


Abstract
Objective To describe recent trends and patterns in methadone maintenance treatment (MMT) practice regionally and over time in the province of Ontario.
Design Population-based descriptive study using health administrative data between September 1, 2011, and December 31, 2014.
Setting Ontario.
Participants All active MMT-prescribing physicians and patients receiving MMT in the study period.
Main outcome measures Characteristics of MMT-prescribing physicians, including age, sex, specialty type, practice region, and practice volume; characteristics of patients receiving MMT, including age, sex, neighbourhood income, and region of residence.
Results Between September 1, 2011, and December 31, 2014, the number of MMT-prescribing physicians and patients who received MMT increased by 26% and 42%, respectively. In 2014, there was a total of 312 MMT-prescribing physicians and 49 703 patients receiving MMT. In 2014 and on a per capita basis, patients receiving MMT were more prevalent in rural regions; and within rural regions, there were disproportionately large numbers of young female MMT patients residing in low-income neighbourhoods.
Conclusion The number of physicians prescribing MMT and patients receiving MMT has increased substantially between 2011 and 2014, with the largest per capita distribution occurring in rural regions and involving young adults. While availability of and access to MMT has improved considerably from before 2000 to levels of high use, these developments are likely influenced by recent trends in the proliferation of prescription opioid misuse across general populations.
Opioid use and dependence have been serious problems in Canada for almost a century. Until recently, the population who used opiates consisted of those in marginalized populations who injected heroin intravenously, resulting in considerable morbidity and mortality.1,2 For example, epidemics of HIV transmission and drug-related overdose deaths observed in Canada (eg, British Columbia) before 2000 involved mainly heroin use.3–6 More recently, opioid use has shifted to include the nonmedical use of prescription opioid medications. Prescription opioid abuse has been documented to be common both in general (eg, adult, adolescent, student) and in marginalized (eg, street, First Nations, correctional) populations in Canada.7–9 Opioid-related harms have been rising in Canada recently. Acute opioid-related overdose deaths in Ontario have risen from 1991 to 2010, and most of these deaths are related to prescription opioids.10,11 Similar trends have been observed in other provinces.12
Methadone maintenance treatment (MMT) was pioneered in Canada and the United States in the 1960s.4,13 It is effective in improving key health, drug use, and social outcomes, and is considered the criterion standard for opioid dependence treatment.14–16 In Canada, restrictive federal regulations imposed on MMT provision (eg, special licensing requirements for physicians, provider and patient monitoring) severely curtailed its availability from the 1970s until the early 1990s. Concretely, there were only 60 MMT-prescribing physicians and 1595 patients receiving MMT in Ontario in 1996.17 In the mid-1990s, regulatory control shifted from federal to provincial authorities.17,18 Revised MMT regulations specifically in Ontario included more flexible MMT practice guidelines, as well as an emphasis on community-based MMT provision (eg, involving GPs and community pharmacies).19,20 These changes led to rapid and extensive increases in MMT availability and use. Consequently, by 2001, there were 161 MMT-prescribing physicians and 7787 patients receiving MMT in Ontario17,21; an assessment published in 2011 found that in 2010 these numbers had risen to 309 and 29 743, respectively.22 Other provinces (eg, British Columbia) observed similar expansions of MMT services.23
While the MMT policy reforms resulted in substantial expansions of MMT availability and uptake, a variety of concerns have emerged regarding the state of MMT organization and practice since its implementation. For example, MMT availability has been concentrated primarily in urban centres, while many non-urban or rural regions have remained underserviced. Many patients receiving MMT have not been able to consistently adhere to MMT, engaging in a “revolving door” pattern of brief engagement and disengagement.24,25 More recently, there have been concerns about MMT quality and practices—including the potentially inappropriate use of and billing for ancillary services—especially related to the rising number of “for profit” MMT clinics across Ontario. In addition, a rise in methadone-related fatalities in Ontario triggered a coroner’s inquest, with multiple recommendations for improved MMT control and practice.26–29 Thus, while MMT has an abundant evidence base to justify its use, there is a concern of adverse consequences related to the more recent rapid and widespread increase in MMT use.
