


Abstract
Objective To identify family physicians’ learning needs related to osteoporosis care; determine family physicians’ preferred modes of learning; and identify barriers to using electronic medical records (EMRs) to implement osteoporosis guidelines in practice.
Design Web-based survey.
Setting Ontario.
Participants Family physicians.
Main outcome measures Quantitative and qualitative data about learning needs related to osteoporosis diagnosis and management; preferred mode of learning about guidelines; and barriers to using EMRs to implement guidelines.
Results Of the 12 332 family physicians invited to participate in the survey, 8.5% and 7.0% provided partial or fully completed surveys, respectively. More than 80% of respondents agreed that the priority areas for education were as follows: selecting laboratory tests for secondary osteoporosis and interpreting the test results; interpreting bone mineral density results; determining appropriate circumstances for ordering anterior-posterior lumbar spine x-ray scans; and understanding duration, types, and adverse effects of pharmacotherapy. Qualitative analysis revealed that managing moderate-risk patients was a learning need. Continuing medical education was the preferred mode of learning. Approximately 80% of respondents agreed that the scarcity of EMR tools to aid in guideline implementation was a barrier to using guidelines, and 50% of respondents agreed that if EMR-embedded tools were available, time would limit their ability to use them.
Conclusion This survey identified key diagnostic- and treatment-related topics in osteoporosis care that should be the focus of future continuing professional development for family physicians. Developers of EMR tools, physicians, and researchers aiming to implement guidelines to improve osteoporosis care should consider the potential barriers indicated in this study.
Osteoporotic fractures afflict 1 in 3 women and 1 in 5 men in their lifetime.1 Fractures are associated with reduced quality of life and increased risk of death,2,3 and cost the Canadian health care system more than $3 billion annually.4 One way to reduce the burden of osteoporosis in Canada is to tackle the diagnosis and treatment care gaps to ensure that appropriate patients receive bone mineral density (BMD) tests and treatment.5 The care gap exists in part because osteoporosis guidelines, like many other clinical practice guidelines, are not used by physicians,6 perpetuating a disconnect between evidence-based recommendations for diagnosis and treatment and the care received by patients. Family physicians play an integral role in the diagnosis and management of osteoporosis.7 However, only 50% to 60% of family physicians report that they are familiar with and use clinical practice guidelines for osteoporosis8 when making diagnosis and treatment decisions.9 Reasons for less-than-optimal use of osteoporosis guidelines include their perceived complexity and the scarcity of practical tools available to assist with their use.10
Since the publication of clinical practice guidelines for osteoporosis in 2002,8 the landscape of osteoporosis care by family physicians has evolved. The 2010 osteoporosis guidelines11 emphasize the use of fracture risk assessment tools (eg, CAROC [Canadian Association of Radiologists and Osteoporosis Canada],12 FRAX [World Health Organization Fracture Risk Assessment]13), and more family physicians are using electronic medical records (EMRs)14—and there is even more EMR use expected in the future.15 Given these changes, there is a need to understand family physicians’ learning needs about osteoporosis care and how EMRs can be used to support implementation of guidelines. Therefore, the primary objective of this study was to identify family physicians’ learning needs related to osteoporosis care; the secondary objectives were to determine family physicians’ preferred learning modes, and identify barriers to using EMRs to implement the 2010 osteoporosis guidelines in practice.
METHODS
Survey design
An interdisciplinary group—comprising family physicians, non–family physician osteoporosis specialists, epidemiologists, and researchers—with quantitative and qualitative expertise designed the survey. The questions were pilot-tested by family physicians (U.M., L.N., J.K.) for question clarity and appropriateness of the answers in close-ended questions. The survey consisted of 17 close-ended and 2 open-ended questions.11 A 7-point Likert scale was used for the close-ended questions16 to determine the importance of (7 = extremely important, 6 = very important, 5 = important, 4 = moderately important, 3 = somewhat important, 2 = slightly important, 1 = not important) and agreement with (7 = strongly agree, 6 = agree, 5 = somewhat agree, 4 = undecided, 3 = somewhat disagree, 2 = disagree, 1 = strongly disagree) various statements. Where indicated, the scales were collapsed for ease of interpretation. The open-ended questions asked participants to describe learning needs and barriers to using EMRs to implement guidelines. For descriptive purposes, physicians’ sex, graduation year, practice setting, and compensation model as classified in accordance with the Ontario Ministry of Health and Long-Term Care family practice compensation models17 were collected. To understand physicians’ preferred learning modes, the professional interventions taxonomy designed by the Cochrane Effective Practice and Organization of Care group was used.18 It was not mandatory for physicians to provide an answer for each question; therefore, the number of responses for each question varies. A copy of the full questionnaire is available from the corresponding author upon request.
