


Article Figures & Data
Figures
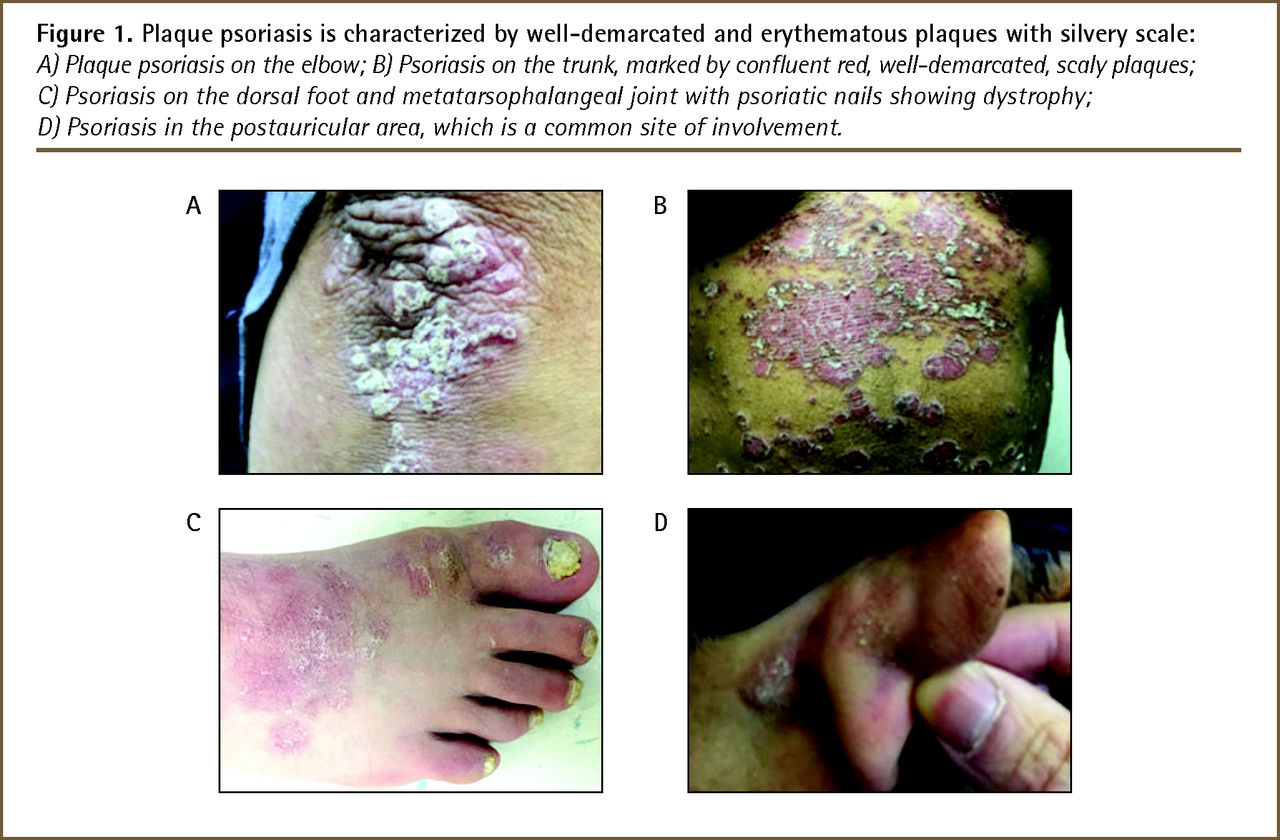
- Figure 1.
Plaque psoriasis is characterized by well-demarcated and erythematous plaques with silvery scale:
A) Plaque psoriasis on the elbow; B) Psoriasis on the trunk, marked by confluent red, well-demarcated, scaly plaques; C) Psoriasis on the dorsal foot and metatarsophalangeal joint with psoriatic nails showing dystrophy; D) Psoriasis in the postauricular area, which is a common site of involvement.
- Figure 2.