Now, 20 years after MMT regulation reform, we will use unique population-based, administrative data to examine key indicators of MMT provision in Ontario. Specifically, we will examine MMT use in Ontario, as well as physician and patient characteristics, as a MMT-policy case study over time within the context of marked shifts in the nature of opioid abuse.
METHODS
Our examination focuses on the number and characteristics of MMT-prescribing physicians and patients receiving MMT from September 1, 2011, to August 31, 2014, in Ontario—Canada’s most populous province (approximately 11 500 000 residents older than 15 years of age in 2012). Our data are drawn from key administrative databases housed at the Institute for Clinical Evaluative Sciences (ICES), where—in the context of a single-payer and public insurance (ie, Ontario Health Insurance Plan [OHIP]) based health care system in Ontario—unique information on patients and providers of medical services are captured by way of encrypted and linked data systems. In September 2011, the Ontario Ministry of Health and Long-Term Care introduced new physician billing codes as a financial incentive for services related to MMT care (specifically for supervision of a patient receiving medication, including medication adjustments and discussions with the patient and family members about methadone treatment and consequences) under OHIP. These MMT billing codes allowed identification of all unique patients (15 years of age and older) receiving MMT and physicians providing MMT services in Ontario during the study period. The billing codes capture care provided by Ontario physicians with an active general exemption for MMT to treat opioid dependence, and thus are an opportunity to capture all MMT physicians and patients in Ontario. The billing codes represent payment for monthly management of patients receiving MMT for opioid dependence, and all require at least 1 direct visit in the month for which the overall MMT care is billed. We examined patterns of MMT services, including the number of unique patients receiving MMT and MMT-related patient visits per physician. Additional ICES-based databases (ie, the ICES Physician Database and the Registered Persons Database) were used to examine further characteristics of physicians providing, as well as patients receiving, MMT. Characteristics for both the physicians and the patients included sex, age, and location of practice or residence;for patients only, characteristics included region of residence (ie, urban or rural based on the Rurality Index of Ontario30) and area-level income quintile based on Statistics Canada 2006 census information; and for physicians, their medical specialty was included. Patients receiving MMT were excluded from analyses if they had an invalid OHIP number (unable to link records across databases), were not eligible for OHIP coverage during the study period, or were missing age or sex variables. Both patient and physician data were examined primarily by calendar year and by Local Health Integration Network (LHIN)—the administrative subunits in the regional health authority structure responsible for health care delivery in Ontario; there are 14 LHINs in Ontario. Data were computed including counts, means with standard deviations, medians with interquartile ranges (IQRs), and percentages. We used weighted (for regional population) regression to test for trends (both over time and by region) in utilization rates of MMT services for both patients and providers. We also compared proportions of patients receiving MMT in rural versus urban areas, and the proportion of female patients and those in the 15-to-24 age group in the North West LHIN versus the rest of the province. The study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre in Toronto, Ont.