Data collection
From December 2013 to January 2014, the online survey was posted on a Web-based server (FluidSurveys. com, Ottawa, Ont) and links to the site were provided to all family physicians practising in Ontario. Invitations were sent via e-mail by the Ontario College of Family Physicians to all listed members (N = 12 332) with no exclusion criteria used. Two reminder e-mails were sent out to members to increase the response rate.19 Once the survey closed, participants’ names were entered into a draw for a tablet computer. The Hamilton Integrated Research Ethics Board approved this study, and participants provided informed consent to participate in the study by submitting their responses.
Analysis
The mean (SD) and frequency (percent) were computed for continuous and categorical data, respectively. Quantitative analyses were performed with SPSS version 20 (IBM Corporation). A qualitative researcher (L.L.) conducted a thematic-framework analysis for the responses to the open-ended questions. Themes and subthemes were identified using both deductive and inductive reasoning. Two analysts (L.L., S.K.) independently coded responses and discussed differences in coding to reach consensus on themes. The sample size was estimated using the sampling frame of 12 332 members of the Ontario College of Family Physicians. If 50% of all participants in the sampling frame responded to the survey and agreed (ie, somewhat agreed, agreed, or strongly agreed) that one of the most important learning needs is the duration of pharmacotherapy, and if the survey was repeated for 1054 individuals, then 95% of the time, the survey would find that between 47% and 53% of the participants in the sample would believe this learning need is important.
RESULTS
Of the 12 332 family physicians invited to participate in the survey, 1054 (8.5%) partially completed the questionnaire and 864 (7.0%) fully completed the questionnaire. Table 1 presents the descriptive characteristics of respondents. The mean (SD) number of years since graduation from medical school was 17.8 (13.6) years. Most physicians were compensated according to the blended capitation model (362 of 830 [34.3% of all respondents]). The most popular EMR vendor used was PS Suite (305 of 1054 [28.9%]). Most participants (875 of 1054 [83.0%]) were familiar with the 2010 osteoporosis guidelines.
Descriptive characteristics of study participants: N = 1054.
Learning needs
Most physicians preferred to learn about the 2010 osteoporosis guidelines through continuing medical education (CME) sessions (Figure 1). Physicians were asked about their level of agreement with the need for more education on various topics related to the diagnosis and treatment of osteoporosis (Table 2). Ratings on the Likert scale were collapsed for ease of interpretation; respondents who agreed with a statement indicating the need for education had originally answered “somewhat agree,” “agree,” or “strongly agree.” More than 80% of respondents agreed that education is needed on the types of laboratory tests to order to rule out secondary osteoporosis and how to interpret such test results, interpreting BMD results, and when to order anterior-posterior lumbar spine x-ray scans (Table 2). Almost all respondents indicated there was a need for education on the duration and adverse effects of pharmacotherapy (Table 2). The results from the open-ended questions about learning needs echo the quantitative findings (Table 3).

Family physicians’ preferred ways to learn about the 2010 osteoporosis guidelines: N = 1019.
CME—continuing medical education, EMR—electronic medical record, PBSG—problem-based small group learning.
*Other comprises paper-based handouts, online webinar, or audit and feedback.
Rank-ordered list of osteoporosis diagnosis and treatment topics for which further education would be useful
Learning needs related to osteoporosis care and barriers to guideline implementation using EMR tools that were identified with open-ended questions
Barriers
Ratings on the Likert scale were collapsed for ease of interpretation; respondents who agreed with a statement indicating barriers originally answered “somewhat agree,” “agree,” or “strongly agree.”
Barriers to using the osteoporosis guidelines.