Patients with psoriasis might have nail involvement, which can present without concomitant plaques:
A) Psoriatic nails, consisting of pitting, distal onycholysis, subungual hyperkeratosis, and crumbling; B) Leukonychia and splinter hemorrhages; C) Distal onycholysis and oil drop sign.
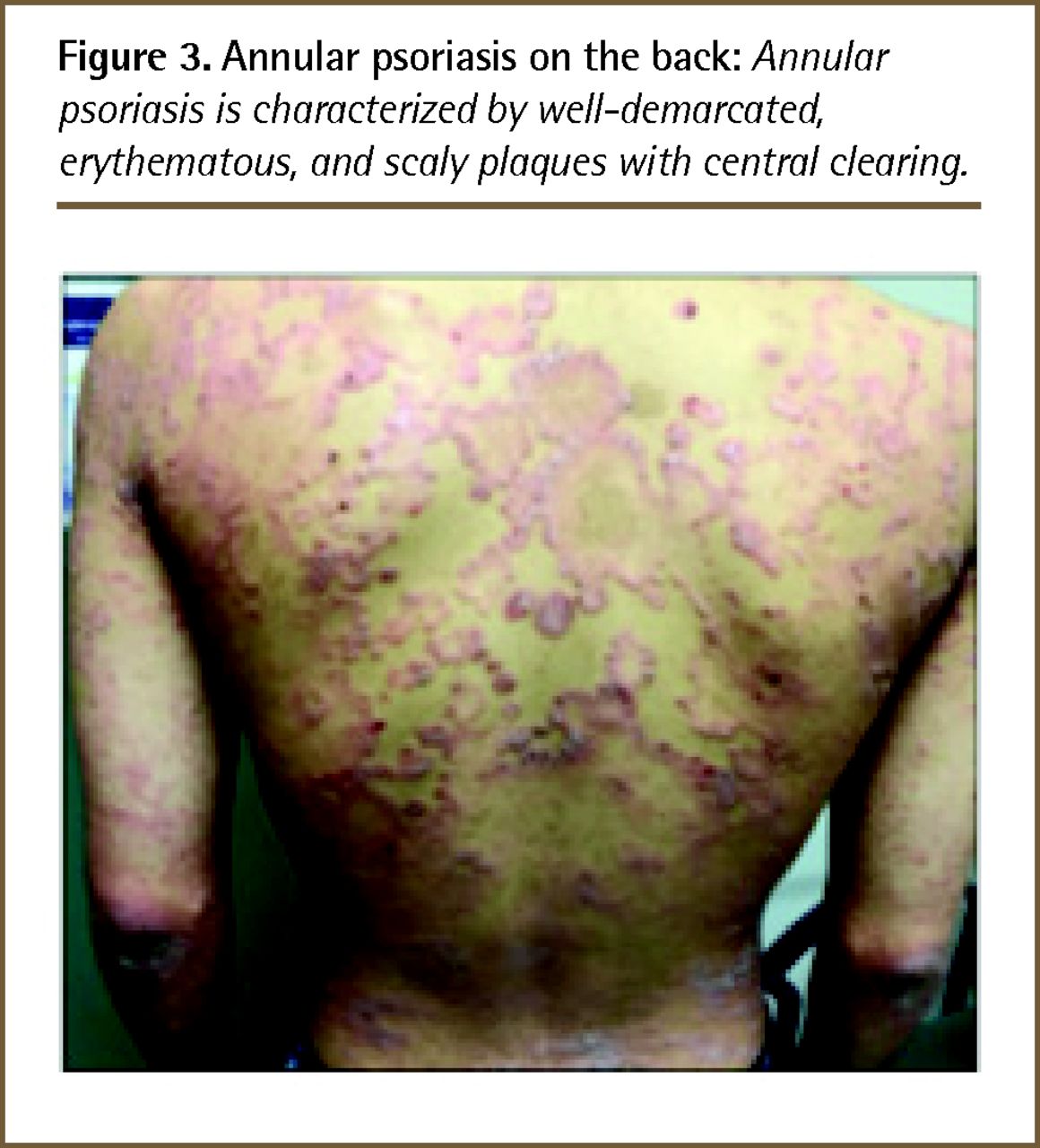
- Figure 3.