RESULTS
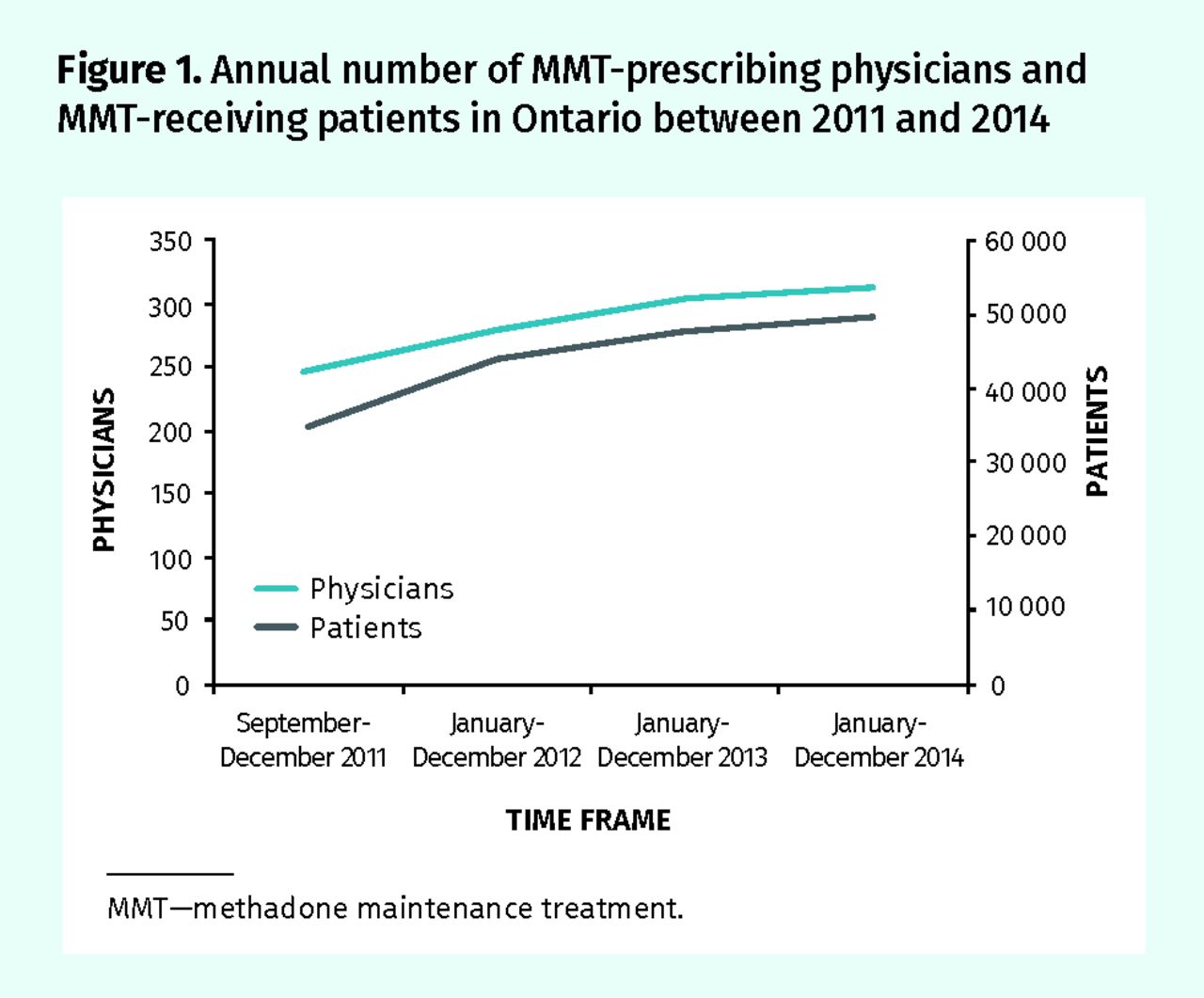
The annual number of unique patients receiving MMT in Ontario increased from 34 938 in 2011 to 49 703 in 2014 (an increase of 42%; linear test for trend, P < .001); correspondingly, the annual number of physicians prescribing MMT increased from 247 in 2011 to 312 in 2014 (an increase of 26%; linear test for trend, P = .03) (Figure 1).

Annual number of MMT-prescribing physicians and MMT-receiving patients in Ontario between 2011 and 2014
MMT—methadone maintenance treatment.
