


Abstract
Problem addressed Despite the rapid emergence of global health training across North American universities, there remains a gap in educational programs focusing on the unique role of family medicine and primary care in global health.
Objective of program The objective of the Global Health in Family Medicine Summer Primer, developed in 2013 by the Department of Family and Community Medicine at the University of Toronto in Ontario, is to strengthen global health competencies among family medicine residents and faculty.
Program description The course covers the meaning of global health; global health ethics; the place of family medicine, primary care, and primary health care in the global health context; epidemiology; infectious diseases; the social determinants of health; and care of vulnerable populations locally and globally. The course is delivered in an intensive 5-day format with didactic lectures, group discussions, interactive workshops, and lived-experience panels.
Conclusion The Global Health in Family Medicine Summer Primer has proven to be a successful educational initiative and provides valuable lessons learned for other academic science centres in developing global health training programs for family medicine residents and faculty.
Global health education is a rapidly growing field, as increasing numbers of university students at all levels strive for competency in addressing complex health issues across international borders.1,2 In a world of increasing interdependence, highlighted by the free and rapid movement of people and goods across borders, learners in the health professions have grown acutely aware of the need to address health issues globally. Fueled by various motivating factors, learners dedicated to global health often share a commitment to improving health equity. The discipline of family medicine and the broader domain of primary care have been linked to improved health equity as well as better health outcomes and greater cost efficiency.3 While a range of programs and curricula have been developed to teach global health, we know of no other short program specifically aimed at providing an overview of key global health issues with a focus on the existing and potential role of family medicine and primary care. In response to the request of family medicine residents for more global health educational programs, and anchored in our understanding of the unique role of family medicine and primary care, the Department of Family and Community Medicine (DFCM) Global Health Program at the University of Toronto in Ontario developed a Global Health in Family Medicine Summer Primer (GHSP), which was first delivered in July 2013. This article describes the course’s objectives, curriculum, and participants, and outlines a number of key lessons learned.
Needs assessment
Because the GHSP was originally conceived as a program to enhance the global health competency of postgraduate trainees in family medicine, the GHSP team conducted a comprehensive needs assessment of this constituency. Given the breadth of global health and the goal of providing an overview while focusing on family medicine and primary care, the needs assessment sought to focus the curriculum around the expressed needs of the learners. An online survey exploring their interest and curriculum suggestions for a global health training program was sent to all family medicine residents at the University of Toronto. The content of the survey was intentionally broad, including subjects that might or might not fall directly under the usual rubric of global health but that were clearly related to addressing the health issues of marginalized or vulnerable individuals and populations. More than one-quarter (28%) of the 371 residents responded. Of these, 28% were interested and said it was likely they would attend the course if it were offered. The most common reasons for negative responses were unwillingness to use vacation time and being already engaged in the Global Health Education Initiative (a 2-year global health program offered for trainees of all specialties). Responses about preferred education methods, general approach, and course content are displayed in Tables 1 to 3.
Preferred educational methods
Preferred approach to global health education
Content preferences
When asked about their degree of interest in each of 4 core areas of global health, respondents were most interested in immigration and refugee health (preference score of 100 out of 100), low-income communities and populations in Canada (score of 91), health in lowand middle-income countries (score of 90), and indigenous and aboriginal health (score of 73). Slightly more than half of respondents (56%) indicated that their primary interest was global health abroad, while 44% were most interested in global health in Canada. Participants’ ranked reasons for their interest in global health are displayed in Figure 1. A desire to help others and personal interest were the most common responses; research interest and career advancement were least common.

Reasons for interest in global health: N = 42.
Participants in the needs assessment survey were also asked about their preferred method of evaluation. Their ranked responses can be found in Figure 2.
