


Abstract
Objective To identify which factors influence medical students’ decision to choose a career in family medicine and pediatrics, and which factors influence their decision to choose careers in non–front-line specialties.
Design Survey that was created based on a comprehensive literature review to determine which factors are considered important when choosing practice specialty.
Setting Ontario medical school.
Participants An open cohort of medical students in the graduating classes of 2008 to 2011 (inclusive).
Main outcome measures The main factors that influenced participants’ decision to choose a career in primary care or pediatrics, and the main factors that influenced participants’ decision to choose a career in a non–front-line specialty.
Results A total of 323 participants were included in this study. Factors that significantly influenced participants’ career choice in family medicine or pediatrics involved work-life balance (acceptable hours of practice [P = .005], acceptable on-call demands [P = .012], and lifestyle flexibility [P = .006]); a robust physician-patient relationship (ability to promote individual health promotion [P = .014] and the opportunity to form long-term relationships [P < .001], provide comprehensive care [P = .001], and treat patients and their families [P = .006]); and duration of residency program (P = .001). The career-related factors that significantly influenced participants’ decision to choose a non–front-line specialty were as follows: becoming an expert (P < .001), maintaining a focused scope of practice (P < .001), having a procedure-focused practice (P = .001), seeing immediate results from one’s actions (P < .001), potentially earning a high income (P < .001), and having a perceived status among colleagues (P < .001).
Conclusion In this study, 8 factors were found to positively influence medical students’ career choice in family medicine and pediatrics, and 6 factors influenced the decision to choose a career in a non–front-line specialty. Medical students can be encouraged to explore a career in family medicine or pediatrics by addressing misinformation, by encouraging realistic expectations of career outcomes in the various specialties, and by demonstrating the capacity of primary care fields to incorporate specific motivating factors.
Medical student specialty choice affects society as a whole, as the pattern of residency selection shapes the long-term composition of the medical work force. Although residency outcomes are determined by the Canadian Resident Matching Service (CaRMS) match process, historically there has been a relative deficit of students applying to primary care specialties, and family medicine in particular, resulting in unfilled training positions. For example, in 2014 there were 89 unfilled training positions in family medicine at the conclusion of the first iteration of the match.1 This results in a distribution of physicians across specialties that does not necessarily align with the needs of Canadians. While some specialties are overwhelmed with qualified physicians and facing problems of unemployment and underemployment,2–5 others, largely primary care and front-line consultant specialties, are struggling to maintain a high level of care with an inadequate number of providers.6–11 The result is underuse of existing health resources, while dedicating financial and societal resources to problems of scarcity in other specialties. Determining the main factors that lead students to choose non–front-line specialist careers is essential, because it provides insight into whether interest in front-line specialties can be enhanced through increased educational exposure, illumination of existing misinformation, or modification of current practice opportunities.
Numerous factors have previously been demonstrated to have an influence on specialty selection, including sex, initial career interest, and perceptions about controllability of lifestyle, prestige, practice setting, variety, and one’s scope of practice.12–14 However, the relative effect of each of these influential factors and the degree to which they correlate with final residency choice remains unknown. Moreover, data are limited with respect to factors specifically affecting the decision to pursue family medicine or pediatrics at the completion of training. The objective of this study was to identify the specific factors that influence medical students’ specialty choice at the time when they are applying to the residency match, and determine the relative importance of each factor.
METHODS
Ethics approval was obtained from the Western University Health Sciences Research Ethics Board. The study population included a sample of medical students recruited from a single representative academic institution. Students from the graduating classes of 2008 to 2011 (inclusive) were invited to participate. This included 548 students in total. Exclusion criteria included students who were unable to complete the questionnaire in English and students who did not apply to CaRMS.
