


Case description
Mr B., an 82-year-old man, presented to the emergency department with a history of coughing and wheezing for 2 weeks without fever or chills. He was afebrile, with a normal white blood cell count and differential. A chest x-ray scan showed patchy perihilar and right basal opacity (Figure 1). Mr B. was admitted with a diagnosis of community-acquired pneumonia. Past medical history included a myocardial infarction, hypertension, and well controlled type 2 diabetes. His serum procalcitonin levels were normal. He improved clinically and was discharged with a diagnosis of presumed viral pneumonia.
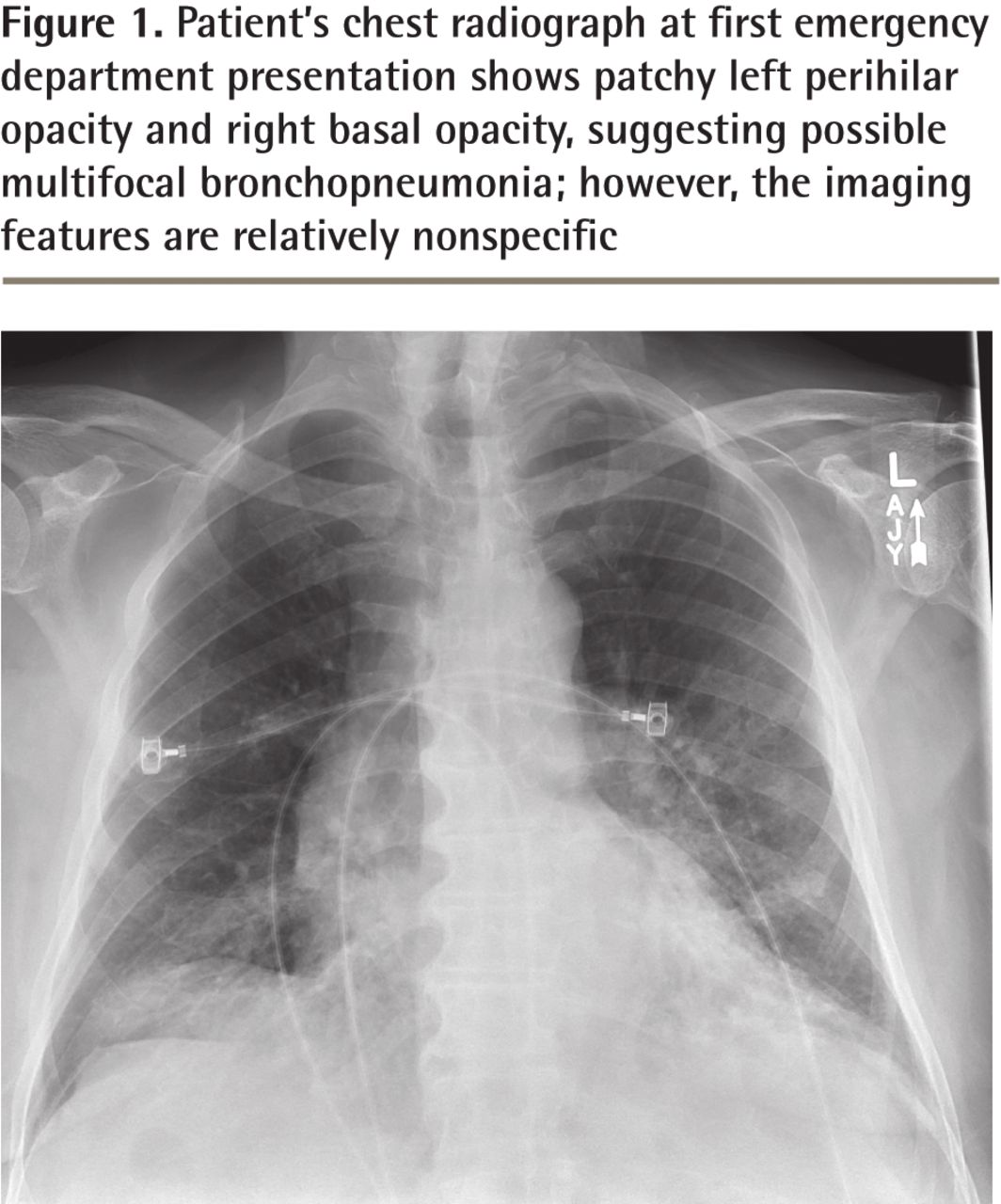
Patient’s chest radiograph at first emergency department presentation shows patchy left perihilar opacity and right basal opacity, suggesting possible multifocal bronchopneumonia; however, the imaging features are relatively nonspecific
Nine months later, Mr B. was re-admitted, again with a diagnosis of community-acquired pneumonia. He had a history of cough, fatigue, and some confusion during the previous 2 weeks, but no fever or chills. He was again afebrile, with a normal white blood cell count and differential. New medical history included a pacemaker insertion 2 months previously for bradycardia noted at cardiac rehabilitation. A chest x-ray scan showed bibasilar airspace disease, with greater perihilar opacity on the left side than the right side (Figure 2). Mr B. improved and was discharged home to complete a 5-day course of levofloxacin for presumed bacterial pneumonia.
