


Abstract
Objective To determine how often primary health care providers (PHCPs) in family medicine groups (FMGs) assess physical activity (PA) levels, provide PA counseling (PAC), and refer patients to exercise professionals; to describe patients’ PA levels, physical fitness, and satisfaction regarding their PA management in FMGs; to describe available PA materials in FMGs and PHCPs’ PAC self-efficacy and PA knowledge; and to identify characteristics of patients and PHCPs that determine the assessment of PA and PAC provided by PHCPs.
Design Cross-sectional study using questionnaires and a medical chart audit.
Setting Ten FMGs within the Integrated University Health Network of the Centre hospitalier universitaire de Sherbrooke in Quebec.
Participants Forty FPs, 24 nurses, and 439 patients.
Main outcome measures Assessment of PA level and PAC provided by PHCPs.
Results Overall, 51.9% of the patients had had their PA level assessed during the past 18 months, but only 21.6% received PAC from at least 1 of the PHCPs. Similar percentages were found among the inactive (n = 244) and more active (n = 195) patients. The median PAC self-efficacy score of PHCPs was 70.2% (interquartile range 52.0% to 84.7%) and the median PA knowledge score was 45.8% (interquartile range 41.7% to 54.2%), with no significant differences between nurses and FPs. In multivariate analysis, 34% of the variance in PAC provided was explained by assessment of PA level, overweight or obese status, type 2 diabetes or prediabetes, less FP experience, lower patient annual family income, more nurse encounters, and a higher patient physical component summary of quality of life.
Conclusion The rates of assessment of PA and provision of PAC in Quebec FMGs were low, even though most of the patients were inactive. Initiatives to support PHCPs and more resources to assess PA levels and provide PAC should be implemented.
Regular physical activity (PA) has many physical and mental health benefits.1–6 According to the World Health Organization, physical inactivity is the fourth leading cause of mortality worldwide.7 Canadian recommendations are to perform “150 min of moderate- to vigorous-intensity aerobic physical activity per week, in bouts of 10 min or more”8 to achieve health promotion and disease prevention and management. However, 80% of Canadian adults did not reach these recommended levels in 2012 to 2013.9
Primary health care providers (PHCPs) are in a key position to address the problem of inactivity in the population as, in 2013, 85% of Canadians reported having a regular medical doctor.10 Although evidence on long-term effects of interventions to promote PA in primary care is lacking, promotion of PA to sedentary adults recruited in primary care statistically significantly increases PA levels according to a meta-analysis of randomized controlled trials.11
Nevertheless, the level of PA counseling (PAC) reported by patients in North America ranges from 15% to 62%,12–17 in contrast to that reported by FPs, ranging from 56% to 85%.13,18–20 To our knowledge, few studies have provided information on Canadian populations, and none has used medical charts to analyze assessment of PA level and provision of PAC.18,19,21–23 In addition, studies focused on FPs without including other PHCPs such as nurses.
Information about primary care in this area is essential for the development of quality improvement initiatives. Thus, the main purpose of this study was to determine how often PHCPs assess PA levels, provide PAC, and refer patients to exercise professionals. Second, the study aimed to describe self-reported patients’ PA level, physical fitness, and satisfaction regarding their care related to PA in family medicine groups (FMGs). We also aimed to describe PA materials available in FMGs and PHCPs’ PAC self-efficacy and PA knowledge. Finally, we aimed to identify the characteristics that determine assessment of PA level and provision of PAC.
METHODS
Population
The data used come from the baseline evaluations of a cluster-randomized trial.24,25 Family physicians, nurses, and patients were recruited between 2009 and 2012 in 10 FMGs within the University of Sherbrooke health network in Quebec. Patient inclusion criteria and the detailed protocol have been described elsewhere.24 The University of Sherbrooke and the Centre hospitalier universitaire de Sherbrooke research ethics review boards approved the study protocol. Briefly, 2 groups of patients were recruited: the targeted diseases group (patients with hypertension or dysglycemia in addition to a body mass index of 25 kg/m2 or greater who had seen a physician at least 4 times in the past 2 years) and the regular follow-up group (patients without the targeted chronic diseases who had seen a physician during the past 2 years). However, we pooled all the participants together for the analyses in this study.
Medical history, PA management, and sociodemographic data.