Annular psoriasis on the back: Annular psoriasis is characterized by well-demarcated, erythematous, and scaly plaques with central clearing.
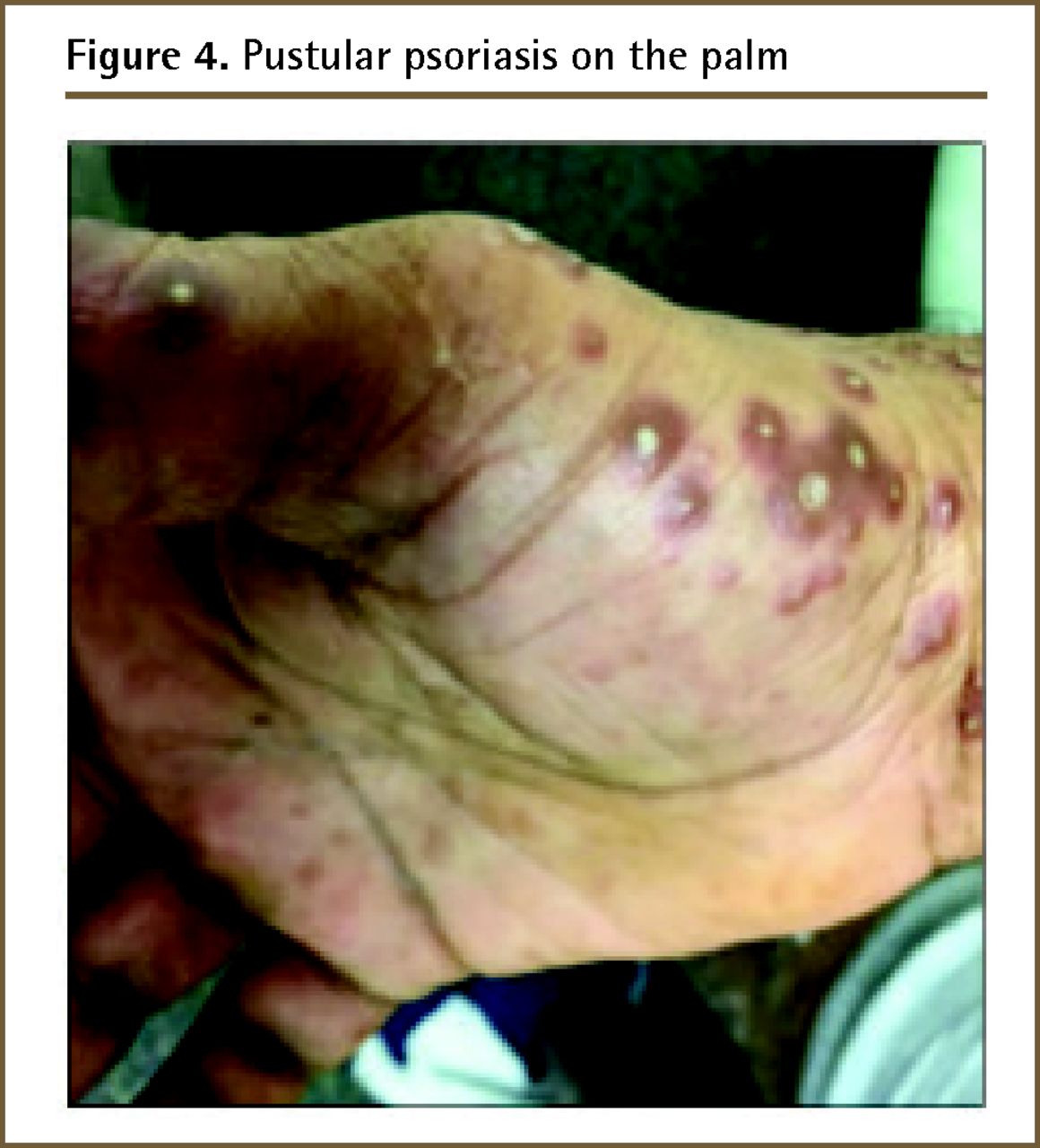
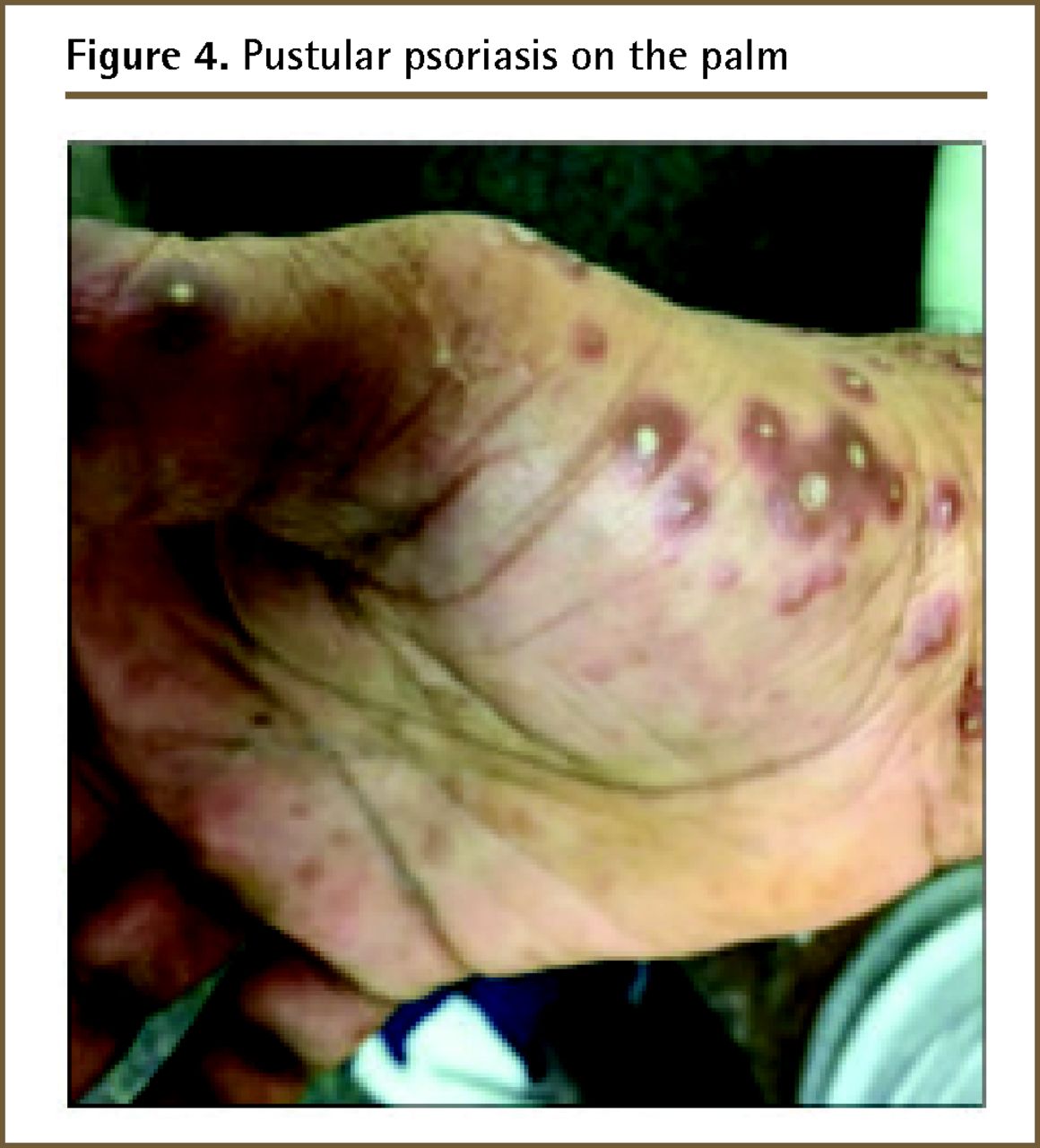
- Figure 4.