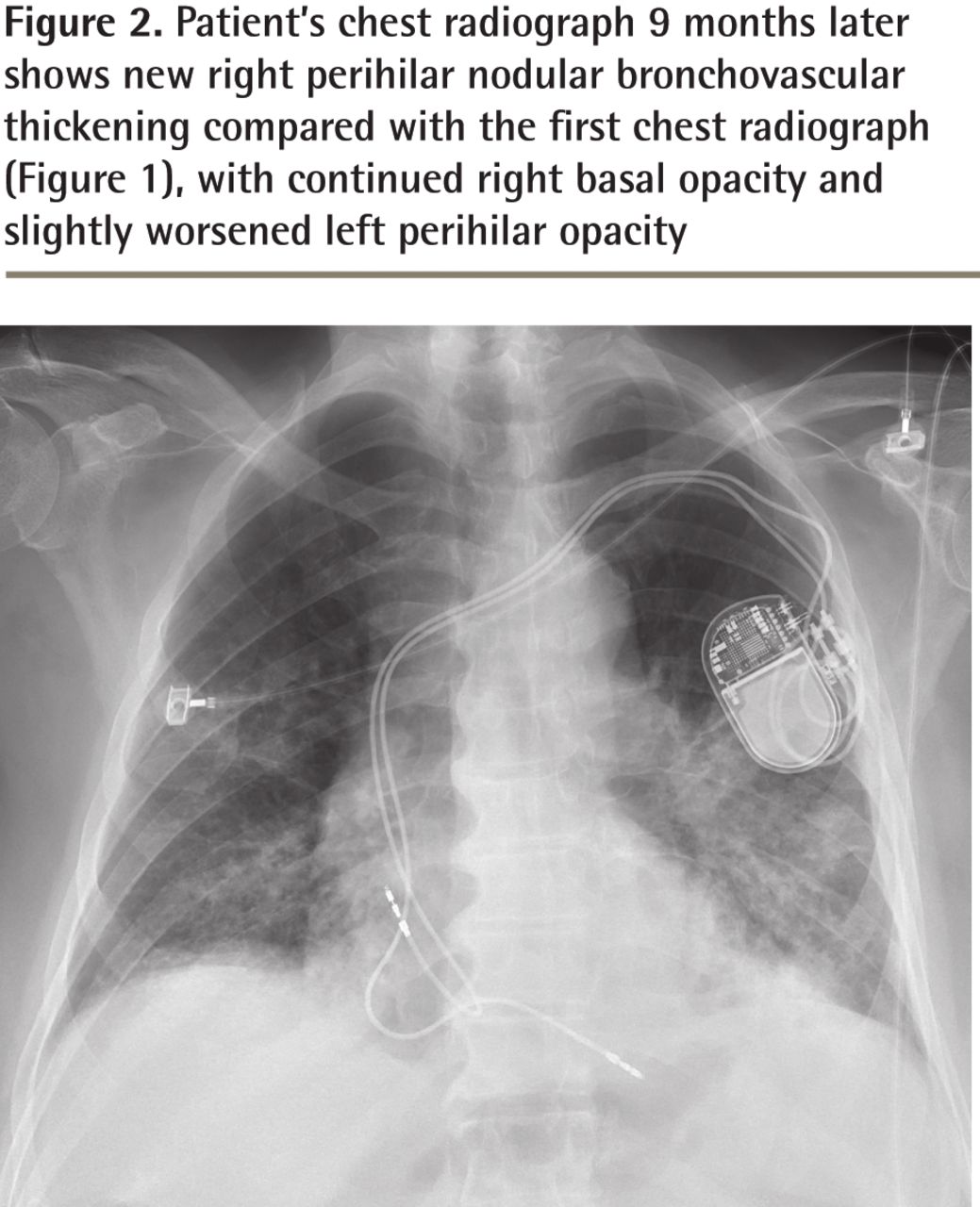
Patient’s chest radiograph 9 months later shows new right perihilar nodular bronchovascular thickening compared with the first chest radiograph (Figure 1), with continued right basal opacity and slightly worsened left perihilar opacity
A computed tomographic (CT) scan of the chest was ordered during a follow-up visit owing to persistent cough and changes on the chest x-ray scan. The CT scan revealed patchy, irregular consolidation with multifocal ground-glass opacities, septal thickening, and visualized fat densities on the lower lobes—more evident on the left lower lobe than on the right—most consistent with lipoid pneumonia (Figure 3). Upon questioning, Mr B. reported that he took a tablespoon of mineral oil each evening for a couple of weeks whenever his chronic constipation would worsen. He had done this many times during the past year, but he could not recall the exact dates. He also described a history of intermittent heartburn. Mr B. was advised to stop mineral oil ingestion immediately. Six week later, he reported that his chronic annoying cough had resolved. Of note, the medication list obtained in the outpatient office, as well as the hospital, included omeprazole as needed but not mineral oil.