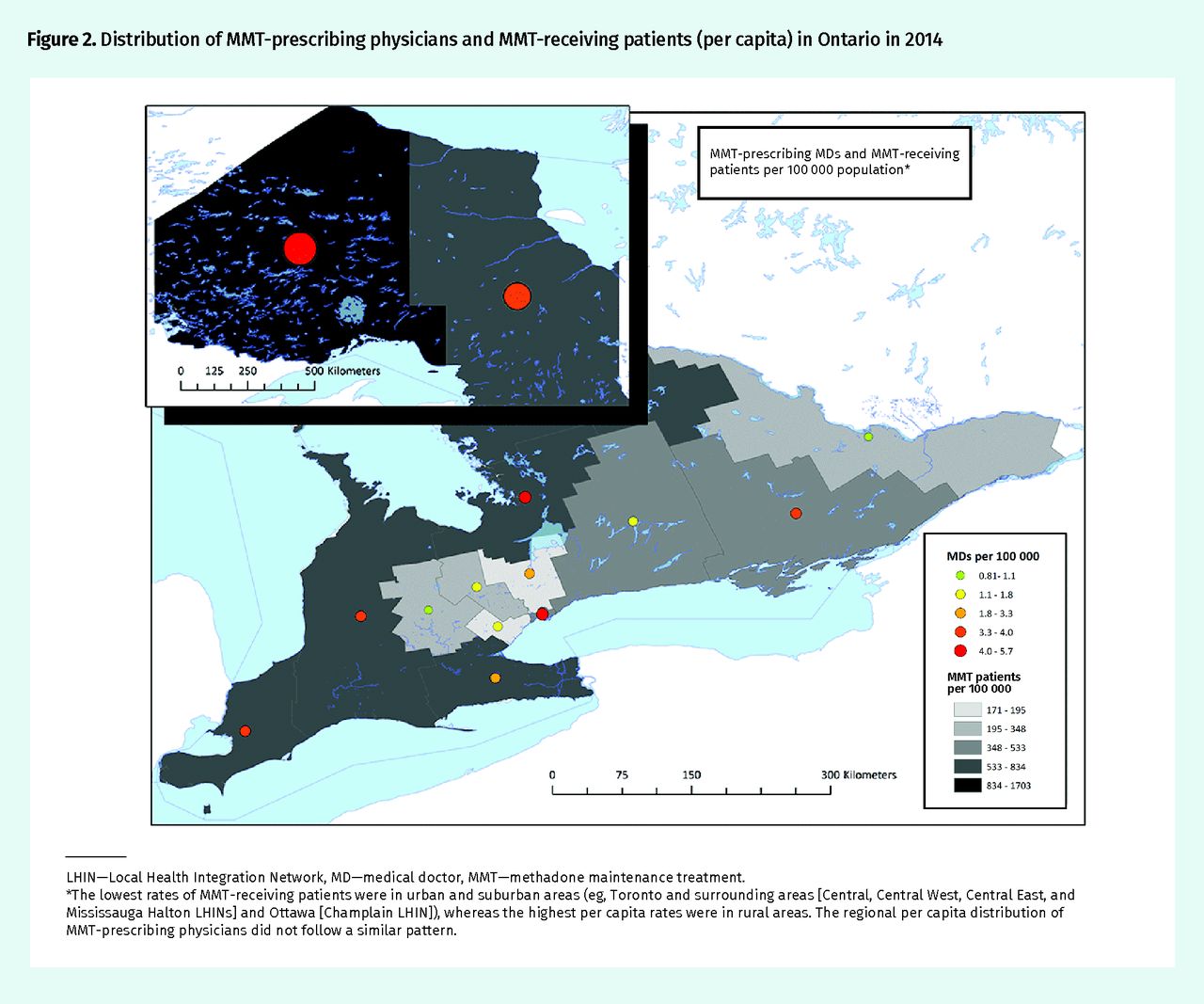
When examining MMT indicators for 2014, the number of MMT-prescribing physicians in LHINs ranged from 6 to 60 (Table 1), and the number of patients receiving MMT in LHINs ranged from 1708 to 7526 (Table 2); based on crude population sizes, the corresponding rates of patients receiving MMT per 100 000 population by LHIN varied 10-fold, from a low of 171 to a high of 1703 (linear test for trend, P < .001); the rates of MMT-prescribing physicians varied 6-fold, from a low of 0.8 to a high of 5.6 (linear test for trend, P < .05). The lowest rates of patients receiving MMT were in urban and suburban areas (eg, Toronto Central and surrounding areas [Central, Central West, Central East, and Mississauga Halton LHINs] and Ottawa [Champlain LHIN]), whereas the highest per capita rates were in rural areas (t test comparing mean of urban-suburban areas vs rural areas, P = .017). The regional per capita distribution of MMT-prescribing physicians did not follow a similar urban-rural pattern (Figure 2).
