


The Canadian population is aging. In 2014, women aged 50 to 54 years comprised the largest age cohort of women in Canada,1 an age at which most women begin the menopause transition. This might be accompanied by vasomotor symptoms (VMS), genitourinary syndrome of menopause (GSM), mood and sleep changes, joint pain, and more.2
After the early termination of the Women’s Health Initiative in 2002, menopausal hormone therapy (MHT) became highly controversial because of reported increases in the risk of breast cancer and cardiovascular disease.3 In response, interest in nonhormonal options grew and many have been evaluated (eg, antidepressants, gabapentin, pregabalin, clonidine, phytoestrogens). While they were effective for mild VMS, these medications are not particularly effective for moderate to severe VMS or for some of the other menopause-related concerns.4,5
New guidelines
Menopausal hormone therapy remains the most effective treatment of VMS, and is also indicated for GSM (previously called vulvovaginal atrophy) and bone protection.4,6,7 Recently, the Women’s Health Initiative data have been reevaluated to better guide physicians in patient selection, with risks being reevaluated and stratified by age and time since menopause.8 New guidelines have been created, with the consensus that MHT is safest for those younger than 60 years and within 10 years of menopause4,6 and might be continued for some women after age 65.9 This is clinically relevant, as new evidence is emerging indicating that many women continue to experience substantial symptoms well into their 60s, with a mean duration of VMS of more than 7 years and extending beyond 11 years for many.10 With no fixed duration of treatment, the guidelines now state that MHT should be individualized to account for each patient’s unique risk-benefit profile.4,6
Many primary care clinicians have had little experience treating menopausal patients. New guidelines and position statements, including those from the Society of Obstetricians and Gynaecologists of Canada,4 the North American Menopause Society,7 and the International Menopause Society,6 help support health care providers in caring for menopausal women. These statements by leading organizations in mature women’s health include recommendations that certain questions be asked of all perimenopausal women.4,6,7 However, existing menopausal questionnaires, such as the Menopause-Specific Quality of Life Questionnaire and Greene Climacteric Scale, are lengthy and might not be ideal for use in the primary care setting.
With the needs of busy primary care physicians in mind, I have developed a quick menopausal screening questionnaire called the Menopause Quick 6 (MQ6) (Figure 1).4,6 This 6-question scale assesses menopausal symptoms for which there are evidence-based treatment options while providing a patient-centred assessment to guide treatment choices. This short questionnaire, written in lay language, can be used during any clinical encounter, including a periodic health examination.

The Menopause Quick 6 questionnaire: If a patient answers yes to any of questions 1 to 4, she might be a candidate for treatment, and further exploration and assessment is warranted. The Society of Obstetricians and Gynaecologists of Canada and International Menopause Society guidelines recommend that questions 2 to 6 be asked of all perimenopausal women.4,6
These 6 questions were selected because they elicit helpful information that can guide management decisions, as described in Table 1.2,4,6,10–12
How to use the information elicited by questions that comprise the Menopause Quick 6
Putting the MQ6 into practice
The MQ6 was designed to be a quick and efficient tool for primary care practice. The information elicited from the 6 questions can guide evidence-based treatment decisions, as set out in the algorithm in Figure 2.5
