


Article Figures & Data
Figures
- Figure 1.
The Menopause Quick 6 questionnaire: If a patient answers yes to any of questions 1 to 4, she might be a candidate for treatment, and further exploration and assessment is warranted. The Society of Obstetricians and Gynaecologists of Canada and International Menopause Society guidelines recommend that questions 2 to 6 be asked of all perimenopausal women.4,6
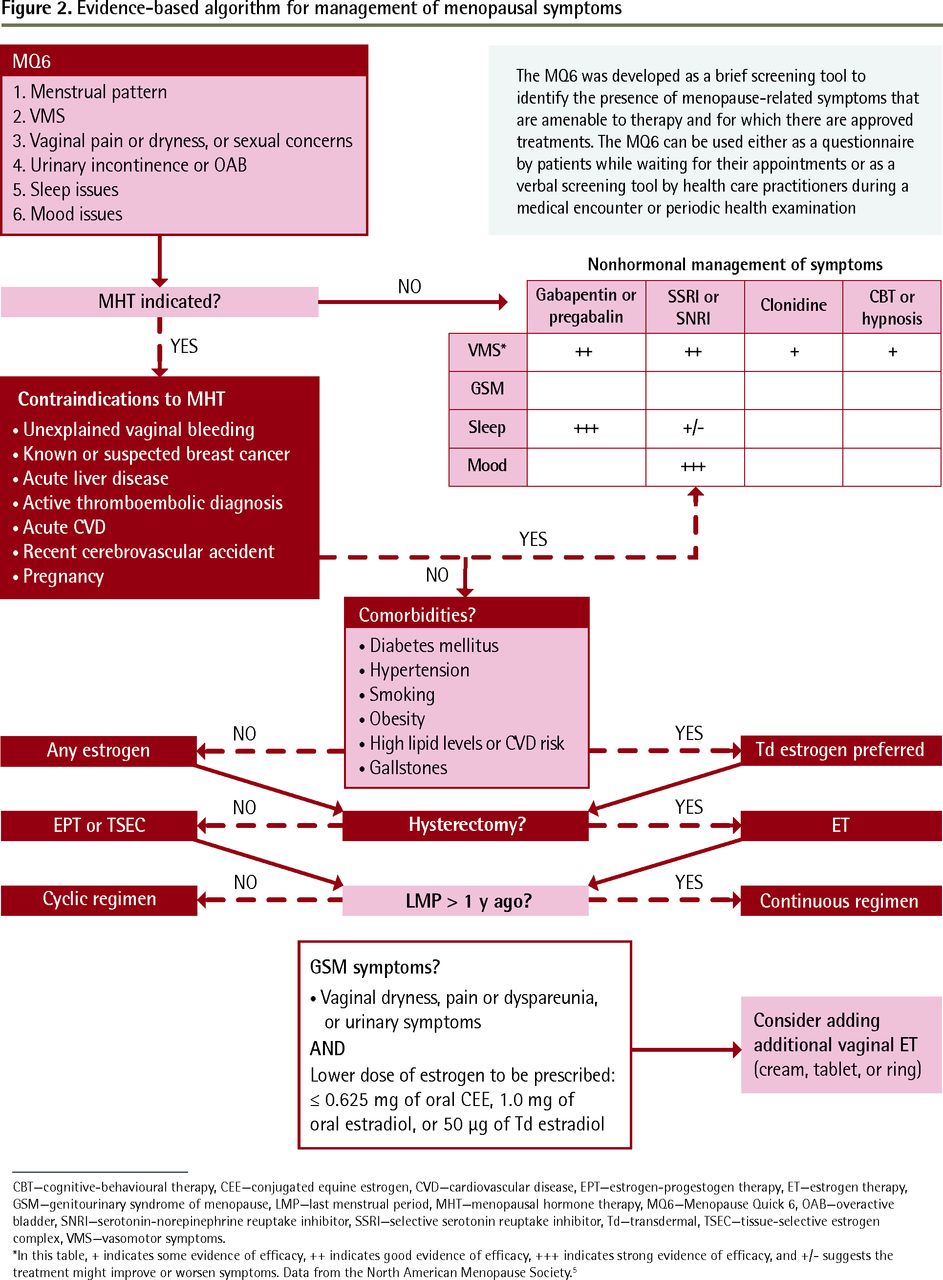
- Figure 2.
Evidence-based algorithm for management of menopausal symptoms
CBT—cognitive-behavioural therapy, CEE—conjugated equine estrogen, CVD—cardiovascular disease, EPT—estrogen-progestogen therapy, ET—estrogen therapy, GSM—genitourinary syndrome of menopause, LMP—last menstrual period, MHT—menopausal hormone therapy, MQ6—Menopause Quick 6, OAB—overactive bladder, SNRI—serotonin-norepinephrine reuptake inhibitor, SSRI—selective serotonin reuptake inhibitor, Td—transdermal, TSEC—tissue-selective estrogen complex, VMS—vasomotor symptoms.
*In this table, + indicates some evidence of efficacy, ++ indicates good evidence of efficacy, +++ indicates strong evidence of efficacy, and +/− suggests the treatment might improve or worsen symptoms. Data from the North American Menopause Society.5

Tables
- Table 1.
How to use the information elicited by questions that comprise the Menopause Quick 6
QUESTION INTERPRETATION Q1: Any changes in your periods? Menstrual irregularities signal imminent menopause. A recent study found that when VMS start before the cessation of menses, they can be expected to last longer (median 11.8 y) than VMS that start after the LMP (3.4 y).10 Further, when prescribing MHT for women who are still cycling irregularly or within 1 y of their LMP, a cyclic hormone regimen should be used.11 If the LMP was more than 1 y ago, continuous regimens can be offered. For all women with cessation of menses younger than 45 y, MHT is recommended Q2: Are you having any hot flashes? Up to 80% of menopausal women experience VMS. When these are mild, many lifestyle and nonhormonal interventions can be effective. Moderate to severe VMS are treated most effectively by hormone therapy4,6 Q3: Any vaginal dryness or pain, or any sexual concerns?
Q4: Any bladder issues or incontinence?The term vulvovaginal atrophy has been replaced by genitourinary syndrome of menopause, reflecting the changes to the vulva, vagina, and urinary tract and to sexual functioning owing to the menopausal drop in estrogen. Many women are reluctant to talk about their vaginal or sexual concerns, bladder issues, or incontinence, yet these can have a substantial negative effect on quality of life. We have effective treatments for these symptoms, so we must ask Q5: How is your sleep? Sleep disturbances are common during menopause and are most often attributed to hot flashes.2 Poor sleep can exacerbate mood and anxiety issues and contribute to cognitive complaints and even weight gain Q6: How is your mood? Menopause is a high-risk time for first-episode or recurrent depression.12 In addition, anxiety and irritability peak during perimenopause. Both SSRIs and SNRIs have been shown to be effective for these mood disorders while having a beneficial effect on VMS. Women who remain symptomatic despite these medications might benefit from hormonal augmentation LMP—last menstrual period, MHT—menopausal hormone therapy, SNRI—serotonin-norepinephrine reuptake inhibitor, SSRI—selective serotonin reuptake inhibitor, VMS—vasomotor symptoms.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.