Number and sociodemographic and practice characteristics of MMT-prescribing physicians in Ontario in 2014, by LHIN
Number and sociodemographic and socioeconomic characteristics of patients receiving MMT in Ontario in 2014, by LHIN
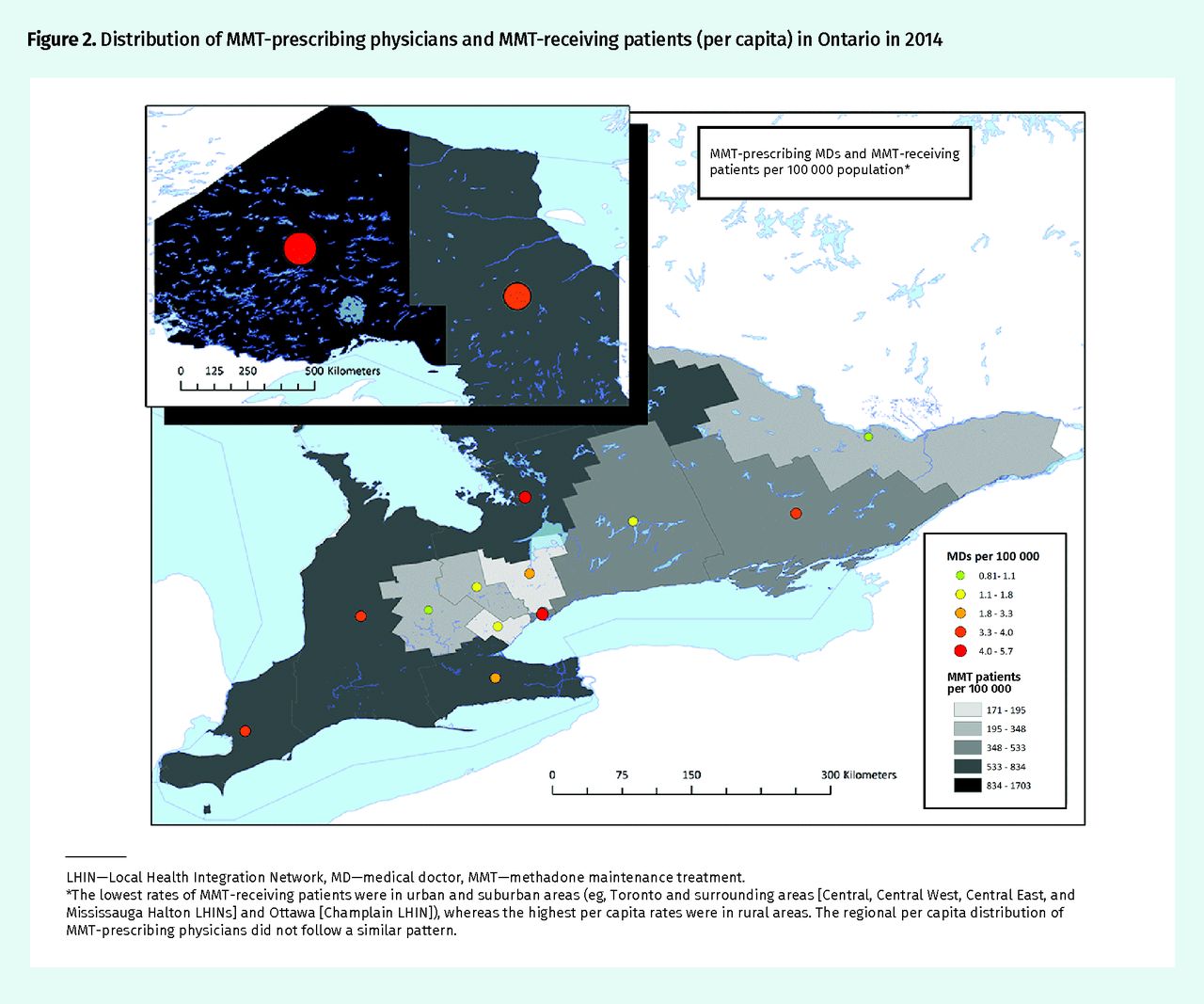
Distribution of MMT-prescribing physicians and MMT-receiving patients (per capita) in Ontario in 2014
LHIN—Local Health Integration Network, MD—medical doctor, MMT—methadone maintenance treatment.