Survey design began with a comprehensive review of the literature to detect factors previously identified as important in career choice.12–14 Based on this literature, a questionnaire was designed with the goal of comprehensively assessing the various influences on specialty choice. The first section of the questionnaire encompassed demographic characteristics, as well as geographic, financial, and personal characteristics (eg, hobbies and interests). The second section involved a list of all programs offered by CaRMS, from which students were asked to rank their preferred specialties. The third section included a list of 40 potential career- and training-related factors that might influence their career choice. Students were asked to score the relevance of each factor on an ordinal scale. Finally, students were asked to identify the 3 most influential factors in choosing their career specialty. This survey was designed specifically for this study and was not pilot-tested.
Questionnaires were distributed in March of each year from 2008 to 2011 (ie, 4 consecutive years), following the submission of fourth-year medical student residency choice rank lists to CaRMS but before the release of match results. For the purpose of this study, respodents’ data were analyzed with respect to 15 career- and training-related factors that were selected a priori as being of potential relevance to a choice of a career in family medicine or pediatrics. Only respondents indicating their first choice specialty were included.
For the purpose of this investigation, family medicine and pediatrics were selected a priori as most consistent with the traditional concept of front-line primary care consultant providers. While other specialties provide consultative front-line care, the core focus of these specialties is on long-term comprehensive patient care. Family medicine and pediatrics provide the foundation for Canadian patient care and were thus selected as most representative of front-line primary care providers.
Responses were dichotomized into positive influences (including “major positive influence” and “positive influence”) and negative influences (“major negative influence” and “negative influence”). Responses of “no influence” were excluded from this portion of the analysis. Respondents most interested in primary care or consultant front-line specialties were compared with those most interested in specialty careers using 2-sample tests of proportions. Each influential factor was examined to compare the proportion of subjects from each of these 2 cohorts who indicated that the factor was a positive influence on their top specialty choice. An a priori α level was set at .05 (2-tailed). The false discovery rate method as described by Benjamini and Hochberg was used to correct for the multiple comparisons to avoid the likelihood of identifying a false-positive result without underpowering our study.15
RESULTS
