’ ability to deliver the following aspects of care: screening for recurrence; managing osteoporosis, lymphedema, endocrine therapy, menopausal symptoms, and anxiety about or fear of recurrence; and providing nutrition and exercise counseling, sex and body image counseling, and family counseling. Response options for each question included low, adequate, or good. Responses were summarized as frequencies and compared using χ2 tests.
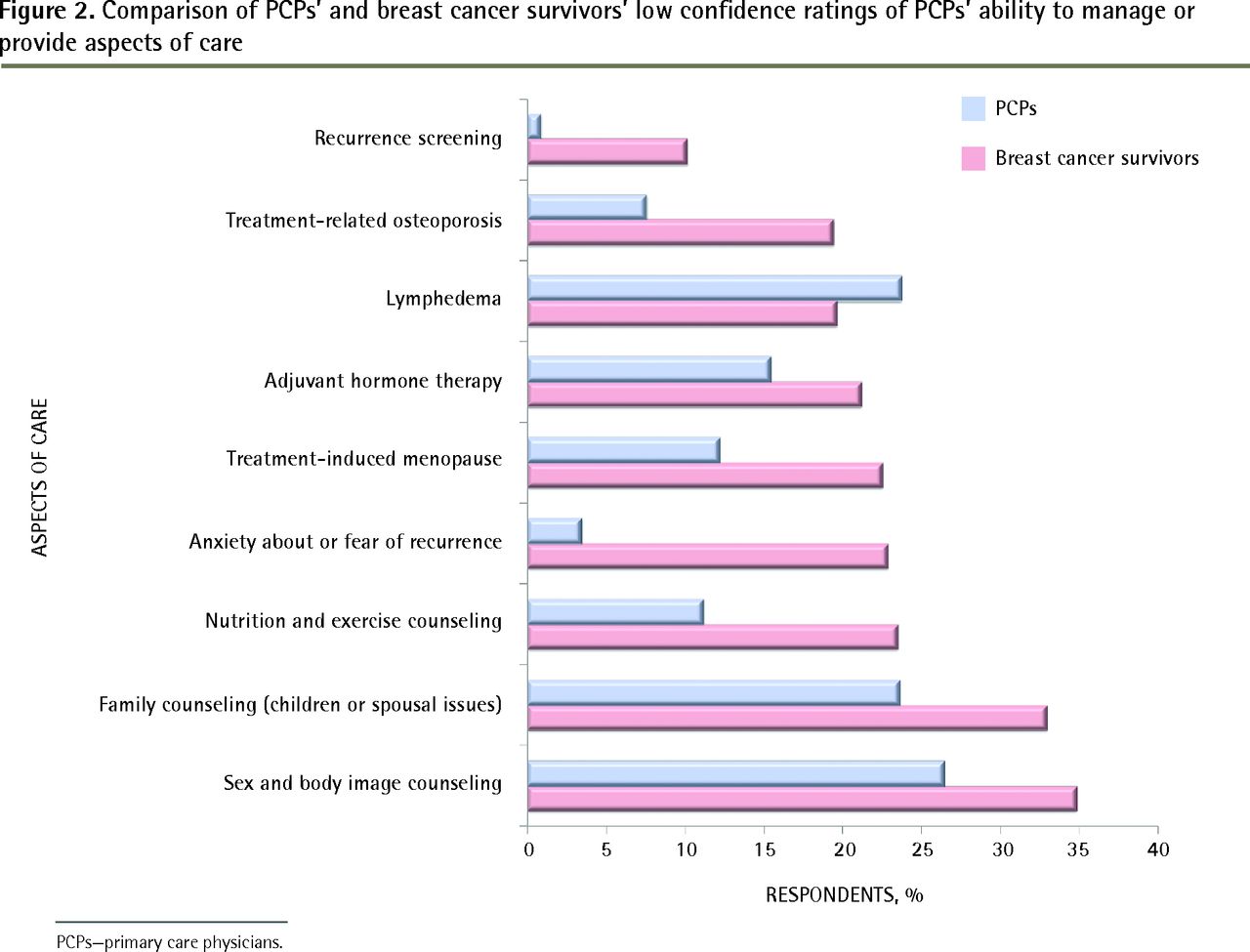
Results Response rates for breast cancer survivors and PCPs were 47% and 59%, respectively. Responses were statistically different in all categories (P < .05). Both groups were most confident in the ability of PCPs to screen for recurrence, but breast cancer survivors were 10 times as likely to indicate low confidence (10% of breast cancer survivors vs 1% of PCPs) in this aspect of care. More breast cancer survivors (23%) expressed low confidence in PCPs’ ability to provide counseling about fear of recurrence compared with PCPs (3%). Aspects of care in which both breast cancer survivors and PCPs were most likely to express low confidence included sex and body image counseling (35% of breast cancer survivors vs 26% of PCPs) and family counseling (33% of breast cancer survivors vs 24% of PCPs). Primary care physicians (24%) described low confidence in their ability to manage lymphedema.