*The lowest rates of MMT-receiving patients were in urban and suburban areas (eg, Toronto and surrounding areas [Central, Central West, Central East, and Mississauga Halton LHINs] and Ottawa [Champlain LHIN]), whereas the highest per capita rates were in rural areas. The regional per capita distribution of MMT-prescribing physicians did not follow a similar pattern.
Most MMT-prescribing physicians were male (74%), younger than 55 years of age (67%), and had a primary care or family medicine designation (75%) (Table 1). Median (IQR) number of monthly unique patients seen by individual MMT-prescribing physicians ranged from a low of 134 (75 to 299) patients for the Waterloo Wellington LHIN to a high of 438 (178 to 564) for the Central West LHIN. Median (IQR) number of monthly MMT-receiving patients varied from a low of 31 (17 to 90) in the North West LHIN to a high of 154 (36 to 228) in the Central East LHIN. Median (IQR) number of monthly MMT-related visits varied by region (lowest in the North West LHIN at 36 [19 to 94] visits vs the highest in the North East LHIN at 191 [70 to 278] visits).
In 2014, most patients receiving MMT were male (63% [range 46% to 78%]) and in the 25-to-44 age group (61% [range 49% to 70%]) (Table 2). Twelve percent (range 5% to 19%) of the total of MMT-receiving patients were younger than 25 years of age. The largest proportion of overall MMT-receiving patients (36% [range 16% to 46%]) resided in the lowest-income neighbourhoods; on a regional level, patients in the regions of and surrounding Toronto (Central [22%], Central West [18%], and Mississauga Halton [16%]) were exceptions to this pattern (Figure 2). Higher rates for both young and low-income-quintile MMT-receiving patients were predominantly found in rural LHINs. Patients receiving MMT in the North West LHIN were statistically significantly different from the rest of the MMT-receiving population; specifically, more than half (54%) of the MMT-receiving patients there were female (percentage of females in the North West LHIN compared with the rest of Ontario, P < .001) and almost 1 in 5 (19%) patients were in the youngest age category (15 to 24 years of age) (percentage in the 15-to-24 age category in the North West LHIN vs the rest of Ontario, P < .001).
DISCUSSION
The present study relied on unique administrative health care data to examine recent population-level characteristics and trends in MMT-prescribing physicians and patients who receive MMT in the province of Ontario.
By 2014, the overall number of MMT-prescribing physicians in Ontario had increased approximately 6-fold since 1996 and doubled since 2001; correspondingly, the number of MMT patients has grown approximately 30-fold since 1996 and 6-fold since 2001. These indicators clearly document a massive expansion of MMT availability and usage, and hence can be interpreted as success indicators in regards to the objective of MMT policy liberalizations and reforms in the late 1990s to improve access to MMT.17,21 In addition, most MMT-prescribing physicians are community-based physicians or GPs, suggesting that MMT provision and care has effectively been moved from specialized, institutional clinics and integrated into more community-based health services; this, likely, has contributed positively to MMT access in the province.19 We also found extensive differences in terms of both MMT provider (6-fold) and patient (10-fold) rates between LHINs, including extremes; currently, almost 1 in 50 residents (2%) in the North West LHIN are patients who receive MMT. These data indicate substantial intra-province differences in MMT service uptake, which might be a function of either differences in MMT need and demand or regional system issues, the specifics of which remain to be investigated and understood. Notably, while MMT utilization and availability was previously concentrated primarily in urban areas, and there were extensive unmet treatment needs in rural regions, MMT utilization rates are now higher in predominantly rural than in urban regions in Ontario.17,22,31
It is important to ask what has been driving the extensive increase in patients who receive MMT. While current epidemiologic estimates of heroin abuse for Ontario are not available, heroin utilization rates have been reported to be decreasing, and the identified MMT-receiving patient population is likely to exceed the total number of heroin users in Ontario.2,32 Rather, while accurate population-based data on current indication for MMT are missing, most of the recent MMT initiations are likely to be for prescription opioid dependence in the context of substantial increases in prescription opioid availability, misuse, and dependence in both general and marginalized or at-risk populations over the past decade.7,8,33 Extensive increases in prescription opioid–related treatment have been recorded in non-MMT treatment (eg, detoxification, non-maintenance treatment) settings during that period.34,35