In total, 323 fourth-year students were surveyed, yielding a response rate of 59%. Demographic information appears in Table 1. Each of the 15 factors were assessed to determine what proportion of students from each cohort considered the factor to be a positive influence on their career choice. Table 2 illustrates the relative importance of each of these factors to medical students overall. Figure 1 presents the relative importance of each factor to individuals choosing primary care careers in family medicine or pediatrics versus those selecting non–front-line specialties.
Characteristics of participants
Factors that influenced participants’ career choice: The 15 identified factors that influenced career choice are organized by their percentage of influence relative to career choice selection. Presented are combined data for both primary care and non–front-line specialties.
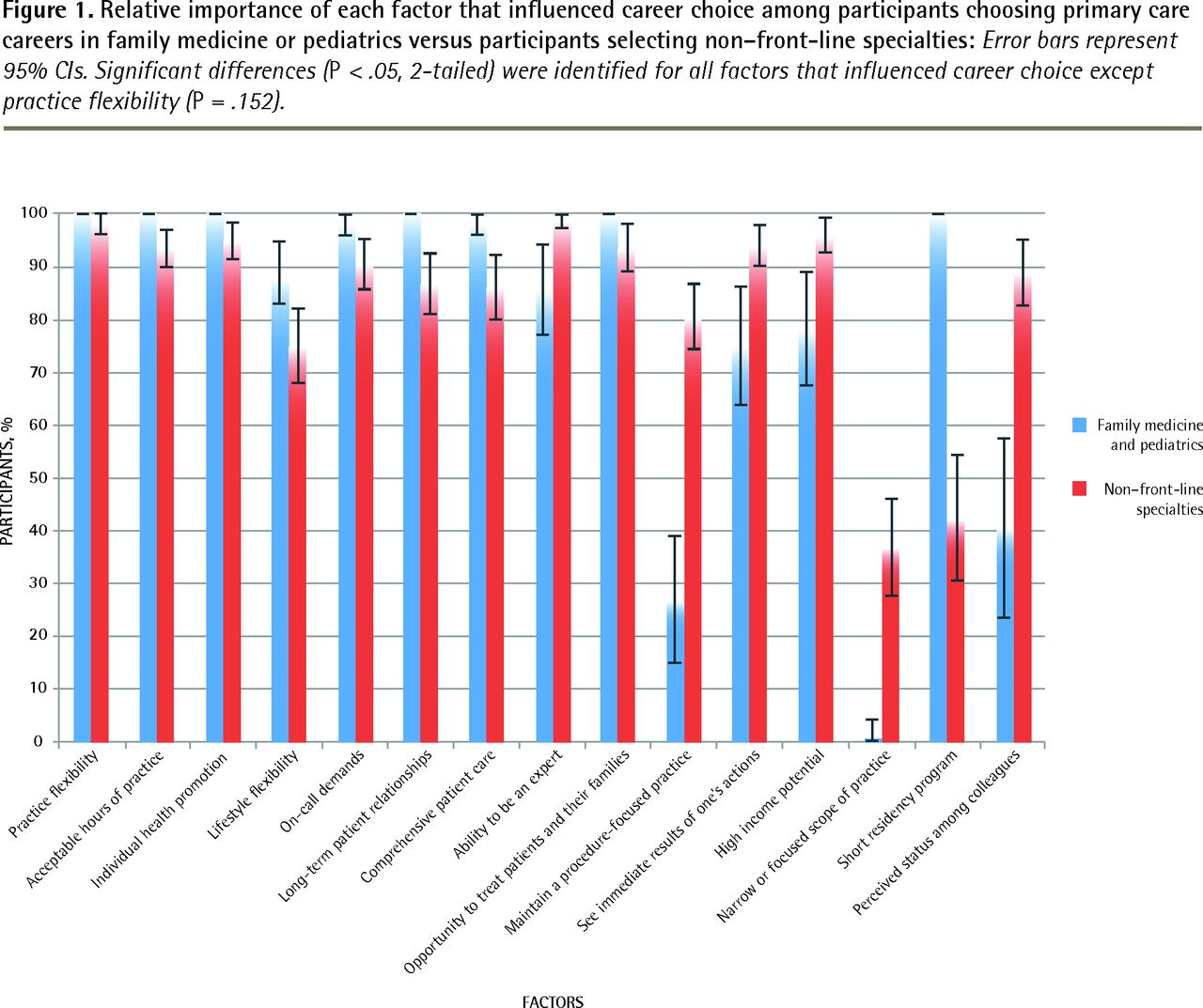
Relative importance of each factor that influenced career choice among participants choosing primary care careers in family medicine or pediatrics versus participants selecting non–front-line specialties: Error bars represent 95% CIs. Significant differences (P < .05, 2-tailed) were identified for all factors that influenced career choice except practice flexibility (P = .152).
Eight out of the 15 career- or training-related factors had a statistically significant positive influence on participants’ career choice of family medicine or pediatrics compared with other specialties. A significantly greater percentage of those who chose family medicine or pediatrics cited acceptable hours of practice (P = .005), ability to promote health on an individual level (“individual health promotion”) (P = .014), lifestyle flexibility (P = .006), acceptable on-call demands (P = .012), opportunities to form long-term relationships with patients (P < .001), providing comprehensive care (P = .001), treating patients and their families (P = .006), and the potential for a short residency program (P = .001) as factors that positively influenced their career choice when compared with those who did not choose careers in front-line specialties.
Six of the career-related factors were statistically significantly more likely to be positive influences on career choice for those who chose non–front-line specialties. These students were significantly more concerned with the ability to become an expert (P < .001), to maintain a focused scope of practice (P < .001), to have a procedure-focused practice (P = .001), to see immediate results from their actions (P < .001), to potentially obtain a high income (P < .001), and to have a perceived status among colleagues (P < .001).
Practice flexibility (eg, patient population treated and choice of procedures) was chosen as a positive influence on career choice by nearly all student participants, and thus it did not have a significant positive influence on career choice for participants in either cohort.
DISCUSSION
The factors that appear to predispose students to choosing family medicine or pediatrics fell into 3 general categories: work-life balance (acceptable hours of practice, lifestyle flexibility, and acceptable on-call demands); physician-patient relationships (promoting individual health, developing long-term relationships with patients, providing comprehensive care, and treating patients and their families); and the duration of the residency program.