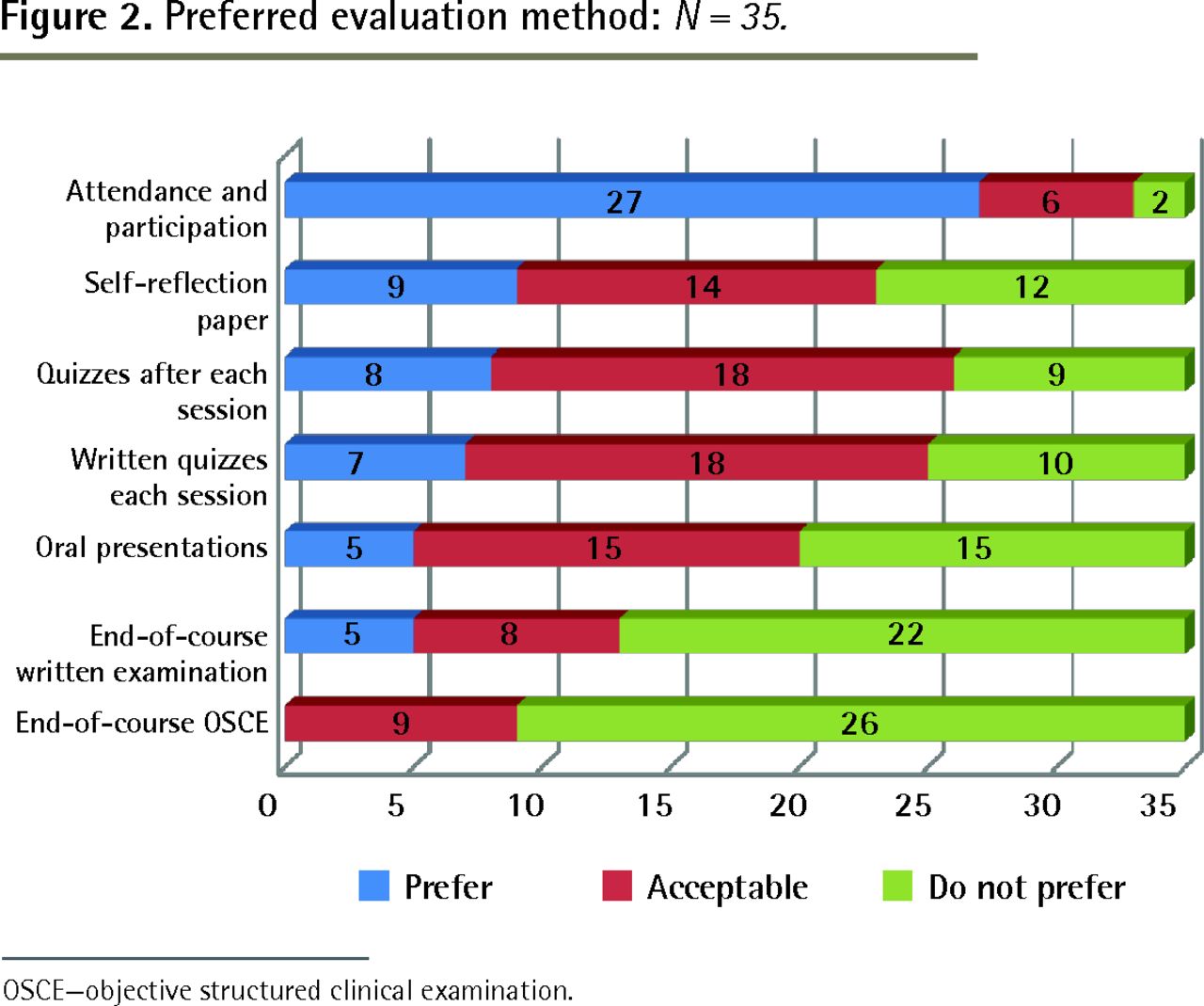
Preferred evaluation method: N = 35.
OSCE—objective structured clinical examination.
Course development and curriculum
The vision of the DFCM GHSP was to help learners understand the important role of primary care and family medicine in global health, to increase knowledge in certain key areas pertinent to global health and primary care, and to meet the expressed learning needs of potential participants. The course was developed by a core team of 4 physician leaders and 1 anthropology scholar in global health with these goals in mind. The distinguishing features of the course include its focus on primary care and family medicine, content pertinent to the care of vulnerable individuals and populations in Canada and in low- and middle-income countries, and its delivery over 1 intensive week (5 days). While the initial target learners for this course were family medicine residents, practising family physicians, mostly DFCM faculty, ultimately constituted about half of the participants. The course was clearly presented as a primer—a starting point for reflection and knowledge acquisition and an overview of some of the issues commonly encountered by family physicians working in the context of global health. It was accredited by the Office of Continuing Professional Development of the Faculty of Medicine at the University of Toronto and was eligible for continuing education credits for participants.