Pustular psoriasis on the palm
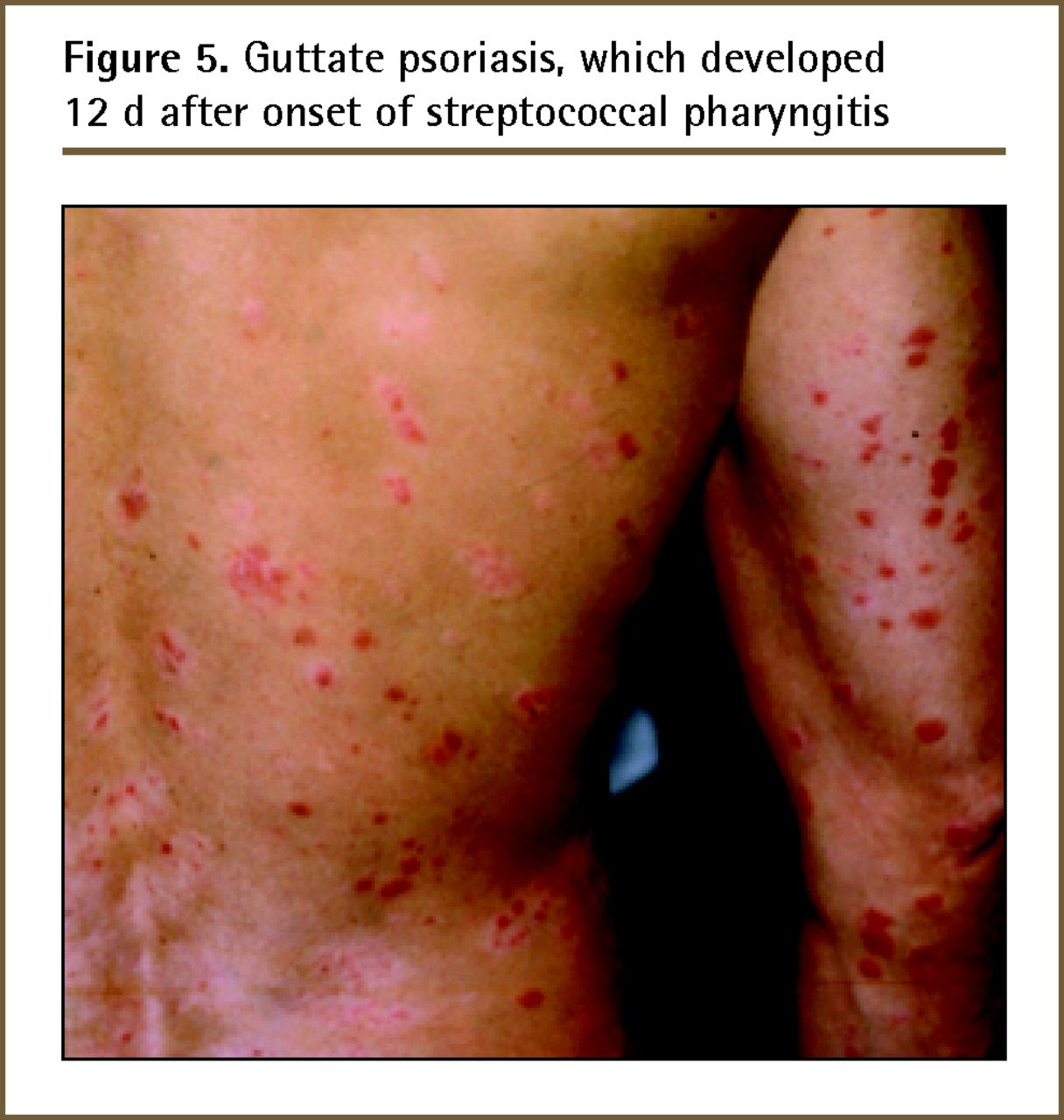
- Figure 5.
Guttate psoriasis, which developed 12 d after onset of streptococcal pharyngitis
- Figure 6.
Approaching erythrodermic psoriasis
- Figure 7.
Treatment algorithm for healthy adult men with chronic plaque psoriasis (> 5% BSA) without psoriatic arthritis
BB—broadband, BSA—body surface area, NB—narrowband, PUVA—psoralen plus UVA, UV—ultraviolet.





