


Article Figures & Data
Figures
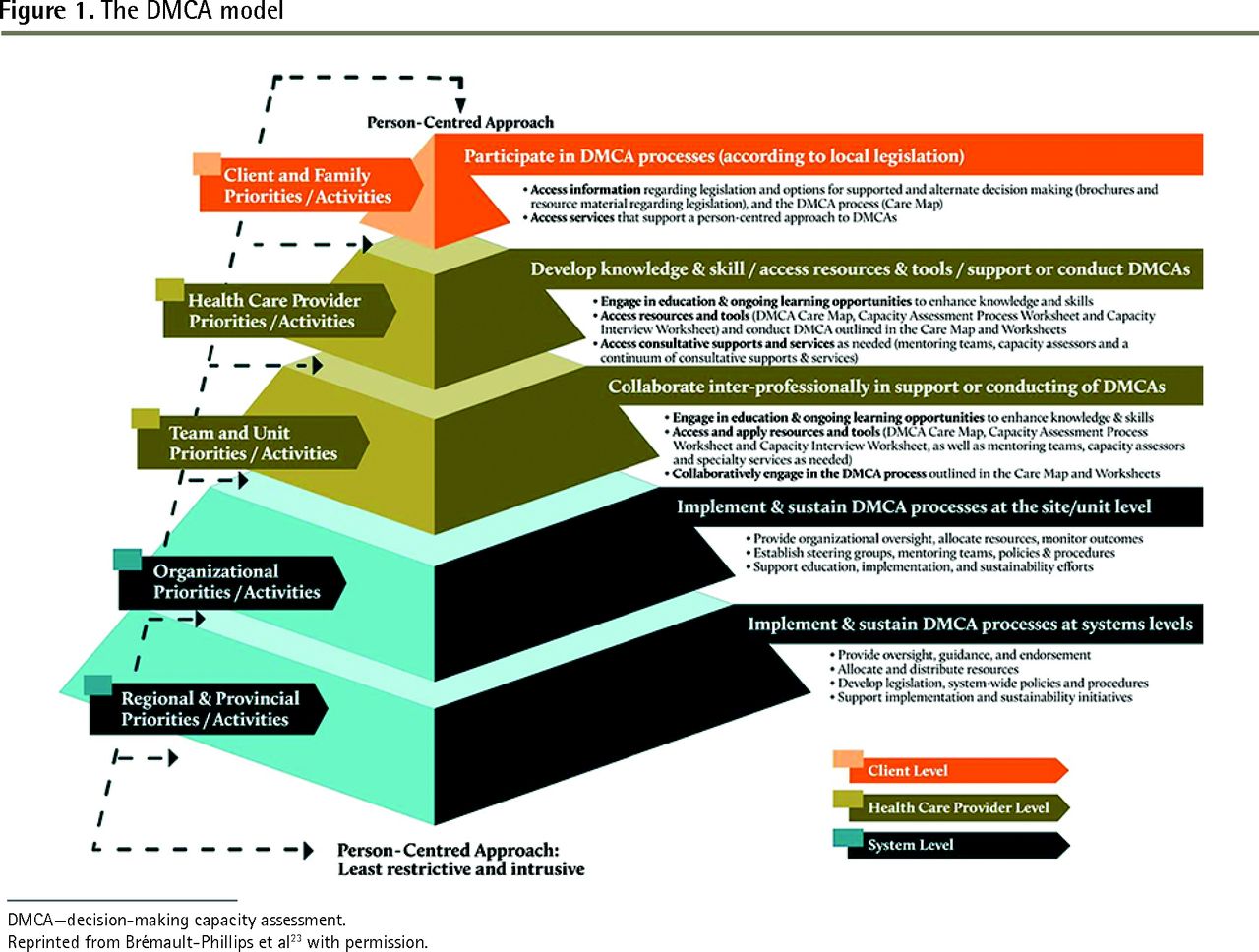
- Figure 1.
The DMCA model
DMCA—decision-making capacity assessment.
Reprinted from Brémault-Phillips et al23 with permission.