Conclusion Breast cancer survivors and PCPs are reasonably confident in a PCP-based model of survivorship care. Primary care physicians are confident in their ability to manage physical effects related to breast cancer, with the exception of lymphedema. Low confidence ratings among both groups in psychosocial aspects of care suggest an area for improvement.
Each year an increasing number of breast cancer patients transition from active treatment to follow-up care. With a 5-year relative survival ratio of 88%, it is expected that most will live many years beyond their breast cancer diagnosis and treatment.1 Thus, while women continue to be diagnosed with breast cancer, improved outcomes means a greater proportion will be entering the survivorship phase, a distinct chapter in the cancer journey.2,3
Care of breast cancer survivors is complex. Common issues include chronic physical effects of therapy,4–8 psychosocial challenges such as depression and anxiety,5,6,9–14 sexual functioning,15–18 and stress on relationships with family members and friends.13,14,19 To address the individual needs of breast cancer survivors, various models of follow-up care have been proposed, including combined care with both oncologists and primary care physicians (PCPs), or predominantly PCP care.20–25 In the latter model, PCPs deliver cancer-specific care while addressing other health concerns. Even with a combined care model, PCPs require some knowledge of the physical and psychosocial issues that breast cancer survivors face.
Studies show that breast cancer survivors followed by PCPs have similar rates of recurrence detection and health-related quality of life as those followed by oncologists21; however, some have found that breast cancer survivors have low confidence in PCPs’ ability to provide cancer-specific care.3,11,20,24,26 Other studies suggest that patient preference is affected more by the practices they are accustomed to than evidence as to what is most effective27 and acknowledge that a trusting long-standing doctor-patient relationship is important.24,28,29 With PCP-led follow-up, the preferences and concerns of both patients and providers must be addressed, as failure to do so affects patient perception of quality of care,24,28,30 as well as physician willingness to assume full responsibility for care.31,32 Primary care physicians themselves have concerns about providing follow-up care, including dealing with challenges in communication with specialists and having sufficient resources (time and reimbursement) and training to manage physical and psychosocial issues effectively.3,25,32–34
Despite our knowledge that PCP-led care for breast cancer survivors causes concern for both breast cancer survivors and PCPs, no studies to date have investigated the confidence of these groups in PCPs’ ability in specific aspects of follow-up care. The purpose of this study was to compare the perceptions of breast cancer survivors and PCPs about PCPs’ ability to deliver aspects of care for breast cancer survivors.
METHODS
The British Columbia Cancer Agency (BCCA) provides all radiotherapy services and manages the budget for all antineoplastic drugs in the province; it also has a centralized charting system and transcription and letter dissemination process for PCPs regarding follow-up care. Throughout their course of treatment, patients are seen regularly by their oncologists, from whom PCPs receive correspondence after each clinical encounter. Approximately two-thirds of breast cancer patients are discharged from the BCCA within 1 year of active treatment completion (chemotherapy or radiation therapy). At the time of discharge from the cancer centre, the oncologist typically dictates a letter to the PCP, summarizing a patient’s diagnosis, treatments delivered, surveillance recommendations, and the recommended type and duration of adjuvant endocrine therapy. Also, a standardized follow-up letter is available for oncologists to send to PCPs specifically outlining surveillance recommendations and side effects of hormonal therapy, if prescribed.