Tables
CLINICAL MANIFESTATION CLINICAL FINDINGS Plaque psoriasis Well circumscribed, erythematous, scaly plaques > 0.5 cm in diameter, either as single lesions or as generalized disease
Classified further according to anatomic sites
• Flexural Also known as intertriginous or inverse psoriasis
Well circumscribed, minimally scaly, thin plaques localized to the skin folds (inframammary, axillary, groin, genital, natal cleft regions)
• Nail Can present without concomitant skin plaques
Pitting, distal onycholysis, subungual hyperkeratosis, oil drop sign, splinter hemorrhages, leukonychia, crumbling, red lunula
Nail involvement is a predictor of psoriatic arthritis
• Scalp One of the most common sites of psoriasis
Often difficult to treat
• Palmoplantar Localized to the hands and soles of feet
Confluent redness and scaling without obvious plaques to poorly defined scaly or fissured areas to large plaques covering the palm or sole
Other variants • Guttate Acute eruption of “dew-drop,” salmon-pink, fine-scaled, small papules on the trunk or limbs
Can follow history of group A streptococcal pharyngitis or perianal group A streptococcus dermatitis
• Pustular Sheets of monomorphic pustules on painful, inflamed skin
Most commonly localized to the palms or soles
• Erythroderma Acute or subacute onset of generalized erythema covering 90% or more of the patient’s entire body with little scaling
Might be associated with hypothermia, hypoalbuminemia, electrolyte imbalances, and high-output cardiac failure
Life-threatening emergency
• Annular Well demarcated erythematous scaly plaques with central clearing
Data from the Canadian Psoriasis Guidelines Committee.1
SEVERITY MEASURES* Mild < 3% BSA†
Disease with a minimal effect on the patient’s QoL; patient can achieve an acceptable level of symptomatic control by routine skin care measures and topical therapy
Moderate 3% to 10% BSA†
Disease that cannot be, or would not be expected to be, controlled to an acceptable degree by routine skin care measures or disease that substantially affects the patient’s QoL, either because of the extent of the disease, physical discomfort (pain or pruritus), or location (eg, the face, hands, feet, or genitals)
Severe > 10% BSA†
Disease that cannot be, or would not be expected to be, satisfactorily controlled by topical therapy and that causes severe degradation of the patient’s QoL
BSA—body surface area, QoL—quality of life.
↵* These are definitions for clinical practice, as applied in the Canadian guideline. The Psoriasis Area and Severity Index is another measure of disease severity, based on BSA, erythema, induration, and scaling.
↵† The size of a single hand is estimated to be 1% BSA.
Data from the Canadian Psoriasis Guidelines Committee.1
DIFFERENTIAL DIAGNOSES DISTINGUISHING CLINICAL FEATURES Atopic dermatitis • Predominant symptom of pruritus and typical morphology and distribution (flexural lichenification in adults and older children; facial and extensor papules and vesicles in infancy) Contact dermatitis • Patches or plaques with angular corners, geometric outlines, and sharp margins dependent on the nature of the exposure to the irritant or allergen Lichen planus • Violaceous lesions and frequent mucosal involvement Secondary syphilis • Copper-coloured lesions and frequent involvement of palms and soles Mycosis fungoides • Irregularly shaped lesions with asymmetric distribution, peculiar colour, and wrinkling due to epidermal atrophy Tinea corporis • Fewer lesions with annular configuration Pityriasis rosea • Tannish-pink, oval papules and patches with “Christmas tree” configuration on trunk with sparing of the face and distal extremities
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Efficacy and Safety of Cannabis Transdermal Patch for Alleviating Psoriasis Symptoms: Protocol for a Randomized Controlled Trial (CanPatch)
- RNA sequencing of a large number of psoriatic patients identifies 131 novel miRNAs and 11 miRNAs associated with disease severity
- Glycoconjugation as a Promising Treatment Strategy for Psoriasis
- Nascent transcript analysis of glucocorticoid crosstalk with TNF defines primary and cooperative inflammatory repression
- Nascent transcript analysis of glucocorticoid crosstalk with TNF defines primary and cooperative inflammatory repression