


Abstract
Objective To describe the management and distribution of drug samples in family medicine teaching units (FMUs).
Design Cross-sectional descriptive study.
Setting All 16 FMUs affiliated with the Department of Family Medicine and Emergency Medicine at the University of Montreal in Quebec.
Participants Health care professionals (physicians, residents, pharmacists, and nurses) who manage (n = 22) and dispense (n = 294) drug samples in the FMUs.
Methods Data were collected between February and March 2013 using 2 self-administered questionnaires completed by health care professionals who manage or dispense drug samples. The data were subjected to descriptive and bivariate analyses.
Results The participation rate was 100.0% for staff who manage drug samples and 72.5% for those who dispense them. Of the 16 participating FMUs, 12 have drug sample cabinets. Eight of the FMUs have a written institutional policy governing the management of drug samples. Of the 76.2% of respondents who said they distributed samples, more than half did not know whether their institution had a policy. In 7 of 12 FMUs with drug sample cabinets, access to samples is not restricted to those authorized to prescribe medications. Cabinets are most often managed by nurses (9 of 12 FMUs). Only 4 of 12 FMUs take regular inventory of cabinet contents. The main reasons cited for dispensing samples were to help a patient financially and to test for tolerance and efficacy when initiating or modifying a treatment for a patient. Three-quarters (78.2%) of dispensers reported that sometimes they were unable to find the drug they wanted in the cabinet; half of those consequently gave patients drugs that were not their first choice. More than half the dispensers reported they never or only occasionally referred patients to their community pharmacists.
Conclusion A portrait of drug sample management and dispensation in the academic FMUs emerged from this study. This study provides insight into current practice and lays the groundwork for the development of guidelines for safe and ethical handling of drug samples.
Pharmaceutical companies use drug samples as a promotional tool.1 Physicians and health care professionals in public health care institutions are usually given samples directly, without the pharmacy department’s involvement.2,3 As a result, family physicians in training are potentially exposed to suboptimal medication management practices.
Although the distribution of drug samples has some benefits, it also poses potential health risks.4–6 Potential problems resulting from suboptimal sample management and distribution are discontinuity of treatments initiated with samples, exclusion of community pharmacists, inadequate monitoring of expiry dates, lack of documentation in patients’ charts, and lack of provision of appropriate drug information to patients. Providing patients with samples might also result in higher costs to the health care system, as it can cultivate the habit of prescribing more expensive, patented drugs.7 A recent meta-analysis showed that when physicians dispense samples to initiate a treatment, they tend to prescribe the patented drugs to continue it.8
The availability of drug samples in family medicine teaching units (FMUs), where health care professionals are trained and where they develop their clinical competencies, raises a number of important issues.
The objective of this article is to describe how drug samples are managed and dispensed in the FMUs of the Department of Family Medicine and Emergency Medicine at the University of Montreal in Quebec.
METHODS
A review of the literature revealed no theoretical framework describing the trajectory of drug samples in FMUs (how they enter, how they are stored, and how they exit). Therefore, the first phase of the present study involved mapping the process, from the drug samples’ arrival at the clinic to their distribution to patients (Figure 1). For each step, the elements, issues, and people involved were identified.

Trajectory of drug samples in the FMUs
FMU—family medicine teaching unit.
Study design and population
A cross-sectional descriptive study was conducted in all 16 FMUs affiliated with the Réseau de recherche en soins primaires de l’Université de Montréal, the Department of Family Medicine and Emergency Medicine practice-based research network.
The study population comprised all personnel who managed or dispensed drug samples in the participating FMUs. Health care professionals who had been with the FMU for less than 1 month were excluded from the study.
Instruments
Two self-administered, multiple-choice questionnaires were developed for this study. The first was intended for personnel responsible for managing samples (managers) and dealt with sample management policy: the selection, procurement, and storage of samples, and procedures for taking inventory, checking expiry dates, and disposing of expired samples. The second questionnaire was intended for those who dispensed samples (dispensers) and surveyed their knowledge about sample management policy and addressed various aspects pertaining to sample distribution, as well as relationships with pharmaceutical representatives.
A group comprising physicians, pharmacists, sample managers, and family medicine residents pretested both questionnaires. The questionnaires took an average of 15 minutes to complete. A few minor problems with the questionnaires were detected during their validation and they were subsequently revised.
Data collection procedures
Data collection was conducted between February and March 2013. A designated person from each participating FMU drew up the list of eligible personnel, presented the research project and solicited participants, distributed the questionnaires, and followed up with the participants in accordance with a procedure preestablished by the researchers. The questionnaires were completed anonymously, picked up by the designated person, and returned to the project coordinator. In the FMUs where no samples were stored or distributed (n = 4), only the questionnaire for sample managers was distributed and completed.
