


Abstract
Objective To provide primary care physicians with an approach to driving safety concerns when older persons present with memory difficulties.
Sources of information The approach is based on an accredited memory clinic training program developed by the Centre for Family Medicine Primary Care Collaborative Memory Clinic.
Main message One of the most challenging aspects of dementia care is the assessment of driving safety. Drivers with dementia are at higher risk of motor vehicle collisions, yet many drivers with mild dementia might be safely able to continue driving for several years. Because safe driving is dependent on multiple cognitive and functional skills, clinicians should carefully consider many factors when determining if cognitive concerns affect driving safety. Specific findings on corroborated history and office-based cognitive testing might aid in the physician’s decisions to refer for comprehensive on-road driving evaluation and whether to notify transportation authorities in accordance with provincial reporting requirements. Sensitive communication and a person-centred approach are essential.
Conclusion Primary care physicians must consider many factors when determining if cognitive concerns might affect driving safety in older drivers.
For primary care clinicians, one of the most challenging aspects of dementia care is the assessment of driving safety.1–4 Driving is a complex task and as people age, decline in cognitive functioning might affect their ability to safely operate a motor vehicle. Drivers with dementia are overall 2.5 to 4.7 times more likely than healthy, age-matched controls to be involved in motor vehicle collisions,5 yet many persons with mild dementia can safely continue to drive for several years.6 Although a few helpful reviews have provided some guidance on dementia and driving,7–10 practical implementation has remained a challenge in the context of a busy primary care setting. While no single office-based test has cutoff scores with validated psychometric properties that would reliably allow it to be used alone to determine driving fitness in all situations,11 this does not imply that in-office tests are of no use to front-line clinicians. Decisions regarding driving safety still need to be made when assessing any person who might be cognitively impaired. Lack of knowledge about whether or not a person with dementia is driving does not protect physicians from legal consequences should that person experience an at-fault motor vehicle crash. This article focuses on a practical approach to considerations in driving safety for older persons with cognitive concerns. As outlined in the Centre for Family Medicine (CFFM) Memory Clinic clinical reasoning model, previously published in Canadian Family Physician (www.cfp.ca/content/59/3/249.full.pdf+html),12 this represents step 7 of a structured primary care approach to patients presenting with memory difficulties.
Case description
Edward is a 78-year-old retired lawyer who presents with memory difficulties during the past year. He forgets names and recent conversations. Over the past several months, his wife has noticed he has forgotten to take his medications and has required frequent reminders. He has missed several bill payments in the past year. He currently drives and neither he nor his wife have any concerns about his driving, with no reported accidents or near accidents. He has 20 years of education, is married, and has 2 children. Alcohol intake is minimal. Medical history includes hypothyroidism, gout, and hyperlipidemia, for which he takes 0.125 mg of levothyroxine once daily, 100 mg of allopurinol once daily, and 20 mg of atorvastatin once daily.
Results of cognitive screening tests administered in your office are as follows: he completes the Trail Making B test (TMT-B) in 4 minutes 7 seconds with 0 errors; his ability to complete the Trail Making A (TMT-A) test is intact; his ability to copy intersecting pentagons is intact; and his Montreal Cognitive Assessment (MoCA) score is 17 out of 30 with 0 out of 5 delayed recall, an intact cube draw, and a clock drawn with incorrect hand placement.
Is driving safety a concern? Should a comprehensive on-road driving assessment be arranged? Must his primary care physician report this to transportation authorities?
Sources of information
The approach described in this article is based on an accredited primary care memory clinic training program developed by the CFFM Primary Care Collaborative Memory Clinic, which has previously been described in detail in Canadian Family Physician.13
Main message
Safe driving is dependent on multiple cognitive and functional skills. Clinicians should carefully consider many factors when determining if cognitive concerns affect driving safety. Indeed, a recent systematic review supports the use of composite batteries, rather than individual cognitive tests, to predict driving performance,14 and other studies have suggested the same.15–18 At the CFFM Primary Care Collaborative Memory Clinic19 and in its training program,13 which has helped to develop 100 other memory clinics in Ontario, consideration is given to several specific findings on corroborated history and cognitive testing, which aid in the physician’s decisions to refer for comprehensive on-road driving evaluation and to report to transportation authorities. These include findings of impairment in daily functioning due to cognitive difficulty, as well as performance on cognitive screening tests that can be practically administered in an office-based setting. In our program, the recommended cognitive screening tests include the MoCA,20 the TMT-A and TMT-B,21 and copying 2 intersecting pentagons.22 The greater the number or severity of concerning findings, the more confident the physician is that it might be unsafe for the patient to drive. This multifaceted approach helps to ensure that cognitive test findings are interpreted in clinical context and that no single test is misused in assessing driving safety. Performance-based, comprehensive on-road driving evaluation remains the most accurate method of determining driving fitness status; however, in most provinces, high out-of-pocket expense for these comprehensive assessments poses a substantial barrier for many older people, and on-road testing is not available in all rural regions. Consequently, this might not be an equitable and realistic option for all older drivers.