Conversely, participants who pursued a non–front-line specialty career prioritized the following: developing a specific expertise, maintaining a procedure-focused practice, seeing immediate results of their actions, potentially earning a high income, and having a perceived status among their colleagues. In order to encourage these individuals to explore front-line and primary care specialties, we must examine how these specific motivating factors might be fulfilled in a primary care or front-line context. It is difficult to imagine that an individual who prioritizes developing a high level of expertise within a narrow focus will be drawn to the broader experience of a primary care or front-line consultant specialty. Similarly, while some areas of primary care offer an opportunity to perform procedures, an individual who is heavily motivated by procedural work might remain more likely to pursue a procedure-oriented specialty.
Perceived status among colleagues is important to medical students. In this survey, this factor was considered important by more than 40% of fourth-year medical students. However, students do not view status as equal among specialties; 89% (95% CI 82.7% to 95.1%) of those interested in non–front-line specialties believed it was a positive influence on their choice of specialty, whereas only 41% (95% CI 23.6% to 57.6%) of those interested in primary care believed it to be a positive influence on their choice of specialty.
Previous literature has noted the presence of a medical hierarchy, with specialists being perceived as having a higher status.16,17 A 2008 article in Canadian Family Physician described increasing isolation of family physicians from their specialist colleagues, and observations by primary practitioners that specialists no longer understand the role of primary care. They note denigration of family medicine by medical schools and specialists, and the creation of a concept of family medicine as a “default” specialty.17 While it might be difficult to change cultural norms within the medical milieu, this might be essential to increasing interest in primary care careers. Blissett et al studied factors affecting final-year Canadian medical students’ specialty choice and discovered that mentorship played an important role.18 The medical students who participated in our survey were taught primarily by specialists with relatively few exposures to primary care instructors. An increase in the presence of mentors from family medicine and pediatrics might not only encourage interest in primary care, but might also lead to a shift away from the perceived hierarchy of medical specialties.
A second possible area for intervention lies in the issue of remuneration. In our study population, high income potential was an influential factor for 57% of students and was a significantly more positive influence among those who chose non–primary care specialties (94%, 95% CI 90.0% to 98.0%) than among those who chose primary care specialties (78%, 95% CI 67.3% to 89.1%). While various funding models and a wide spectrum of different practice models creates variability in the compensation of primary care practitioners and pediatricians, a perception exists among medical students that family physicians are underpaid.19 Over the past several years, alternative funding plans have improved remuneration for family physicians in Ontario.20 According to the 2011 annual report of the Office of the Auditor General of Ontario, as early as 2007 to 2008, family physicians who were paid through family health group or family health organization alternate funding arrangements earned 25% more than family physicians paid under the traditional fee-for-service model did.20 Even before this increase in remuneration variability, medical students were shown to underestimate the pay of family physicians while overestimating the pay of some specialists, such as dermatologists.19 In general, compensation for both family physicians and pediatricians varies enormously owing to the level of flexibility inherent in these practices (eg, office-based vs hospital-based practices, participation in emergency department or obstetric work, academic practice, and practice location). However, previous studies on medical student perceptions suggest a lack of appreciation for this variability. Students overwhelmingly refer to the traditional outpatient clinical practice, identifying general practitioners as “gatekeepers” and emphasizing communication and counseling functions.21 This limited conception of the field is important, as the career-related factor found to be influential to the greatest proportion of students (91%) was practice flexibility. While believing that practice flexibility is important, medical students fail to appreciate the breadth and flexibility of practice that follows a choice to pursue primary care or any front-line specialties. Increased exposure to these specialties might encourage an appreciation for the variability of practice models, as well as the resultant variability in remuneration. Efforts to increase medical student exposure to family physicians, with an emphasis on exposing them to a variety of practice models, is likely to improve their perception of family medicine as a career option and decrease the widespread misperceptions that currently influence career decisions. Furthermore, open discussion of the economic and financial realities of medicine (eg, practice overhead, net income, opportunity, cost of longer residency training, retirement planning) will assist in breaking down financial misconceptions and their influence on career choice.