Approval from the University of British Columbia and BCCA Research Ethics Board was obtained in order to identify eligible participants from electronic medical records. We identified 1023 eligible PCPs who had at least 1 female patient with nonmetastatic breast cancer discharged from the BCCA for ongoing follow-up during a period of 3 to 18 months before the first survey mailing. Eligibility criteria for breast cancer survivors required that participants spoke English, had been assessed for nonmetastatic invasive breast cancer, and had completed active treatment (defined as surgery, radiation therapy, intravenous chemotherapy, or trastuzumab therapy; patients could still be receiving endocrine therapy) in the preceding 9 to 12 months, with no indication of recurrence and no previous cancer diagnosis. A total of 2289 breast cancer survivors were identified who met these criteria.
The PCP survey was developed by 2 oncologists and designed to obtain PCPs’ perspectives on their ability to manage aspects of care for breast cancer survivors and to identify potential ways to assist PCPs in enhancing the delivery of these aspects of care in practice. The final version of the survey was intentionally condensed to 1 page and designed for completion in 2 to 3 minutes. Before distribution, the survey was tested among 4 PCPs for face validity, content, relevance, and time required for completion, and then was revised accordingly.
The breast cancer survivor survey was designed using findings from focus groups with breast cancer survivors and included sections on demographic information, severity of physical and psychosocial effects in the year following treatment, and preferences about follow-up care.35 The survey instrument was validated with a group of 10 breast cancer patients being seen for routine follow-up at BCCA clinics, and with 10 breast cancer patients who participated in the focus groups. One question on the breast cancer survivor survey specifically asked about their confidence in the ability of their PCPs to manage the same aspects of survivorship care: “If you had to approach your family physician about any of the following concerns after you completed active treatment for breast cancer, what would your confidence level be in his or her ability to manage them appropriately?” Response options were identical to question 6 in the PCP survey.
The PCP survey was sent to 1000 of 1023 identified eligible PCPs, using survey administration methods described in a previous publication.36 Two mailings were done. The first included a cover letter, the survey, and a postage-paid return envelope. Physicians were asked to respond anonymously by fax or mail. To increase sample size and recruitment, a second mailing was sent 1 month later, with a modified cover letter instructing participants not to complete the survey twice. Responses were anonymous. The breast cancer survivor survey was sent to all 2289 breast cancer survivors who met the inclusion criteria. One mailing was sent. For breast cancer survivors, surveys were labeled with a unique identifier that could later be linked to disease and treatment information.
Statistical analysis
Responses were summarized as frequencies, and results from breast cancer survivors and PCPs were compared using χ2 tests. Our analysis primarily focused on rates of low confidence responses, which we believed to be areas where improvements might be needed.