Corroborated history
Assessment of driving safety begins with a careful corroborated history to obtain an accurate report of family member concerns and documentation of previous motor vehicle accidents or near accidents. This corroborated history can be obtained in the context of a full discussion with family about all medical and safety issues, with permission usually sought from the patient when discussing any issues with family. The family member should be interviewed alone, allowing for safe disclosure of any driving concerns. A history of a motor vehicle crash within the previous 2 years has been shown to be a strong predictor of future motor vehicle crashes.16 When family members do raise concerns about driving safety, they are often accurate and their concerns should be strongly considered23; however, lack of concern might not always reflect low driving risk. Drivers with dementia and their family members might not recognize decline in driving-related abilities or might underreport concerns, possibly owing to personal bias.24,25 Corroborated history can also help to determine the degree of functional impairment in instrumental and basic activities of daily living due to cognitive difficulty9,26 (Table 110) as a proxy for severity of the dementing illness. Consensus among national guidelines is that those with moderate or severe dementia should not drive; in the Canadian Medical Association guidelines,26 this is defined by a new loss of ability to perform 2 or more instrumental activities of daily living or any basic activity of daily living on the basis of cognitive difficulties.
The SHAFT and DEATH mnemonics for the instrumental and basic activities of daily living
Cognitive testing
Several international guidelines have recommended use of the TMT-B to assess driving safety. The TMT-B measures motor processing speed, executive functioning, and cognitive flexibility in switching attention between competing sets of stimuli. A systematic review concluded that there is support for using TMT-B cutoffs of 3 minutes for completion or 3 or more errors11—the 3 or 3 rule (Table 2).10 The TMT-A,27 a task that measures motor processing speed, might also be helpful in discriminating between safe and potentially unsafe cognitively impaired