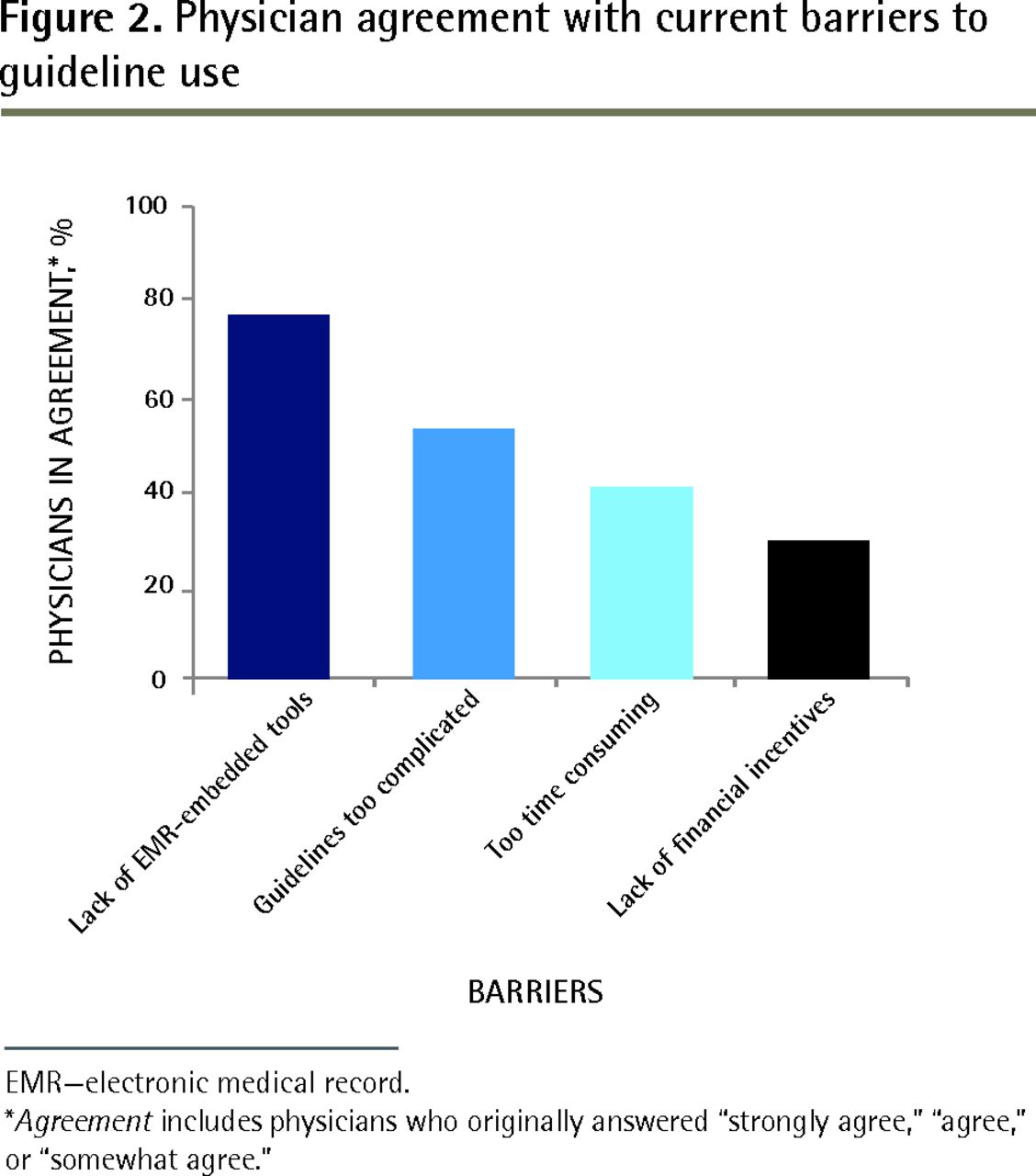
One of the main barriers to using the 2010 osteoporosis guidelines was the lack of EMR-embedded tools to help clinicians, as noted by 76.9% (732 of 952) of participants (Figure 2). Only 29.6% (275 of 928) of participants indicated that a lack of financial incentives was a barrier (Figure 2).

Physician agreement with current barriers to guideline use
EMR—electronic medical record.
*Agreement includes physicians who originally answered “strongly agree,” “agree,” or “somewhat agree.”
Barriers to using EMR-embedded tools to facilitate guideline use.
Approximately half of respondents (433 of 874 [49.5%]) agreed that time would limit their ability to use an EMR tool (Figure 3), a finding that was echoed in the qualitative analysis (Table 3). Most participants were optimistic about the potential effects of an EMR tool on patient outcomes, as most participants (532 of 849 [62.7%]) disagreed with the statement that the tool would not have an effect on patient outcomes (Figure 3). Additional barriers identified in the qualitative analysis are displayed in Table 3. When physicians were asked about their willingness to use an EMR tool, most physicians (773 of 887 [87.1%]) agreed that they would attempt to use it in practice.