Computed tomography of chest at patient’s follow-up visit: Axial unenhanced thoracic computed tomography in lung (A–C) and soft tissue (D–F) windows show multifocal, bilateral, patchy areas of dependent ground-glass opacity and peribronchial consolidation. Soft tissue images show several foci of low attenuation consolidation consistent with fat (arrowheads). Compare attenuation of these regions with fat attenuation in the chest wall (F).
*Chest wall.
Differential diagnosis
Cough with basilar infiltrates in elderly patients has a wide differential diagnosis, including bacterial pneumonia, viral pneumonia, congestive heart failure, pulmonary fibrosis, and aspiration pneumonia. Lipoid pneumonia is a form of aspiration pneumonia related to ingestion of oil.
Discussion
Exogenous lipoid pneumonia is a well described entity caused by ingestion and aspiration of lipid material, most commonly mineral oil. Lipoid pneumonia occurs mostly in the elderly and in children with developmental disabilities, presumably because these groups are more prone to aspiration.1 The pneumonitis is a foreign body reaction that causes cough, dyspnea, and often fever. Hemoptysis has also been reported.2 Radiographic features of lipoid pneumonia on chest CT scan are well described,3 and the largest series included 35 children and 18 adults.4 Radiographic findings are more common in the dependent parts of the lungs (lower lobes) and are often bilateral, with patchy consolidation, a ground-glass appearance, and septal thickening. Treatment of lipoid pneumonia is largely supportive after cessation of the inciting agent. Segmental lung lavage has been described in case reports for severe aspiration,5 but there are no clinical trials to evaluate the risks versus benefits. Steroids were used to treat acute mineral oil aspiration pneumonias in one Chinese case series,6 but the value of steroid treatment has not been established. Lipoid pneumonia is often mild and does not appear to progress if the causative agent is stopped.7 The true incidence of lipoid pneumonia is unknown, but clinical diagnosis is uncommon. Mineral oil use should be discouraged, especially among people at risk of aspiration, including the elderly and people with gastroesophageal reflux, dysphagia, or neurologic disease. Water-soluble osmotic laxatives such as polyethylene glycol 3350 or magnesium hydroxide are safer alternatives for treating constipation in such patients. Patients should be specifically asked about their use of over-the-counter medications (eg, laxatives), including those medications used on an as-needed basis. Elderly patients with basilar or aspiration pneumonia should be asked about mineral oil ingestion.
Conclusion
Lipoid pneumonia is a pneumonitis that occurs after aspiration of oils such as mineral oil, castor oil, or shark liver oil. Many family physicians are not familiar with lipoid pneumonia, hence it is likely underdiagnosed. Increased awareness could help with prevention efforts, as well as diagnosis.
Acknowledgments
I thank radiologist Dr Michael B. Gotway for noting the unusual findings on the patient’s computed tomographic scan and for providing assistance with the clinical images.
Notes
EDITOR’S KEY POINTS
Lipoid pneumonia is a form of aspiration pneumonia related to ingestion of oil. It occurs most commonly in the elderly and in children with developmental disabilities.
Mineral oil should not be used as a laxative in elderly patients or any patients who have swallowing difficulty. Water-soluble osmotic laxatives such as polyethylene glycol 3350 or magnesium hydroxide are safer alternatives.
Patients should be specifically asked about their use of over-the-counter medications (eg, laxatives), including those medications used on an as-needed basis. Elderly patients with basilar or aspiration pneumonia should be asked about mineral oil ingestion.
Computed tomography findings are generally diagnostic for lipoid pneumonia.
POINTS DE REPÈRE DU RÉDACTEUR
La pneumonie lipidique est une forme de pneumonie de déglutition associée à l’ingestion d’huile. Elle se produit le plus fréquemment chez les personnes âgées et les enfants ayant des déficiences développementales.
L’huile minérale ne devrait pas être utilisée comme laxatif chez les patients âgés ni chez ceux qui ont des problèmes de déglutition. Les laxatifs osmotiques solubles dans l’eau comme le polyéthylène glycol 3350 ou l’hydroxyde de magnésium sont des solutions de rechange plus sécuritaires.
On devrait spécifiquement demander aux patients s’ils utilisent des médicaments en vente libre (p. ex. des laxatifs), y compris ceux seulement pris au besoin. Il faudrait demander aux patients âgés souffrant de pneumonie basale ou de déglutition s’ils ont ingéré de l’huile minérale.
Les constatations à la tomodensitométrie servent habituellement à diagnostiquer la pneumonie lipidique.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.