RESULTS
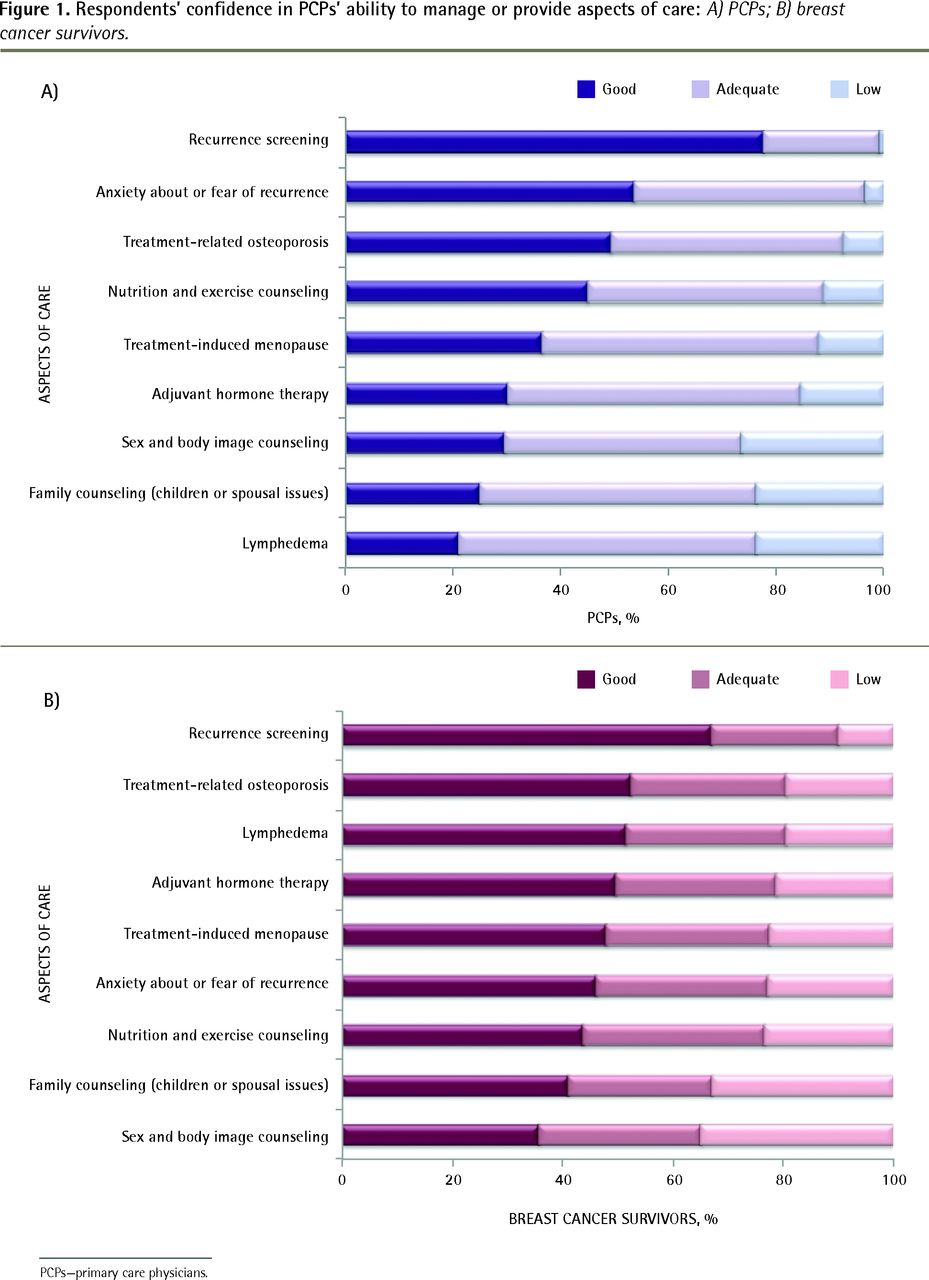
Response rates for breast cancer survivors and PCPs were 47% (1065 of 2289) and 59% (587 of 1000), respectively. Primary care physicians’ and breast cancer survivors’ responses are presented in Figure 1, and are statistically different in all categories (P < .05). Breast cancer survivors were more polarized in their responses than PCPs were, and were more likely to respond good or low, while PCPs’ self-evaluations were more likely to be good or adequate responses. Most of the responses from both PCPs and breast cancer survivors were good or adequate in all aspects of care.

Respondents’ confidence in PCPs’ ability to manage or provide aspects of care: A) PCPs; B) breast cancer survivors.
PCPs—primary care physicians.
Overall, PCPs were fairly confident providing follow-up care, with almost 80% of respondents reporting good or adequate confidence in all aspects of care. Primary care physicians were most confident in screening for recurrence (Figure 1). Figure 2 shows that areas with the highest frequency of low confidence responses from PCPs were providing family counseling (24%), managing lymphedema (24%), and providing sex and body image counseling (26%).