The curriculum was organized into 5 days, each with a theme (Table 4). It was delivered through a mix of interactive didactic sessions; group and case-based, interactive workshops; and a panel of individuals with a lived experience of poverty. The first day focused on a conceptual and reflective foundation with an introduction and discussion of the concept of global health, global health ethics, primary care, and primary health care, as well as a review of the unique role of family medicine in global health. The second day focused on infectious diseases including fever in the returning traveler and the basics of HIV care globally and locally. The third day highlighted the importance of social determinants of health, their direct relevance to family medicine and global health, and innovative tools to learn and teach how to identify and address issues related to the social determinants of health through primary care and family medicine. The care of refugees and vulnerable populations was the focus of the fourth day and included presentations of lived experience by a panel. The theme of the fifth day was the integration of global health in a family medicine career, with presentations from experienced family physicians engaged in global health and a review of the notion of partnerships and capacity building. The curriculum was delivered by a mix of family medicine faculty and other specialist colleagues who were experts in the given area.
Program curriculum
Learner assessment and course evaluation
An online pretest that focused on capturing attitudes toward global health and global health ethics was filled out by participants before the start of the course. These data were used to further refine the course content and were also reflected back to participants to stimulate discussion. Written pretests and posttests focusing on global health knowledge delivered during the course were completed by the participants on days 1 and 5.
Course evaluation included daily formative evaluation discussions, daily online evaluations of presenters and session feedback, and both written and online summative course evaluations that were required in order to receive a certificate of completion.
Outcomes
Participation and attendance
A total of 18 participants attended this course, including 5 residents, 12 practising physicians, and 1 graduate student (despite efforts to limit attendance to practising clinicians). Of the 12 practising physicians who attended, 10 held faculty positions at the University of Toronto. Participants were highly engaged and attendance was exemplary.
Knowledge acquisition and effects
Participant responses on the written posttest improved by more than 20% overall from the pretest, with initially lower scoring participants increasing their performance on the final test more than initially high scorers. Participants universally reported having met their learning objectives and having increased their global health knowledge, skills, and awareness of knowledge deficits. Respondents reported that they planned to use the knowledge gained in their local practice, in teaching trainees, and for both short and extended global health practice.
Course evaluation
Overall, the course was exceptionally well received, with all participants rating diversity of topics, speakers, and formats as very good or excellent. All participants reported that the course was a good use of their time. Strengths of the course included the enthusiastic, high-quality speakers and the opportunities for different types of learning. Weaknesses included the intensity of the course, inability to cover all materials to everyone’s satisfaction, and challenging location logistics.
Discussion and lessons learned
This pilot project had a number of limitations. The relatively small number of total participants, the small number of cohorts (2), the need for trainees to take vacation time to attend the program, and the unexpected (although welcomed) participation of faculty might all have affected our findings. Nonetheless, a number of valuable lessons have emerged from this pilot project.
High-quality global health courses are in demand
The participation rate and the enthusiasm with which participants engaged in this course confirmed that there is both a need for and an interest in global health learning among family medicine residents and faculty. The framing of the curriculum to align with the specific elements of family medicine and primary care is also important to note. It is expected that a need will soon emerge for further educational opportunities around more specific or more advanced aspects of global health.
Participant diversity as a strength
The GHSP had been initially planned with family medicine residents as the primary learner group; however, the presence of residents, community family physicians, and faculty substantially enhanced the learning environment. Overall, the family medicine trainees tended to have a longstanding interest in global health, with many having had opportunities to explore the field and reflect on its core issues over the course of their training. Practising physicians, who tended to be in the mid-to-late career stage, had a deep commitment to, and knowledge of, the discipline of family medicine, and many were experienced teachers. However, their exposure to global health was generally more recent; few had had global health experiences but many were considering global health activities in the near future. In some cases this course represented their first formal engagement with the field of global health. They tended to focus on perceived knowledge gaps around the management of specific medical conditions, particularly infectious diseases. The relative depth of awareness and reflection among trainees and the openness and humility displayed by the faculty created a very rich environment for discussion and learning.
Value of networking and sharing
In keeping with the central role of experiential learning and reflection in global health learning, participants repeatedly noted the importance of networking, connecting, and sharing experience with one another as a key strength of this course. It appears that such exchanges might play an important role in the clarification of motives, in fostering self-reflection, in acquiring knowledge, and in defining one’s role in the global arena.