Data analysis
Descriptive, bivariate statistical analyses were performed using SPSS software. The study was approved by the research ethics boards of the University of Montreal (Comité d’éthique de la recherche en santé) and the Centre de santé et de services sociaux de Laval (Comité scientifique et d’éthique de la recherche).
RESULTS
In all, 22 sample managers and 294 dispensers participated in the study. The response rates were 100.0% and 72.5%, respectively. The respondents’ occupations are summarized in Table 1.
Respondents’ occupations according to their roles in drug sample management and dispensing
Drug sample management in the FMUs
Sample management policy
According to the drug sample managers, 8 of the 16 FMUs have written institutional policies governing the management of drug samples. In addition, 6 of 16 FMUs reported that their FMUs had general criteria for sample selection. However, no written formal documentation of these criteria exists. Most sample dispensers (178 of 224) did not know if their institutions had written sample management policies, or if their FMUs had selection guidelines (115) or a list of accepted samples (107). Almost half of respondents were not aware if a policy governing contact between residents and pharmaceutical representatives existed at their FMUs (Table 2).
Drug sample dispensers’ knowledge about sample management policies: N = 224 dispensers (who distributed drug samples in the previous 6 months) in FMUs with drug sample cabinets.
Storage
Four FMUs do not receive or dispense any drug samples. Drug samples are stored in shared cabinets in the other 12 FMUs. Samples are also kept in individual physicians’ offices in 4 of these 12 FMUs (Figure 2). Samples in the shared cabinets are organized by health issue (pain, contraception, etc) or system (gastroenterology, cardiology, psychiatry, etc) in half of the FMUs with shared cabinets (n = 6).

Presence and storage of drug samples in the FMUs
FMU—family medicine teaching unit.
Access and inventory management
In 5 of 12 FMUs, the samples are kept behind a locked door. In the others, access is unrestricted and open to all FMU personnel, including clerical and cleaning staff.
A team, most often led by a nurse (9 of 12), devotes an average of 3 hours a month to sample management. Inventory of the contents of the shared cabinet is conducted at regular intervals in 4 of 12 FMUs; in 3 of these, inventory is performed by visual inspection only.
Expired samples are disposed of using 1 of 4 protocols: expired samples are sent to the hospital pharmacy (6 FMUs), returned to the issuing pharmaceutical company (4 FMUs), disposed of with biomedical waste (1 FMU), or thrown into the trash (1 FMU).
Distribution of drug samples
Overall, a large proportion of respondents (224 of 294, 76.2%) said they had provided patients with samples at least once in the previous 6 months. Within each FMU this ranged from 35.0% to 92.3%. Nearly half the sample dispensers (44.9%) reported issuing samples at a frequency of at least once a month. Oral contraceptives, analgesics (including nonsteroidal anti-inflammatory drugs), intranasal corticosteroids, antacids (including proton pump inhibitors), and ointments were the products most commonly distributed (Figure 3).
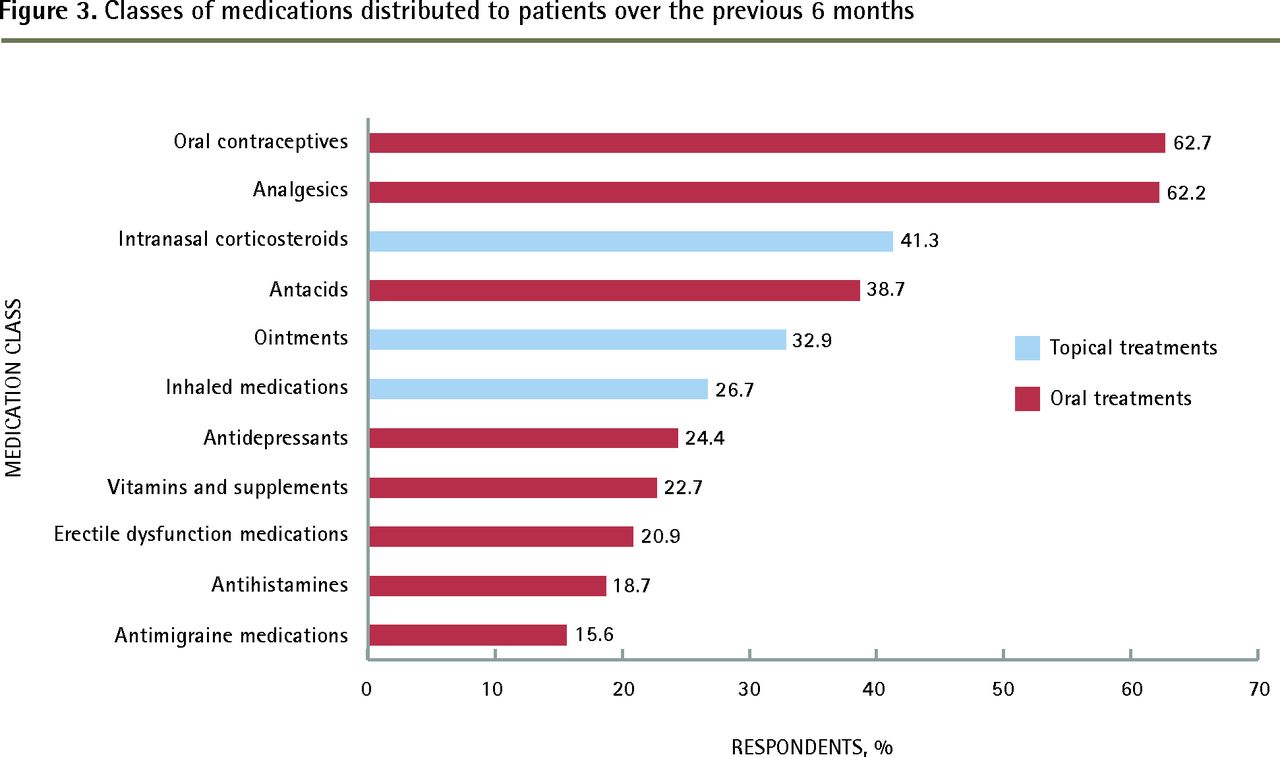
Classes of medications distributed to patients over the previous 6 months
The primary reasons cited for giving samples to patients were to help them financially, to test for tolerance and efficacy when initiating or modifying a treatment for patients, and to provide patients with relief from pain or other important symptoms (Figure 4). Other frequent reasons for using samples included facilitating adherence to treatment and initiating a treatment without delay (ie, the pharmacy was inaccessible at the time). Kindness was identified as a motivation to give samples by a few dispensers.

Primary reasons cited by respondents for dispensing drug samples to patients
Three-quarters of dispensers (78.2%) reported that sometimes they were unable to find the drug sample they wanted; 49.3% of those said that as a result they gave their patients a different medication than the one they looked for in the cabinet. They selected an alternative from the same pharmacologic class.