Physician agreement regarding barriers to implementing osteoporosis guidelines using an EMR tool
EMR—electronic medical record.
*Agreement includes physicians who originally answered “strongly agree,” “agree,” or “somewhat agree.”
DISCUSSION
We examined family physicians’ learning needs related to the 2010 osteoporosis guidelines and barriers to using EMR-embedded tools to implement the guidelines. Priority areas for education for family physicians were as follows: selecting and interpreting laboratory tests for secondary osteoporosis; interpreting BMD reports; understanding how frequently BMD tests should be ordered; determining appropriate circumstances for ordering spine x-ray scans; and understanding types, doses, and duration of pharmacotherapies, adverse effects of treatments, and how to manage moderate-risk patients. The chief barrier to using guidelines in practice was identified to be a lack of tools embedded within EMRs to assist with the implementation of guidelines. Physicians agreed that if there were EMR-embedded tools available, a lack of time, a lack of financial incentives, tool complexity, and difficulty introducing a tool into some EMR programs would be potential barriers to use. Regardless, most physicians were interested in having an EMR tool available and believed that EMR tools might have a positive effect on patient outcomes.
Understanding the learning needs of and identifying topics clinically important to family physicians is an important step in narrowing the osteoporosis care gap in Canada.20 Regarding learning needs, many of our findings are in agreement with previously reported learning needs of family physicians in Ontario. Similar to our finding that 83.2% of physicians agreed that more education was needed on interpreting BMD reports, Jaglal and colleagues found that 66.8% of physicians were interested in learning more about interpreting T-scores from BMD reports.9 A rise in interest in this area might be due to the migration away from the more simplified diagnostic rules (ie, T-score ≤ −2.5),21 to more complex fracture risk assessment. Also, similar to Jaglal’s findings, our study revealed that family physicians are still highly interested in learning about how long patients should be prescribed pharmacotherapy, the side effects, and appropriate dosages.9 A qualitative study conducted on the management of osteoporosis by family physicians indicated that, like in our study, physicians expressed confusion about how to manage patients who were in the moderate-risk category for fracture.10 Therefore, more complex clinical cases should be presented to physicians during CME sessions, or guidelines should include more practical guidance for moderate-risk patients.
While the evidence on the effectiveness of CME for increasing knowledge, changing physicians’ behaviour, and improving patient outcomes is mixed,22 our study showed that CME remains the preferred means of education about guidelines. Although most physicians in our study preferred CME for learning about the clinical practice guidelines, various reviews suggest that multifaceted interventions are optimal, combining CME with patient and physician reminders and prompts, seminars with local opinion leaders, and other interventions in the Cochrane Effective Practice and Organization of Care group taxonomy.23,24
Whether physicians use clinical practice guidelines is dependent on a number of intrinsic and extrinsic factors.25 The strategies employed to implement the guidelines must be tailored to the learner’s needs and setting, and should involve multiple types of interventions.23,24,26 Most participants in our study expressed interest in using an EMR-embedded tool to facilitate osteoporosis guideline use. One study has evaluated whether EMR-based reminders influence osteoporosis screening and treatment rates.27 Compared with usual care, the number of patients who received a BMD test or osteoporosis treatment was 8-fold higher in the intervention group with reminders.27 Reviews on the effectiveness of computerized clinical decision support systems, including EMR tools, have suggested that these tools can have a positive effect on processes of care28 and treatment monitoring.29 However, potential barriers to using EMR tools to improve guideline use are tool complexity, a lack of time to learn and apply the tool during patient visits, and a lack of financial incentives to use the tool. These barriers are similar to general barriers around using EMRs.30
Limitations
Study limitations include our low response rate (7.0% to 8.5%), which is lower than reported for the National Physician Survey31 and other surveys involving family physicians in Ontario.9 One reason for this might be that surveys were sent out to physicians during December and January, a busy time of the year for clinicians. We recommend caution applying our findings to all family physicians in Ontario and the rest of Canada. However, a rigorously designed, administered, and analyzed cross-sectional survey on this important topic might pave the way for further discussion, research, and modifications of osteoporosis guidelines.