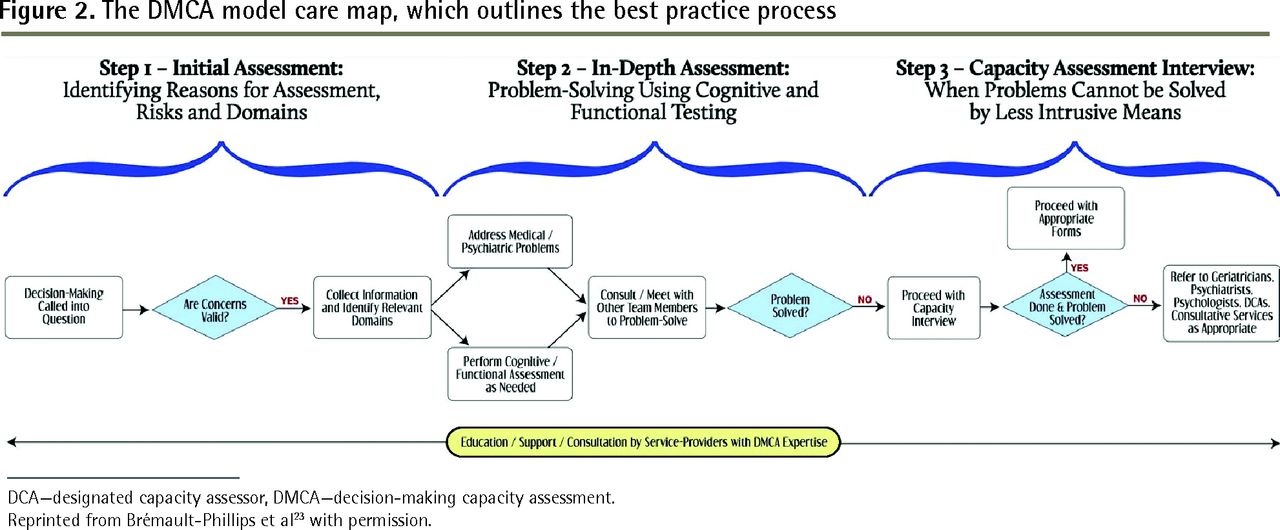
- Figure 2.
The DMCA model care map, which outlines the best practice process
DCA—designated capacity assessor, DMCA—decision-making capacity assessment.
Reprinted from Brémault-Phillips et al23 with permission.
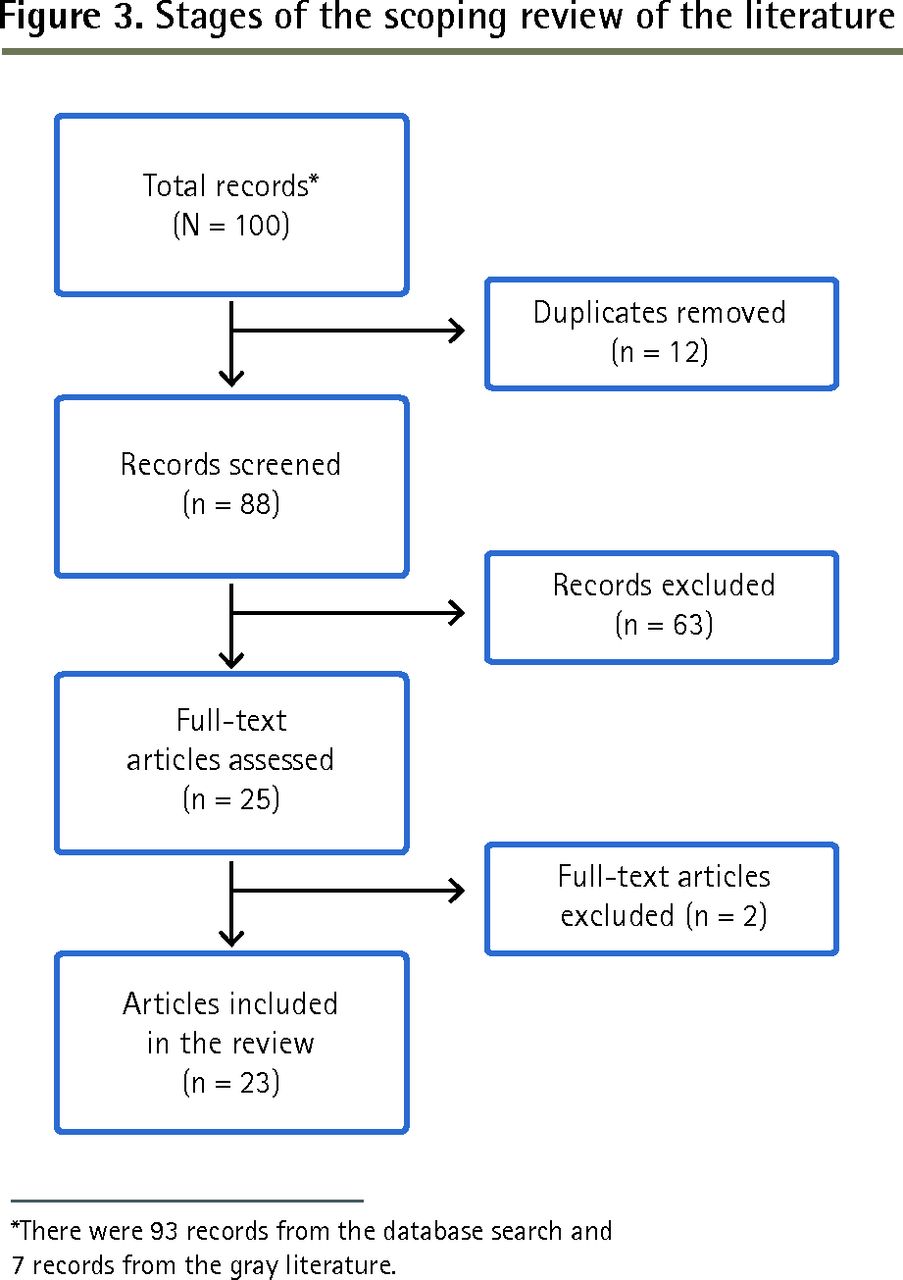
- Figure 3.