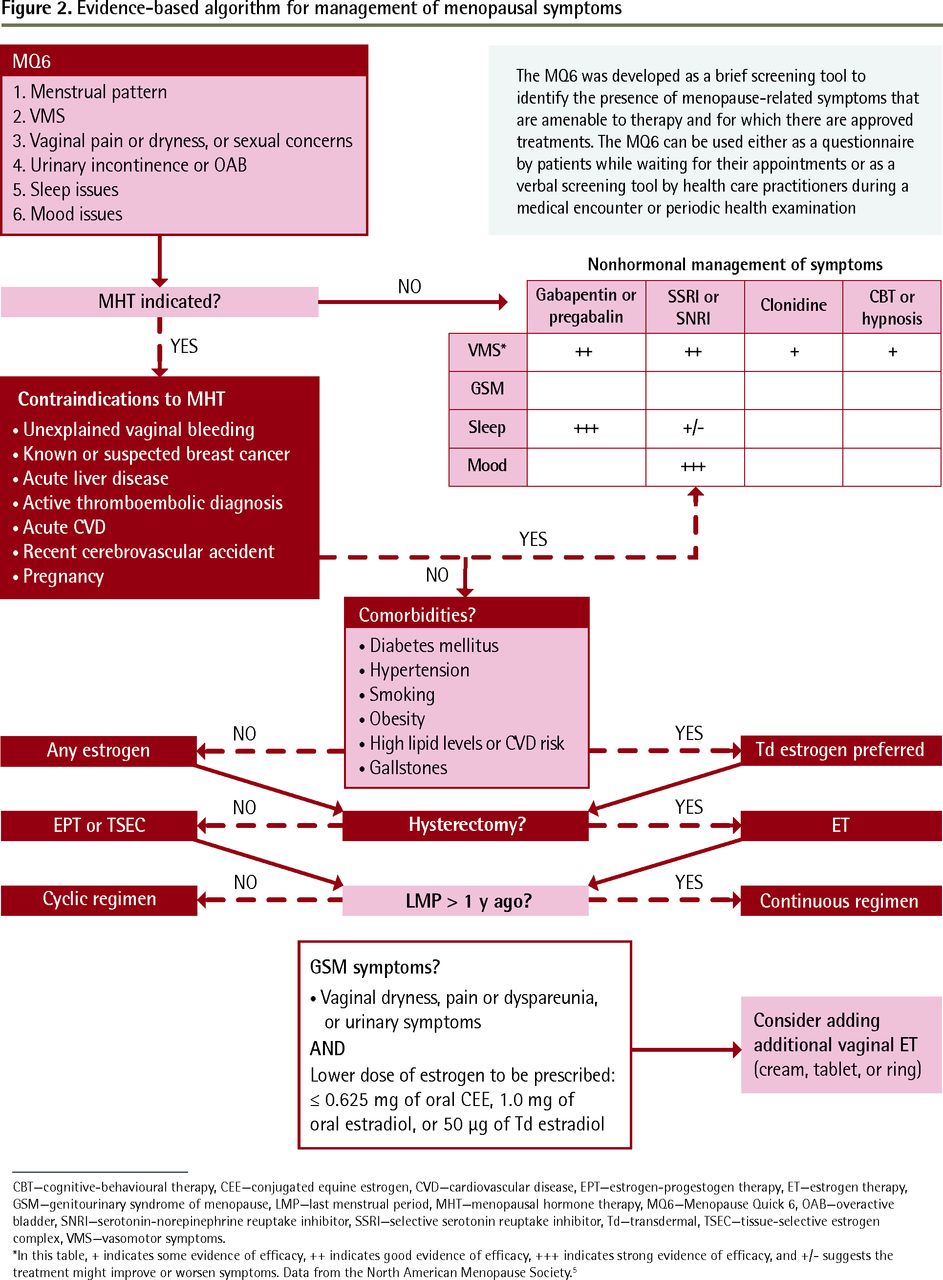
Evidence-based algorithm for management of menopausal symptoms
CBT—cognitive-behavioural therapy, CEE—conjugated equine estrogen, CVD—cardiovascular disease, EPT—estrogen-progestogen therapy, ET—estrogen therapy, GSM—genitourinary syndrome of menopause, LMP—last menstrual period, MHT—menopausal hormone therapy, MQ6—Menopause Quick 6, OAB—overactive bladder, SNRI—serotonin-norepinephrine reuptake inhibitor, SSRI—selective serotonin reuptake inhibitor, Td—transdermal, TSEC—tissue-selective estrogen complex, VMS—vasomotor symptoms.
*In this table, + indicates some evidence of efficacy, ++ indicates good evidence of efficacy, +++ indicates strong evidence of efficacy, and +/− suggests the treatment might improve or worsen symptoms. Data from the North American Menopause Society.5
As the algorithm specifies, when hormone therapy is indicated and there are no contraindications to MHT, then a transdermal preparation, which avoids first-pass hepatic metabolism, is recommended for women with comorbidities that increase cardiovascular risk, including risk of venous thromboembolism or stroke (based on observational data).11
As the progestogen in the MHT regimen provides endometrial protection, patients who have undergone a hysterectomy require only estrogen therapy. When endometrial protection is required, the use of either estrogen-progestogen therapy or a tissue-selective estrogen complex is recommended.4 A tissue-selective estrogen complex recently approved for use in Canada combines conjugated equine estrogen with a selective estrogen receptor modulator (bazedoxifene), the latter component providing endometrial protection while eliminating the need for a progestogen.
In the first year after menopause begins, women will often bleed when taking a continuous MHT regimen, so a cyclic regimen is preferred.11 Cyclic regimens usually include a steady dose of an estrogen for days 1 to 25 or 1 to 31 of the month, accompanied by a progestogen for 12 to 14 days of the month, resulting in withdrawal bleeding. Continuous regimens use steady daily doses of an estrogen and progestogen.13
Of note, we are now treating with lower-dose regimens of MHT, which do not always provide sufficient treatment of the local symptoms of GSM. For adequate treatment of local symptoms, the addition of vaginal estrogen therapy should be considered.
Conclusion
Primary care clinicians are increasingly using measurement-based care and integrating it into their electronic medical record systems. The MQ6 can help fill a gap for measurement-based care in mature women’s health. It takes about 2 minutes to use the MQ6 questionnaire with a perimenopausal patient, making it an efficient tool for busy primary care clinicians.
Using the MQ6 ensures that clinicians are asking the right questions in a standardized way. The accompanying algorithm, guided by the answers to the MQ6, is based on the latest evidence-based guidelines and can facilitate clinical decisions in an area that has a controversial and sometimes confusing history. From the patient perspective, using these tools can help patients engage to discuss sensitive issues and it reassures them they are being cared for in a holistic manner.
Acknowledgments
I thank Dr Wendy Wolfman, Mr Mike Hill, and Ms Christina Clark for their contributions to this article.
Footnotes
This article is eligible for Mainpro+ certified Self-Learning credits. To earn credits, go to www.cfp.ca and click on the Mainpro+ link.
This article has been peer reviewed.
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro d’avril 2017 à la page e219.
Competing interests
Dr Goldstein has received honoraria for advisory board participation and consultant fees from Pfizer and Merck.
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.