older drivers. A recent study demonstrated that inability to complete the Trail Making tests within a reasonable time frame (ie, TMT-A > 48 seconds, TMT-B > 108 seconds) might suggest the need for further driving evaluation.28 Both the TMT-A and TMT-B are available at www.healthcare.uiowa.edu/igec/tools/cognitive/trailMaking.pdf or www.rgpeo.com/media/53150/trails%20a%20and%20b.pdf.
Trail Making A and B test cutoff scores
Guidelines have recommended the administration of other cognitive screening tests, such as the Mini-Mental State Examination (MMSE) and the clock-drawing test. Scores on the MMSE have not been shown to be predictive of driving risk16,17 or motor vehicle crashes16 in drivers. However, impairment in the copying of the intersecting pentagon task in the MMSE, but not the MMSE score itself, has been associated with driving cessation in older adults.29 Indeed, a meta-analysis of neuropsychological tests has suggested that tests of visuospatial skills might be the most relevant to driving abilities.6 The clock-drawing test has also been shown to predict performance on a driving simulator.30 It is unfortunate that the complex methods used to score the clock-drawing test in research are rarely used in front-line clinical care, where the gestalt approach of dichotomizing results into good or bad is usually used. Further research is required to develop scoring methods that are feasible in the context of busy clinical practice and that are correlated with crash risk. Recently, a study17 demonstrated that in cognitively impaired older adults, the MoCA20 score might have better predictive value for driving outcome than that of the MMSE. In that study, a MoCA score of 18 or less in cognitively impaired individuals was associated with greater likelihood of failing an on-road driving assessment, although its predictive ability was not strong enough to recommend its use as the sole instrument for identifying unfit drivers.17
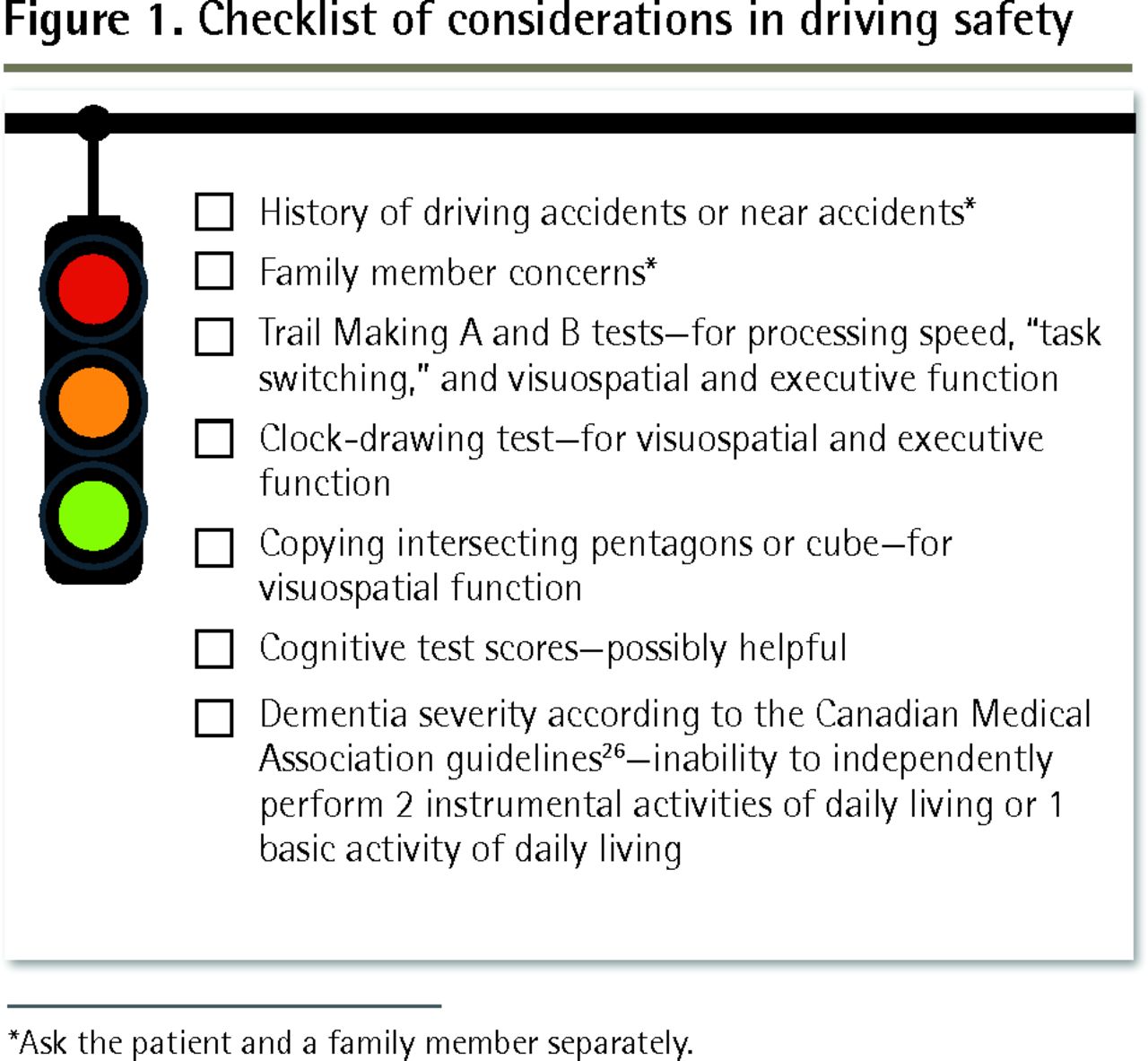