The presumed widespread use of MMT for prescription opioid dependence raises important questions regarding the evidence for and appropriateness of current treatment practice. While the effectiveness of MMT for heroin abuse is widely documented, several studies have shown that problematic prescription opioid users differ from heroin users presenting for treatment in important characteristics (eg, shorter or less-severe drug use, better physical or mental health, better social integration)36–38; relatively few—and no Canadian—studies have examined MMT outcomes for prescription opioid dependence.39–41 Similarly, there is a dearth of studies focusing on alternative treatments (eg, detoxification, tapering, psychotherapeutic approaches), and available data suggest potential benefits for at least subsets of patients.37,39,41,42 Yet, financial incentives for MMT from the Ministry of Health and Long-Term Care (single public payer of health care in Ontario) during the study period positioned MMT as the preferred treatment over alternative treatments in Ontario.43–45 These circumstances have resulted in a treatment environment where MMT, which in most instances means long-term opioid maintenance treatment, has become the predominant first-line treatment absent of a continuum of treatment options that can be aligned with the severity of opioid dependence presentation (eg, duration of dependence and quantity of regular opioid use). This might both constitute problematic clinical practice and lead to undesirable economic effects and other outcomes; based on a current annual cost estimate of $5651 for MMT, the current annual expenditures for MMT in Ontario would be more than $280 000 000.46
The above concerns appear to be reflected in our study results. For example, between 1-in-5 and 1-in-6 MMT patients in the 2 northern LHINs (ie, North East and North West) were between the ages of 15 and 24, and included disproportionately high rates of females. In addition, there was a pronounced socioeconomic stratification of MMT use across the province by individuals from lowest-income neighbourhoods. It is both questionable whether these large proportions of female teenagers and adults are best served by, potentially close to lifelong, MMT at this stage of their lives.47–49 It is furthermore unclear whether the pronounced concentration of MMT in low-income patient groups truly reflects corresponding socioeconomic patterns of opioid abuse and treatment needs in these particular groups or whether other factors are pushing these individuals into MMT.
Limitations
The study has several limitations. Our data are relevant to Ontario and might not be generalizable to other provinces across Canada. We were only able to examine the MMT activity captured through OHIP billing. Health care provided to status First Nations or Indigenous people—involving most living on reserves—are covered by federal health care coverage. Because these health services under federal program auspices are not captured in ICES data holdings, we are likely underestimating MMT use in regions (eg, rural) with higher rates of First Nations or Indigenous people. Furthermore, LHINs are a large geographic unit to use, and within LHINs there will be rural, urban, and socioeconomic variability. We used LHINs because they are a convenient and established way to define health regions in Ontario. We were unable to use sub-LHIN regionalization because, even with LHIN regionalization, we were unable to report on some MMT physician characteristics because of small sample size. Additionally, our data do not include cases of buprenorphine-naloxone–based maintenance treatment, which is available in Ontario, yet was only covered by provincial health funding during the study period where MMT was documented to not be feasible or effective. Our data also only described MMT provision and use patterns, and did not provide information on treatment outcomes in the population. Finally, the billing codes used to capture characteristics of physicians who prescribe and patients who receive MMT were only initiated in September 2011. For this reason, our data only described trends over 3 years.