Stages of the scoping review of the literature
*There were 93 records from the database search and 7 records from the gray literature.



Tables
FACTORS FINDINGS AND RELATED PARTICIPANT QUOTATIONS THEMES FROM SCOPING LITERATURE REVIEW THAT THIS FACTOR APPLIES TO Facilitators • Physicians’ commitment to delivering PCC As PCC is central to the DMCA model, many participants felt comfortable adopting it “I really like the patients. I like the amount of time I get to spend with patients. I like to get to know them well, and I like complexity and the uncertainty to some extent. I feel like it’s an area that’s overlooked by the rest of medicine. I can make a big difference doing not too much”
“I love geriatrics. I feel like I’m their advocate. Somebody has to be looking out for them”
DMCAs will become more important as the population ages. Providing PCC will involve the administration of DMCAs to those patients for whom DMC is a concern • Team-based approach to conducting comprehensive DMCAs A team-based approach is valuable in conducting comprehensive DMCAs. Physicians are often reliant on IP team members for assessment and problem-solving expertise. In units and sites that were able to establish a collaborative IP approach to DMCAs, physicians believed they were better able to conduct a comprehensive DMCA “I just think anyone who’s involved in their care, I am happy for anyone’s input, everyone’s input who has some type of vested interest in this person’s care. OT, PT, nurse, anyone who’s involved—I think that they’re all so helpful”
Many doctors report that training is suboptimal. Doctors lack sufficient training to complete DMCAs on their own and rely greatly on other IP team members for expertise. There is no consistent approach to DMCA; physicians note that there is no method to conducting DMCAs, but note that working with an IP team is a good approach • Tools associated with the DMCA model to guide the DMCA process The DMCA model tools—in particular the worksheets—are reportedly key facilitators. Physicians appreciated that the worksheets guide the process, prompting them to cover all aspects of the DMCA. They also found that the worksheet facilitates collation of IP team findings and standardizes the problem-solving approach “I find [the worksheets] helpful just because I don’t have that much experience yet … it just reminds me to think of everything”
Many doctors report that training is suboptimal. Doctors lack sufficient training, but note that the worksheets associated with the DMCA model process improves their ability to complete DMCAs Barriers • Knowledge gaps regarding DMCAs More inexperienced FPs did not think they had enough training and exposure to real-life experiences to confidently conduct DMCAs. Some felt less confident making judgments when unfamiliar with a patient, while others were worried about the serious consequences of their assessment (eg, patient’s loss of autonomy) “Not good. I question [DMCAs] all the time, but I try to make sure everyone in the team agrees with what I’m saying”
“Additional training for sure ... I felt like I had no experience”
“It’s not really a huge part of our training”
Many doctors report that training is suboptimal and tension exists between ethical principles of autonomy and protection, particularly when unfamiliar with a patient • Isolation from IP teams Some participants reported that they did not have access to an IP team, felt uncomfortably isolated, and desired greater collaboration “No, I’m on my own. There’s no one”
Many doctors report that training is suboptimal. It is difficult to make clinical judgments concerning DMC when education is lacking and there is limited access to IP teams to assist • Conflicts with families Resolving conflicts with family members residing at a distance and infrequently involved in a patient’s life was difficult, as was balancing patient medical needs while engaging with family members. Physicians noted that conflicts tend to arise over issues such as medical decisions (eg, family attempting to override their medical judgment), finances, DMCAs, facility choice, end-of-life decisions, and legal guardianship), or when family members either appear to have ulterior motives (eg, financial) or are unaware of the patient’s wishes (eg, goals of care and advance directives) “We’ve done the whole process, everyone is on board and all of the sudden we get this call from the daughter from England or the States, ‘Oh, I don’t agree with this ....’ She wants to change everything, challenges meds, challenges the way you’re practising medicine, and you’re like, oh, wow”
“And they’re often a person that has a strong personality, and then they take over the family dynamics. And most people don’t have personal directives; they weren’t dealt with”
Tension exists between ethical principles of autonomy and protection. When family members become involved, issues can arise concerning autonomy and familial wishes, regardless of motive • Concerns about liability, responsibility to the patient, and lack of clarity on billing Physicians are in a difficult position regarding DMCAs, as they often spend only short periods of time with a patient (participants reported conducting a DMCA in 0.5 to 2 hours), during which time they make a determination about a person’s DMC that might have legal implications “It’s just the challenge of being constantly threatened with litigation; threatened that you don’t know what you’re talking about; threatened that they’re going to get more and more people involved”