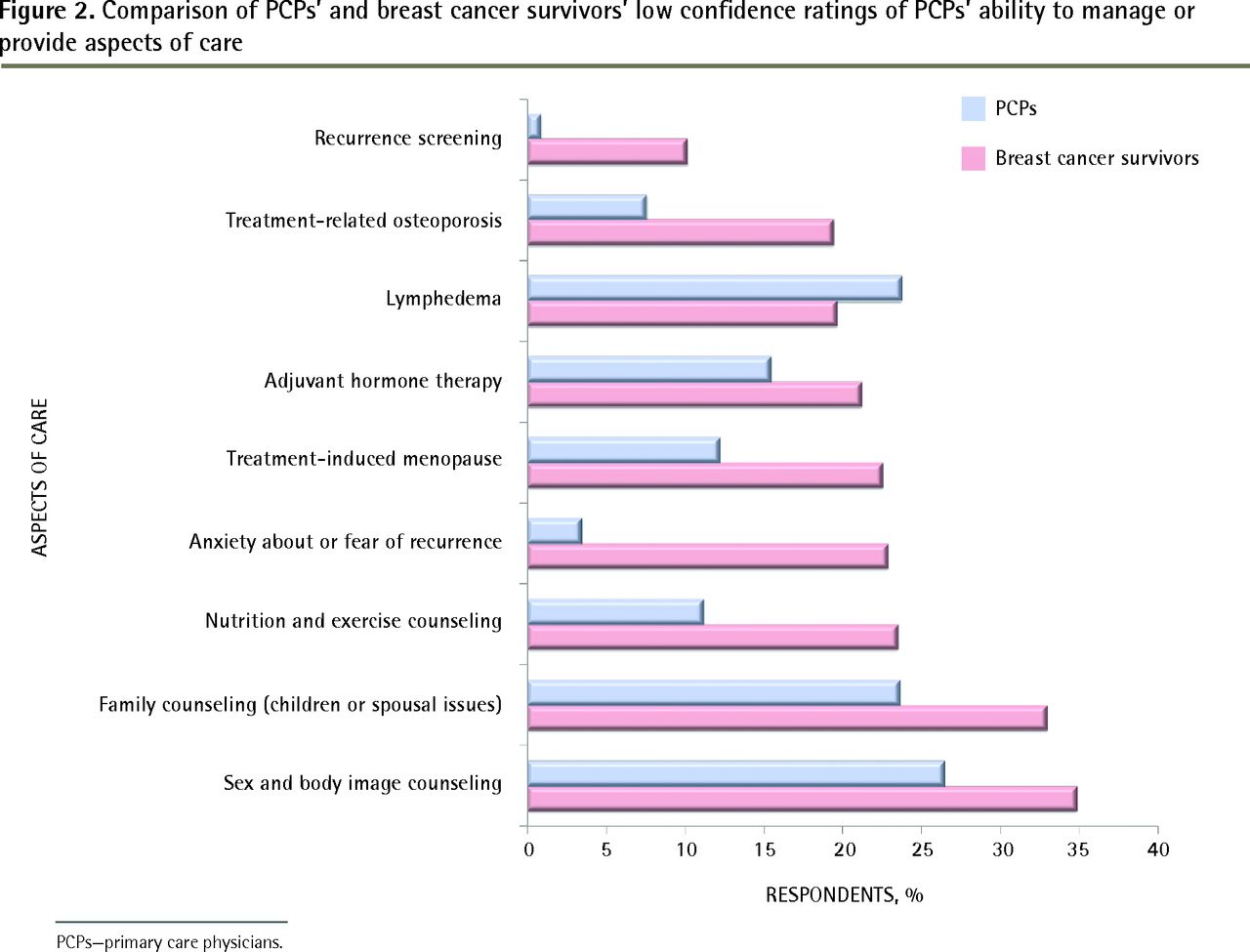
Comparison of PCPs’ and breast cancer survivors’ low confidence ratings of PCPs’ ability to manage or provide aspects of care
PCPs—primary care physicians.