Limitations
In presenting the data herein, several limitations must be addressed. The data presented stemmed from a single academic institution. Therefore, its findings are likely affected by the specific institutional culture and medical school curriculum. However, given the nature of medical school training, including required content that is shared among Canadian institutions, and cultural similarities across Canadian institutions, we expect that these findings can be extrapolated to other Canadian universities. This study was also limited by the lack of a pre-existing validated survey tool. The novel survey tool used herein was designed specifically for this study and was not pilot-tested before its use to negate any repeated-measurement bias. Nevertheless, the described influences were derived from the literature, and the results obtained appear to support the survey’s construct and content validity. Recognizing this limitation, the results obtained must be interpreted within the context of this study. Finally, the grouping of pediatrics and family medicine as front-line primary care specialties is most in keeping with the traditional concepts of these specialties and might not be completely representative of regional variations in the practice of these specialties across Canada. As mentioned, the results obtained are limited to the a priori assumptions of this investigation and should be restricted to this context. In spite of these limitations, the data do provide meaningful insights into the factors that contribute to career choice selection among medical students.
Conclusion
This investigation provides a novel perspective by focusing on Canadian medical students while they were making their decisions regarding residency choice. This point of action assessment provides insight into the main factors that influence the career decisions that ultimately shape the composition of the Canadian physician work force. The data presented provide direction for medical specialty career counseling with a focus on highlighting the values and remedying the misconceptions about particular specialties.
Notes
EDITOR’S KEY POINTS
Medical students’ decisions regarding specialty contribute to the formation of the national physician work force. It is important to determine the main factors that lead students to choose non–front-line specialist careers in order to have insight into whether interest in front-line specialties can be enhanced through increased educational exposure, illumination of existing misinformation, or modification of current practice opportunities.
The authors surveyed medical students at the time that they were applying to the residency match to determine what factors influenced their choice of specialty.
Status was considered important by more than 40% of respondents. However, students did not view status as equal among specialties; 89% of those interested in non–front-line specialties believed it was a positive influence on their choice of specialty, whereas only 41% of those interested in primary care believed it to be a positive influence on their choice of specialty.
POINTS DE REPÈRE DU RÉDACTEUR
Le choix d’une spécialité par les étudiants en médecine influence la composition du contingent national de médecins. Il est important d’identifier les facteurs qui amènent les étudiants à choisir une spécialité autre que la première ligne de manière à savoir s’il est possible de mousser l’intérêt à l’égard des spécialités de première ligne par l’entremise d’une exposition accrue durant la formation, en corrigeant les renseignements erronés qui circulent ou en modifiant les possibilités de pratique.
Afin d’établir les facteurs qui influencent le choix d’une spécialité, les auteurs ont mené une enquête auprès d’étudiants en médecine au moment où ils s’inscrivaient au jumelage des résidents.
Plus de 40 % des répondants considéraient que le statut social associé à une spécialité était important. Ils estimaient toutefois que les spécialités ne donnaient pas toutes le même statut; 89 % de ceux qui s’intéressaient aux spécialités plus pointues croyaient que cela avait une influence positive sur leur choix de spécialité, un avis qui était partagé par seulement 41 % de ceux qui envisageaient une spécialité de première ligne.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
Dr Osborn administered the survey to students, analyzed the results, and wrote the manuscript. Dr Glicksman administered the survey to students, assisted in the statistical analysis, and provided critical assessment of the manuscript. Dr Brandt conceived the idea for the study, designed the research methodology and the survey, assisted in the administration of the survey and the interpretation of the results, and assisted in writing the manuscript. Dr Doyle assisted with the conception of the study, the development of the study methodology, and the development of the survey; and provided critical analysis of the manuscript. Dr Fung assisted with the study design, the development of the survey, and the interpretation and analysis of the results; and provided critical assessment of the manuscript. All authors gave final approval of the version submitted for publication.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}