The percentage of dispensers wishing for access to a medication class is consistently higher than the percentage of individuals having dispensed that class during the period assessed by the study (Table 3). The difference between use and want is largest for antihistamines, antimigraine medications, and inhaled medications.
Distribution of and desire for samples by medication class: N = 224 dispensers (who distributed drug samples in the previous 6 months) in FMUs with drug sample cabinets.
While a substantial proportion of supervising physicians (67.2%) declared they documented their distribution of samples in patients’ charts, only 32.8% of residents reported they did. Figure 5 shows what information is recorded in the chart when a sample is given. More than 70% of dispensers said they documented the name, dosage, and quantity. Lot numbers were seldom recorded. More than half the respondents (57.9%) said they never or only occasionally referred patients to their community pharmacists for additional information. A higher proportion of supervising physicians (59.4%) than residents (36.0%) said they met with pharmaceutical representatives.

Frequency of dispensers’ documentation in patients’ charts upon issuing a drug sample: N = 191.
DISCUSSION
To our knowledge, this is the first Quebec study of its type conducted in settings where future family physicians are trained. Most studies deal with ethical aspects of the relationships between physicians and pharmaceutical industry representatives. Surprisingly, although drug samples are one of the industry’s top strategies for influencing physicians’ prescribing behaviour, none of the literature deals with the practical aspects of sample management and distribution in clinics. Notably, our investigation found that while all 16 FMUs adhered to the general ethical principles governing relationships between the industry and clinics, 12 reported they had a cabinet containing industry-provided samples.
Most of the FMUs studied had drug sample cabinets. However, most of the personnel who dispensed samples had no knowledge of a framework governing their procurement, distribution, and disposal. This is concerning, as a number of studies have shown that the availability of samples influences physicians’ judgment and prescribing behaviour.7 Access to drugs as samples is associated with a higher frequency of prescribing those drugs that were provided as samples.9 In addition, health care professionals’ decisions about prescriptions are often made using information provided by pharmaceutical representatives.10,11
Although the proportion of those who dispense samples is rather high, the frequency with which they do so is relatively low. The primary reasons our respondents cited for dispensing samples are clinically relevant (ie, to reduce costs for the patient, to test tolerability and efficacy, to provide immediate relief, and to foster treatment adherence). Three-quarters of sample dispensers reported that sometimes they were unable to find the medications they sought; half of those said they ended up giving their patient another drug. This supports claims about the influence of pharmaceutical companies on modifying physicians’ prescribing behaviour. Other investigators have reported similar findings.3,12 With no framework to regulate the samples stored in the clinics’ cabinets, the available samples, largely provided by pharmaceutical representatives, do not meet clinicians’ needs.12
With regard to the safe management of medications, our study reveals that in many of the FMUs, access to prescription drugs is not limited to personnel authorized to prescribe or dispense them. Samples are not always under lock and key, and in many cases no one is responsible for monitoring who accesses them. In addition, the hospital pharmacy department plays little or no role in managing the contents of the cabinets. While expired samples are generally disposed of safely, few of the FMUs conduct a systematic inventory (ie, with medication counts as in hospital pharmacies) of the cabinet contents at regular intervals.