Breast cancer survivors were fairly confident in all domains of follow-up, but less so than PCPs were. Similar to the physician responses, breast cancer survivors were most confident in PCPs’ ability to screen for recurrence (Figure 1). Rates of low confidence were higher in breast cancer survivors’ responses in all aspects of care except lymphedema (Figure 2). The highest rates of low confidence for breast cancer survivors were in PCPs’ ability to provide psychosocial aspects of care, such as family counseling or sex and body image counseling.
DISCUSSION
In our study, breast cancer survivors and PCPs were most confident in PCPs’ ability to screen for recurrence. This finding is reassuring given that there is randomized trial evidence showing PCP follow-up is a reasonable alternative to oncologist follow-up and results in no difference in recurrence detection rates.21
The finding that most PCPs and breast cancer survivors in our survey had good or adequate confidence levels in PCPs’ ability to provide cancer-specific care is encouraging. Some studies have suggested that patients believe PCPs lack expertise needed to deliver cancer-specific follow-up.3,11,20,24 None of these studies discusses the specific procedure used when transitioning from specialist to PCP care. Without proper communication, breast cancer survivors might feel abandoned3 or perceive their specialist- and PCP-led care as distinct entities.11 Furthermore, inadequate communication leaves PCPs unsure about whether they or the specialists are responsible for follow-up care.20 The difference between our study results and others might, in part, be related to communication with patients at the time of discharge from specialist care, or be related to the communication between the oncologist and the PCP during the transfer of care.
Previous analysis illustrated that PCPs who followed more breast cancer survivors had higher confidence levels in managing physical aspects of follow-up care such as menopausal symptoms, endocrine therapy, osteoporosis, and lymphedema, and in providing counseling about nutrition and exercise.36 More breast cancer survivors had lower confidence levels than PCPs did in PCPs’ ability to manage the “physical” aspects of care including treatment-related osteoporosis, menopause, and adjuvant hormonal therapy, with the exception of lymphedema. The reason for patients’ lower confidence in PCP-led follow-up for physical aspects of care is unclear but might be owing to different expectations between patients and physicians, or communication issues.24,26
Primary care physicians play important roles in identifying and managing lymphedema with strategies for pain control and self-care techniques,37 and referral to allied health care professionals.38,39 The present findings demonstrate that some PCPs feel inadequately prepared to deliver this care, possibly reflecting less experience among PCPs in lymphedema management, decreased incidence of clinically significant lymphedema (with the shift away from axillary node dissections to more sentinel node procedures), insufficient training in identification and management of lymphedema, or inadequate interdisciplinary communication with physiotherapists. Primary care physicians are better informed and more likely to properly manage lymphedema if educational materials are received.40 However, written guidelines and other forms of indirect education, although evidentially helpful, cannot replace practical experience.25
Both breast cancer survivors and PCPs were most likely to indicate low confidence in PCPs’ ability to provide psychosocial aspects of care, such as sex and body image counseling and family counseling. Counseling has been shown to be PCP-dependent regarding content, quality, and frequency,41 and the approach greatly affects whether patients feel well cared for.30 Similar to lymphedema management, PCPs might have less training in psychosocial domains. Studies acknowledge that PCPs play an important role in psychosocial counseling14,42 but face barriers in providing breast cancer survivors with this support,11,18,33,34 such as lack of reimbursement and time limitations. There is evidence that delivery of adequate counseling takes longer than medically focused visits,34 and PCPs who are aware of this time issue might feel less confident providing effective care during brief follow-up visits.