Figure 1 summarizes the corroborated history and cognitive testing elements that might aid in a physician’s decisions to refer for comprehensive on-road driving evaluation and to report to transportation authorities in accordance with provincial requirements.26 The greater the number and the greater the severity of worrisome findings, the more concerned the physician should be that the patient might be at higher risk of a motor vehicle crash. Reporting to transportation authorities might be warranted, as is discussion of the option to arrange for a comprehensive on-road driving evaluation as the fairest means of determining driving safety. It should be noted that factors other than cognition might affect driving safety and must also be considered in the assessment of any older driver. These can include the presence of physical limitations, visual impairment, excessive alcohol consumption, and other comorbid conditions; these are described in detail elsewhere.8,26
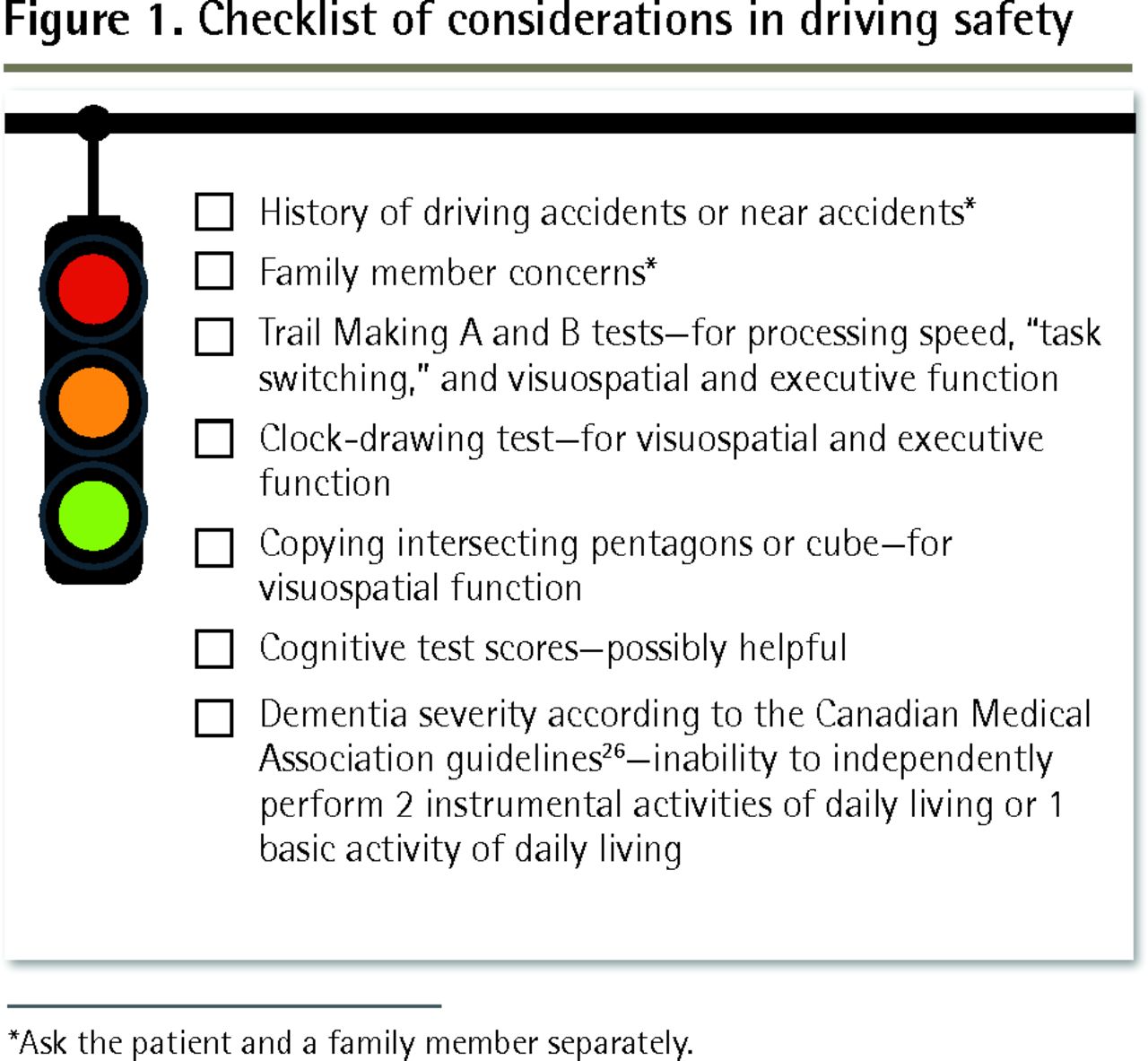
Checklist of considerations in driving safety
*Ask the patient and a family member separately.
Communication and follow-up
Physicians in most Canadian jurisdictions are legally mandated to report medical findings that could affect fitness to drive. Even in provinces with discretionary reporting, Canadian guidelines26 recommend that physicians err on the side of reporting any potentially medically unfit driver to permit transportation authorities to investigate further and to prevent potentially avoidable patient, caregiver, and bystander morbidity and mortality. However, reporting to transportation authorities might compromise the physician-patient relationship31,32 and is identified as an important barrier to care2,4 for front-line clinicians. In disclosing concerns about driving safety to the person with dementia and their family members, the need for tactful communication and sensitivity cannot be overstated. Dementia is a progressive, terminal illness associated with feelings of shame, rejection, social isolation, and loss of a sense of control.33 Driving discussions are emotionally charged because the ability to drive is associated with independence and personal identity.34 Loss of driving ability has been associated with social isolation35 and an almost doubled risk of depressive symptoms.36 A person-centred approach37 is essential, considering the perspectives and needs of the individual and exploring transportation alternatives that might help the person to maintain mobility and social functioning.