Increasing knowledge and shifting attitudes
The learner assessments and course evaluations demonstrated that the course resulted in increased global health knowledge among participants. However, shifts in attitude among participants were also noted. While increased knowledge was a clear expectation of learners, the less explicitly sought change in attitude is arguably most interesting. Expanding the understanding of global health from a more narrow focus on the health dimension to a broader and more complex acknowledgment of values and foundational assumptions about the world is arguably key to fully engaging in global health.3
Global health as a local issue
A number of participants, mostly practising physicians, who might have previously assumed global health to be synonymous with international health, acknowledged their relative surprise at the realization of the local relevance of global health. Leveraging interest in vulnerable populations abroad to inform approaches to vulnerable populations locally could prove particularly effective. Raising awareness, with future and practising physicians, of the local relevance of global health and equipping them with skills and community resources to better serve local vulnerable populations could become a key focus of future programming. As such, global health could become a privileged avenue to bring attention and skill to the care of those vulnerable populations in Canada, a goal frequently identified by policy makers and one of the goals of the Future of Medical Education in Canada report.4
Curriculum content and delivery
Given the breadth of global health, one of the most important challenges in designing this course was to decide on the length of the course and on the substantive content. In their evaluation, many participants noted that they would have liked more didactic sessions while also advocating for more discussion time in the future. This raises the possibility of providing additional material through readings and Web-based sessions in the future while preserving classroom time for the essential exchange, discussion, and reflection required to assimilate global health competency.
Building a global health community
Participants enjoyed the opportunities for networking and sharing during the course and were enthusiastic about continuing to interact with peers and mentors with similar interests. It was suggested that the DFCM facilitate a network or virtual community that could act as an ongoing forum for practising physicians with common interests in global health. The planning team and participants agreed that GHSP alumni could form the nucleus of such a network. First steps to maintaining and stimulating global health connections would include tracking and communicating participants’ new global health activities, initiatives, and educational offerings.
Conclusion
The GHSP was a successful educational initiative for those involved and provided valuable lessons learned for other academic health science centres in developing similar global health programming.
Notes
EDITOR’S KEY POINTS
The Global Health in Family Medicine Summer Primer is a short program specifically aimed at providing an overview of key global health issues with a focus on the existing and potential role of family medicine and primary care.
Respondents to the needs assessment were most interested in immigration and refugee health, low-income communities and populations in Canada, health in low- and middle-income countries, and indigenous and aboriginal health. Slightly more than half of respondents indicated that their primary interest was global health abroad, while 44% were most interested in global health in Canada. A desire to help others and personal interest were the most common reasons for interest in global health.
This pilot evaluation of the intensive 5-day primer developed based on this needs assessment found that participants demonstrated increased knowledge and shifting attitudes. The lessons learned included that high-quality global health courses are in demand, participant diversity is a strength of such courses, and covering the breadth of material is challenging. Participants saw value in networking and sharing, and suggested there was need for a network or virtual community that could act as an ongoing forum for practising physicians with common interests in global health.
POINTS DE REPÈRE DU RÉDACTEUR
Le cours d’été sur la santé mondiale dans le contexte de la médecine familiale intitulé Global Health in Family Medicine Summer Primer est un programme intensif qui survole les grands enjeux de la santé mondiale, et surtout le rôle actuel et éventuel de la médecine familiale et des soins primaires.
Les répondants à l’évaluation des besoins s’intéressaient surtout à l’immigration et à la santé des réfugiés, des communautés et des populations à faible revenu au Canada, des pays à faible revenu et à revenu intermédiaire, et des populations autochtones. Un peu plus de la moitié des répondants ont indiqué que leur principal intérêt était la santé mondiale à l’étranger, tandis que 44 % s’intéressait particulièrement à la santé mondiale au Canada. Le désir d’iaider les autres et l’intérêt personnel étaient les raisons les plus courantes de l’intérêt pour la santé mondiale.
Les résultats de l’évaluation pilote de ce cours d’introduction intensif de cinq jours mis au point suivant l’évaluation des besoins indiquent de meilleures connaissances et un changement d’attitude chez les participants. Parmi les leçons apprises, on a noté que les cours de haute qualité en santé mondiale sont très recherchés, que la diversité des participants est une force, et qu’il est difficile de couvrir toute la portée du matériel. Les participants ont apprécié l’importance de tisser des liens et d’échanger, et ont suggéré qu’un réseau ou une communauté virtuelle pourrait servir de forum permanent pour les médecins ayant des intérêts communs en santé mondiale.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
All authors contributed to the concept and design of the program; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.