The distribution of samples is not always documented in patients’ charts, and when it is, the entries lack important information. Additionally, more than half of the time a patient is provided a drug sample, the community pharmacist is not informed. As a result, the patient’s medication record is not up-to-date and the patient does not benefit from the community pharmacists’ expertise. This break in continuity can be especially unsafe for patients with multiple chronic conditions.
Limitations
One of the principal limitations of this study is that we did not consult patient charts to validate the data we collected. We are thus unable to confirm the rates at which samples were dispensed or what information was entered in the charts. Social desirability bias on the part of the respondents is also a possibility, although likely mitigated by the anonymity of the data collection process.
Conclusion
Our research highlights issues to take into consideration for the development of best practice guidelines for safe and ethical drug sample management and distribution. Safe medication use requires that the medication chosen is appropriate to the diagnosis, the prescription is properly recorded in the patient chart, and measures are taken so that the patient uses it optimally. Pharmacists should evaluate the treatment plan and provide counseling to the patient. The use of samples often circumvents important steps such as these and influences the prescriber’s product selection. The same standards that apply to drugs obtained through the pharmacy should apply to samples to ensure they are used appropriately, safely, and responsibly.
These results will inform the development of best practice recommendations by the College des médecins du Québec for drug sample use in medical practice.
Acknowledgments
This project received funding from the Réseau de recherche en soins primaires de l’Université de Montréal.
Notes
EDITOR’S KEY POINTS
While all 16 of the University of Montreal’s family medicine teaching units adhered to the general ethical principles governing relationships between the pharmaceutical industry and clinics, 12 reported they had a cabinet containing industry-provided samples.
Three-quarters of sample dispensers reported that sometimes they were unable to find the medications they sought; half of those said they ended up giving the patient another drug. Most of the personnel who dispensed samples had no knowledge of a framework in their institutions governing the procurement, distribution, and disposal of samples.
Safe medication use requires that the medication chosen is appropriate for the diagnosis; the prescription is properly recorded in the patient chart; and measures are taken so that the patient uses it optimally. Pharmacists should evaluate the treatment plan and provide counseling to the patient. The use of samples often circumvents important steps such as these and influences the prescriber’s product selection.
POINTS DE REPÈRE DU RÉDACTEUR
Alors que les 16 unités d’enseignement en médecine familiale à l’Université de Montréal ont toutes adopté les principes généraux d’éthique qui régissent les relations entre l’industrie pharmaceutique et les cliniques, 12 ont rapporté qu’elles disposaient d’une armoire de rangement pour les échantillons provenant de l’industrie.
Les trois-quarts de ceux qui distribuent les échantillons ont mentionné qu’ils étaient parfois incapables de retrouver les médicaments qu’ils cherchaient; la moitié d’entre eux ont dit qu’ils finissaient par administrer un autre médicament au patient. La majeure partie des membres du personnel qui distribuaient les échantillons ignoraient que leur institution avait des règles régissant leur acquisition, leur distribution et la façon d’en disposer.
L’utilisation sécuritaire d’un médicament exige que son choix soit conforme au diagnostic; que sa prescription soit correctement consignée dans le dossier du patient; et qu’on s’assure que le patient l’utilise de façon optimale. Les pharmaciens devraient aussi évaluer le plan de traitement du patient et lui donner des conseils. Souvent, l’utilisation d’échantillons ne respecte pas des étapes aussi importantes; de plus, la disponibilité des échantillons risque d’influencer le choix du produit prescrit.
Footnotes
This article has been peer reviewed.
Cet article fait l’objet d’une révision par des pairs.
Competing interests
None declared.
Contributors
Dr Lussier was primary investigator and supervised the project. All authors conceived and designed the study instruments, and contributed to the initial survey dissemination. Dr Binta Diallo oversaw and coordinated the field work (distribution of the surveys, retrieval of the surveys, and data entry) and analyzed the data. Dr Binta Diallo and Mr Gagnon contributed to the presentation of the data. Dr Binta Diallo drafted the manuscript and all authors contributed to the revision of the manuscript.
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Drug samples in family medicine teaching units: a cross-sectional descriptive study: Part 1: drug sample management policies and the relationship between the pharmaceutical industry and residents in Quebec
- Drug samples in family medicine teaching units: a cross-sectional descriptive study: Part 3: availability and use of drug samples in Quebec
- Reflective practice
- Drug samples in family medicine teaching units: a cross-sectional descriptive study: Part 2: portrait of drug sample management in Quebec