For persons with mild dementia who are still able to drive, guidelines recommend regular reassessment of driving safety every 6 to 9 months.26 Ideally, for all persons with a diagnosis of dementia there should be early discussion of the eventual need to stop driving. Communication that occurs over time allows older persons the opportunity to reflect on the process of driving retirement and to plan for transportation alternatives.34 Resources to assist with this discussion and planning are available in the Driving and Dementia Toolkit for Patients and Caregivers (www.rgpeo.com/media/30422/d%20%20d%20toolkit%20pt%20crgvr%20eng%20with%20hyperlinks.pdf) and the Driving and Dementia Toolkit for Health Professionals (www.rgpeo.com/media/30695/dementia%20toolkit.pdf).38,39 Primary care physicians are uniquely positioned to have trusting, sensitive conversations with their older patients about driving safety concerns and the need for future transition to alternate forms of transportation.34
Future research should be directed to the challenging area of assessing driving safety in persons with mild cognitive impairment,40 as well as to the development of a composite battery of office-based tests with valid, usable cutoff scores that reliably screen for driving safety in cognitively impaired persons that can be feasibly administered in the clinical primary care setting.14 Until then, clinicians must continue to consider many factors when determining if cognitive concerns affect driving safety, balancing the need to respect individual autonomy with maintaining patient and public safety.
Case resolution
Working through the CFFM Memory Clinic clinical reasoning model approach,12 a diagnosis of probable Alzheimer dementia is made. Considerations regarding driving safety include Edward’s slow time to complete the TMT-B test, his impaired clock-drawing ability, and identification of functional impairment due to cognitive difficulties in 2 instrumental activities of daily living (managing medications and paying bills). Given these considerations, driving safety is a concern. A comprehensive on-road driving evaluation is recommended as the fairest way of determining fitness to drive, and Edward is advised not to drive until an on-road driving evaluation confirms his fitness to drive. Also, the option to “retire” from driving and local transportation alternatives are discussed. Notification is sent to provincial transportation authorities advising that driving safety concerns have been identified and that a comprehensive on-road driving evaluation has been recommended to determine fitness to drive.
Conclusion
One of the most challenging aspects of dementia care is the assessment of driving safety. Because safe driving is dependent on multiple cognitive and functional skills, physicians must carefully consider many factors when determining if cognitive concerns affect driving safety in the older driver. Specific findings on corroborated history and office-based cognitive testing might aid in this assessment. Sensitive conversations about driving safety concerns are essential, considering the needs of the individual to maintain mobility and social functioning while maintaining patient and public safety.
Notes
EDITOR’S KEY POINTS
Assessing driving safety in patients with cognitive impairment represents a considerable challenge in the busy primary care setting. On-road testing remains the most accurate way of determining fitness to drive, but such testing can be prohibitively expensive and it is not available in all areas. This article focuses on a practical in-office approach to considerations in driving safety for older patients with cognitive concerns.
There is no single office-based test that can reliably be used alone to determine whether it is safe for a patient with cognitive impairment to drive. Evidence suggests that the use of composite batteries, rather than individual cognitive tests, might be more useful. The accredited Centre for Family Medicine Primary Care Collaborative Memory Clinic training program considers specific findings on corroborated history and cognitive testing in assessing driving safety.
This multifaceted approach helps to ensure that cognitive test findings are interpreted in clinical context and that no single test is misused in assessing driving safety.
Footnotes
This article is eligible for Mainpro+ certified Self-Learning credits. To earn credits, go to www.cfp.ca and click on the Mainpro+ link.
This article has been peer reviewed.
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro de janvier 2017 à la page e9.
Contributors
Both authors contributed to the literature review and interpretation, and to preparing the manuscript for submission.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Everyday Driving and Plasma Biomarkers in Alzheimers Disease: Leveraging Artificial Intelligence to Expand Our Diagnostic Toolkit
- Top 10 Self Learning articles from 2017
- Roles des medecins de famille dans les soins lies a la demence
- Driving assessment for people with dementia
- Evaluation de laptitude a conduire chez les personnes atteintes de demence
- Role of the family physician in dementia care