Patient concerns might be neglected if there is uncertainty about who should initiate discussion.15,16 Breast cancer survivors can have difficulty in sharing problems with their providers,22 which makes physician-led discussions essential.29 If patients are reluctant to ask for help, and their needs remain unaddressed, they might feel unsatisfied with care.18 Some studies show that patients prefer care providers familiar with their cancer history and who have been actively present during their cancer journey.20,28 Thus, confidence of PCPs and breast cancer survivors in psychosocial aspects of PCP-led follow-up might be improved with better physician education on breast cancer survivors’ psychosocial needs, increased interaction between breast cancer survivors and PCPs before discharge from active treatment, and by advocating for the integral role of PCPs in cancer-related counseling to ensure appropriate resources (time and reimbursement) to provide this component of care.
Limitations
Some limitations of this study include that the surveys were designed locally; and while the surveys were assessed to be accurate and reliable for small groups, they are not rigorously validated survey instruments. There is also potential selection bias, as breast cancer survivors and PCPs with strong opinions about the topic might have been more likely to participate. Because the survey data from PCPs were anonymous, it is unknown if physician demographic characteristics differentially affected reported confidence in some aspects of PCP-led follow-up care. The lack of information about PCPs might conversely be seen a strength, providing a broader look at the PCP population.
Conclusion
In British Columbia, where PCP follow-up in the survivorship stage for breast cancer survivors is the most common model of care, most PCPs and breast cancer survivors are reasonably confident in PCPs’ ability to provide effective follow-up care. The highest rates of low confidence among breast cancer survivors and PCPs in psychosocial issues might indicate areas that require further investigation and support.
Notes
EDITOR’S KEY POINTS
This study found that in British Columbia, where primary care physician (PCP) follow-up in the survivorship stage for breast cancer survivors is the most common model of care, most PCPs and breast cancer survivors are reasonably confident in PCPs’ ability to provide effective follow-up care. Breast cancer survivors and PCPs were least confident in PCPs’ ability to provide psychosocial care, such as counseling for family or sex and body image issues.
Confidence of PCPs and breast cancer survivors in PCPs’ ability to provide psychosocial care might be improved with better physician education on breast cancer survivors’ psychosocial needs, increased interaction between breast cancer survivors and PCPs before discharge from active treatment, and by advocating for the integral role of PCPs in cancer-related counseling to ensure appropriate resources (eg, time and reimbursement).
Primary care physicians expressed low confidence in their ability to manage lymphedema, possibly reflecting less experience among PCPs in this aspect of care, decreased incidence of clinically significant lymphedema, insufficient training, or inadequate interdisciplinary communication with physiotherapists.
POINTS DE REPÈRE DU RÉDACTEUR
Cette étude a révélé qu’en Colombie-Britannique, où ce sont des médecins de première ligne (MPL) qui le plus souvent sont responsables des soins aux survivantes du cancer du sein, la plupart des MPL et des survivantes du cancer étaient relativement confiants dans la capacité des MPL d’effectuer un suivi adéquat. Ces deux groupes étaient toutefois moins certains de la capacité des MPL de donner des soins de nature psychosociale, tels que le counseling des familles ou les questions relatives à l’activité sexuelle et à l’image corporelle.
Avec une meilleure formation des médecins sur les besoins des survivantes du cancer du sein, avec davantage d’interactions entre ces survivantes et les MPL avant la fin de leur traitement actif, et en préconisant une prise en charge totale des MPL dans le counseling lié au cancer de façon à s’assurer des ressources appropriées (c.-à-d. en termes de temps et de rémunération), on pourrait améliorer la confiance des MPL et des survivantes du cancer dans la capacité des MPL de prodiguer des soins de nature psychosociale.
Les MPL avaient peu de confiance en leur capacité de traiter le lymphœdème, peut-être à cause de leur peu d’expérience dans ce type de problème, de la faible incidence des lymphœdèmes cliniquement significatifs, d’un manque de formation ou d’un défaut de communication interdisciplinaire avec les physiothérapeutes.
Footnotes
This article has been peer reviewed.
Cet article fait l’objet d’une révision par des pairs.
Contributors
All authors contributed to the concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.