Conclusion
This survey identified diagnosis- and treatment-related learning needs for family physicians related to the 2010 osteoporosis guidelines. To assist physicians with clinical practice guideline implementation, EMR tool developers should be aware of the potential barriers to use, including tool complexity and lack of time and financial reimbursement for using the tool. These study findings will aid EMR tool developers, researchers, and physicians aiming to implement guidelines to improve care for those with fractures and for those at risk of fractures in Ontario.
Acknowledgments
We thank the Ontario College of Family Physicians for supporting the study and the Hamilton Health Sciences Foundation for funding part of this work.
Notes
EDITOR’S KEY POINTS
Understanding family physicians’ learning needs and identifying topics that are clinically relevant are important steps in narrowing the osteoporosis care gap in Canada. This study identified diagnosis- and treatment-related learning needs for family physicians related to the 2010 osteoporosis guidelines.
Continuing medical education remains the preferred means of learning about guidelines. Many participants expressed confusion about how to manage patients at moderate risk of fractures; more complex clinical cases should be presented during continuing medical education sessions, and guidelines should include more practical guidance for moderate-risk patients.
Most participants expressed interest in using a tool embedded in the electronic medical record to facilitate osteoporosis guideline use; however, there are several potential barriers to using such tools, including tool complexity, a lack of time to learn and apply the tool during patient visits, and a lack of financial incentives to use the tool.
POINTS DE REPÈRE DU RÉDACTEUR
Pour combler les lacunes entourant le traitement de l’ostéoporose au Canada, il est important de comprendre les besoins d’apprentissage des médecins de famille et de cerner les sujets cliniquement pertinents. Cette étude fait ressortir les besoins d’apprentissage des médecins de famille concernant le diagnostic et les traitements en relation avec les lignes directrices de 2010 sur l’ostéoporose.
La formation médicale continue demeure le moyen privilégié pour l’apprentissage des lignes directrices. De nombreux participants ont exprimé leur confusion concernant la façon de prendre en charge les patients à risque modéré de fractures; les cas cliniques plus complexes devraient être présentés lors des séances de formation médicale continue et les lignes directrices devraient offrir des conseils plus pratiques pour les patients à risque modéré.
La plupart des participants se sont dits intéressés à utiliser un outil intégré dans le dossier médical électronique pour faciliter l’application des lignes directrices sur l’ostéoporose; par ailleurs, il existe divers obstacles à l’utilisation de tels outils, notamment la complexité de l’outil, le manque de temps pour apprendre à s’en servir et l’utiliser durant les visites des patients, de même qu’un manque d’incitatifs financiers à utiliser cet outil.
Footnotes
Competing interests
Dr Mehan served as an advisory board member and received honoraria for presenting, planning, or moderating events from AstraZeneca, Amgen, Eli Lilly, Sanofi, Merck, Janssen, Lundbeck, Novo Nordisk, and Dairy Farmers of Canada. Dr Jovaisas received research funding, honoraria, and travel grants from, as well as served on advisory boards and had consulting roles for, Abbott, Altana, AstraZeneca, Amgen, Bristol-Myers Squibb, Centocor, Dimethaid, Eli Lilly, Janssen Ortho, Roche, Mentor, Merck Frosst, Novartis, Nycomed, Procter & Gamble, Pfizer, Sanofi-Aventis, Schering-Plough, Servier, Solvay, Wyeth, and UCB Pharma. Dr Cheung received Amgen grants (to the University Health Network [UHN]) and honoraria; Eli Lilly grants (to UHN) and honoraria; and Merck grants (to UHN). Dr Adachi received grants or research support, speaker’s bureau remuneration or honoraria, and consulting fees from Amgen, Eli Lilly, Merck, Actavis, and AgNovos. Dr Adachi was also the past president of Osteoporosis Canada, as well as a member of the International Osteoporosis Foundation board of directors and scientific advisory council. Dr Papaioannou received grants or research support, speaker’s bureau remuneration or honoraria, and consulting fees from Amgen, Eli Lilly, and Merck Canada.
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
All authors contributed to the concept and design of the study. Drs Papaioannou, Pritchard, Adachi, Ioannidis, Thabane, Nash, Mehan, and Feldman and Ms Karampatos contributed to the survey creation and implementation. Drs Pritchard, Ioannidis, Thabane, and Lohfeld conducted the analysis and interpretation. Dr Pritchard drafted the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual content and final approval of the article. All authors have taken care to ensure that the material in the manuscript is complete and original.
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}
{kind=link}