Conclusion
In this study we documented extensive and largely community-based expansions of MMT care provision and use of MMT services in Ontario 20 years after important policy reforms. While MMT use varies across Ontario health regions, we question whether the nature of current MMT practice, as well as key patient characteristics, equivocally indicate optimal and evidence-based MMT care provision in the Ontario population, especially in reference to the large numbers of (young) patients mainly with prescription opioid dependence, as well as the increasing proliferation of “for-profit” MMT clinics indicating questionable treatment practice and quality. Facilitated by recent policy and system reforms, the pendulum of MMT expansion might have swung too far in Ontario, resulting in substantive adverse or undesirable effects in the structure, practice, and outcomes of MMT care. These circumstances urgently require more detailed examination, and potential—and, where possible, best evidence–based—policy and regulation adjustments.
Acknowledgments
Dr Kurdyak received operational grant funding from the Ministry of Health and Long-Term Care (MOHLTC) Health Services Research Fund Capacity Award. The Institute for Clinical Evaluative Sciences is funded by the Ontario MOHLTC. The study results and conclusions are those of the authors, and should not be attributed to any of the funding agencies or sponsoring agencies. No endorsement by the Institute for Clinical Evaluative Sciences or the Ontario MOHLTC is intended or should be inferred. This work was supported in part by research funding from the Canadian Institutes of Health Research (CIHR), specifically grant #SMN-139150 (Ontario CRISM [Canadian Research Initiative in Substance Misuse] Node Team grant, NPI [nominated principal investigator]: B. Fischer).
Notes
Editor’s key points
▸ This study examined the trends in methadone maintenance treatment (MMT) in the province of Ontario. By 2014, the overall numbers of MMT-prescribing physicians in Ontario had increased approximately 6-fold since 1996 and doubled since 2001; correspondingly, the number of patients receiving MMT had grown approximately 30-fold since 1996 and 6-fold since 2001.
▸ These indicators show a massive expansion of MMT availability and use, and hence can be interpreted as success indicators in regards to the objective of MMT policy reforms in the late 1990s to improve access to MMT. However, they might also raise questions regarding the evidence for and appropriateness of current treatment practice.
▸ Most MMT-prescribing physicians are community-based GPs, suggesting that MMT provision and care has effectively been moved from specialized, institutional clinics and integrated into more community-based health services, likely contributing positively to MMT access.
▸ There were substantial intra-province differences in MMT service uptake, which might be a function of either differences in MMT need and demand or regional system issues. Also, MMT utilization rates are now higher in predominantly rural than in urban regions in Ontario.
Points de repère du rédacteur
▸ Cette étude cherchait à connaître les tendances actuelles dans le traitement de maintien à la méthadone (TMM) en Ontario. En 2014, le nombre de médecins prescrivant le MTM en Ontario était environ 6 fois plus élevé qu’en 2001, et il a doublé depuis ce temps; parallèlement, le nombre de patients ainsi traités était environ 30 fois plus élevé qu’en 1996 et 6 fois plus élevé qu’en 2001.
▸ Ces chiffres indiquent une augmentation massive de la disponibilité et de l’usage du MTM, ce qui peut être interprété comme un indicateur de succès, compte tenu des modifications à la politique survenues à la fin de 1990 et dont le but était d’augmenter l’accès à ce traitement. Toutefois, cela pourrait aussi soulever des questions concernant les données probantes à l’appui de l’actuelle pratique de traitement et sa pertinence.
▸ La plupart des médecins qui prescrivent le TMM sont des omnipraticiens qui pratiquent dans la communauté, ce qui permet de croire que la prescription du TMM ne relève plus de cliniques institutionnelles spécialisées, mais qu’elle est maintenant intégrée aux services de santé communautaires, contribuant vraisemblablement à améliorer l’accès au TMM.
▸ Il y avait des différences intraprovinciales importantes dans l’utilisation du TMM. Ces différences pourraient résulter soit de différences quant au besoin et à la demande de TMM, soit de problèmes au niveau des systèmes régionaux. De plus, en Ontario, les taux d’utilisation du TMM sont plus élevés dans les régions principalement rurales que dans les zones urbaines.
Footnotes
Contributors
All authors contributed to the concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}