“For me it’s the legality of it all. Like, what does this mean? If I don’t do a capacity assessment because I don’t think it’s needed, does that mean … I am somehow legally responsible? Like those parts of it all, I’d really like to know more”
Knowledge gaps were evident regarding billing methods for DMCAs and financial remuneration outlined within and permissible according to local legislation“No, I bill, but I probably don’t bill right”
“No, I just do like a daily visit with a modifier”
DMCAs will become more important as the population ages and many doctors report that training is suboptimal. There will be increasing demands on doctors as their patients age, requiring additional or increased training and time to complete these assessments DMC—decision-making capacity, DMCA—decision-making capacity assessment, IP—interprofessional, OT—occupational therapist, PCC—person-centred care, PT—physical therapist.
RECOMMENDATIONS FINDINGS AND PARTICIPANT QUOTATIONS THEME FROM SCOPING LITERATURE REVIEW THAT THIS RECOMMENDATION APPLIES TO Enhanced training and education is needed Physicians emphasized the need for appropriate training to ensure that those conducting DMCAs have requisite knowledge and skills. Participants indicated that more experience working through case studies with physician colleagues would be beneficial “I think there definitely is a need for people who are trained to do this”
“I think a lot of residency training is done by social work or OTs, so when I was training as a resident I never did any of it. It wasn’t a physician’s job”
“I guess as someone who’s just recently come through the program, as far as I can remember, I think I only received 1 session on capacity, maybe 2 sessions ... and for a long time, it was only a half-day session. I don’t think we did a lot of hands-on cases”
Many doctors report that training is suboptimal Access to IP team supports holistic and comprehensive DMCA Participants recommended having greater access to experienced HCPs (eg, social workers, OT, nurses) to facilitate or conduct DMCAs “In an ideal world, any professional who had a deep knowledge of this issue”
“A social worker, though I’d love an OT who does some types of testing and does it all the time. Their job, because I mean, I don’t do them very often, it’s always our RN that does them, so that would be something I’d like, someone that’s experienced to do it”
Many doctors report that training is suboptimal Consultative or mentoring support would enable FPs to enhance their competencies in DMCAs and discuss complex cases with colleagues Participants expressed the need for access to physician colleagues who might be able to offer consultative or mentoring support “Rural clients, I know they have DMCA mentors in the community. One of them was very far southeast with the case that I was involved with, and she did very well. So it was good that they had that person there right in the area and they could do part of the assessment, not all of the assessment. That was really good. It’s great. I think the more knowledge we disseminate the better”
“One of the things that I think was probably key was the role [the provincial mentor] played in the success of this. Because oftentimes there would be cases, and I think [the mentor] built their confidence and skill level within that group …. And that’s very important because if you have just got everybody brand new and just trained in the actual model as a capacity assessor, they don’t know how to think around some of the difficult cases”
Many doctors report that training is suboptimal Appropriate remuneration is needed for services rendered Greater clarity regarding billing practices and remuneration processes was recommended. Participants suggested that this might increase the number of physicians who would engage in DMCAs “The other thing that helps is I’m on an ARP, which is really helpful. Our psychiatrist is on fee-for-service …. There is only a billing code for 1 activity for capacity related. That’s to enact a personal directive. There’s no billing code for EPOA work, guardianship application, capacity-assessment report, mentorship, sitting at a committee meeting, and educating. So ARP under the geriatrics specialized program allows us a certain percentage of time for research, administration, and education. And so with that I’ve decided which areas I want to focus on, and capacity was one of them. That allows me to sit at meetings and do the extra mentorship and support”
DMCAs will become more important as the population ages. To be agreeable with completing DMCAs, physicians need to be appropriately remunerated through established payment and billing procedures ARP—alternate relationship plan, DMCA—decision-making capacity assessment, EPOA—enduring power of attorney, HCP—health care professional, IP—interprofessional, OT—occupational therapist, PT—physical therapist, RN—registered nurse.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.