Sociodemographic data and smoking status were self-reported. An 18-month retrospective medical chart review was performed by experienced research personnel using a standardized grid to evaluate whether FPs, nurses, and dietitians in the FMGs performed an assessment of PA level (yes or no), provided PAC, offered self-monitoring tools (pedometer or diary), or referred patients to exercise professionals. More precisely, the assessment of PA level was considered to have been performed if exercise methods were described or a general evaluation of PA level, such as inactive or active, was documented in the medical chart. Physical activity counseling was considered to have been provided if recommendations, PA objectives, or suggestions of PA methods or parameters were written in the chart. Patient comorbidities were also extracted from medical charts.
Anthropometric measures.
Standard methods were used by the research team to obtain height, weight, and waist circumference with calibrated instruments.24–26
Physical fitness.
Functional capacity, peak grip strength, and peak isometric quadriceps strength were assessed by the research team27 with a 6-minute walking test in an indoor 20-m corridor,28 a hand dynamometer,29,30 and a hand-held force dynamometer,31 respectively.
Levels of recreational PA and sedentary behaviour.
A questionnaire from the Canadian Community Health Survey32 was used to evaluate recreational PA during the past 3 months and the amount of time spent viewing television during a normal week. The PA index was obtained by summing the energy expenditure of each recreational PA performed by the patient. Participants were categorized as inactive (< 1.5 kcal/kg/d), moderately active (1.5 to < 3 kcal/kg/d), or active (≥ 3 kcal/kg/d).
Health-related quality of life.
Physical and mental summary scores of the validated 36-Item Short Form Health Survey were used to assess health-related quality of life.33
Satisfaction regarding PA management.
Based on visual analogue scales (0 to 100 mm), 7 questions were used to evaluate patient satisfaction with PHCP expertise, recommendations, explanations, approach, listening, understanding, and time spent on the subject of PA. The average score from each question was used to obtain a total score. In addition, patients were asked if they met with an exercise professional.
Evaluation of FPs and nurses
All the questionnaires were administered to FPs and nurses after they signed the consent form. Sociodemographic data and years of experience were self-reported. Physical activity counseling self-efficacy of FPs and nurses was evaluated with a 100-mm visual analogue scale.24
To assess knowledge of PA benefits and recommendations, FPs and nurses responded to 1 multiple-choice question (How many steps per day should someone minimally do to not be considered inactive?) and 3 short-answer questions (Name 4 benefits of PA on health; name 3 types of recommended PA; write the recommended duration according to the PA intensity performed). Percentages were calculated from the total score out of 20 points.
Materials available in FMGs
Family medicine group managers were interviewed regarding whether Canadian PA guideline materials, leaflets on PA, and self-monitoring tools such as pedometers were available for patients.24
Statistical analyses
Data were analyzed with SPSS, version 16.0. The normality of data distribution was evaluated with Shapiro-Wilk tests, frequency histograms, and quantile-quantile plots. Bivariate logistic regression analyses were used to determine associations of independent variables with dependent variables. Variables associated in univariate analyses (P < .2) were tested in a log-likelihood ratio forward logistic model (multivariate analysis). Among collinear data (eg, body mass index, waist circumference, overweight or obese status, FP age, FP experience), the independent variable that was the most significantly associated with the dependent variable in univariate analyses was used in the multivariate analysis. In the second multivariate analysis model, the number of comorbidities was replaced by comorbidities significantly associated with dependent variables. No analysis of nurse-related variables was performed, given that patients could have had no visit with a nurse or visited more than 1 nurse. Characteristics of FPs and nurses were compared using Mann-Whitney U tests. A comparison of satisfaction among patients who had had an assessment of PA level or not, and received PAC or not, by FPs was performed with Student t tests and Mann-Whitney U tests for comparison with nurse and dietitian data. The null hypothesis was rejected at P < .05.
RESULTS
Participant characteristics
Among the 439 patients, 181 were recruited in the targeted diseases group and 258 in the regular follow-up group. Forty FPs (median age 49.9 years, interquartile range [IQR] 43.9 to 57.3 years, n = 38, 62.5% women) and 24 nurses (median [IQR] age 33.5 [26.7 to 41.4] years, n = 22, 91.7% women) participated in the study. Family physicians had significantly more years of experience compared with nurses (median [IQR] 22.0 [12.0 to 32.0] years, n = 39; vs 10.0 [5.2 to 20.8] years, n = 24; P < .05). No significant differences were found between FPs and nurses in PA knowledge (median [IQR] score 45.8% [41.7% to 58.3%], n = 39; vs 45.8% [41.7% to 53.1%], n = 24) and PAC self-efficacy (median [IQR] score 68.2% [50.8% to 81.5%], n = 38; vs 77.7% [57.6% to 87.4%], n = 23).
Management of PA
Overall, 51.9% of the patients had had their PA level assessed during the past 18 months, but only 21.6% received PAC from at least 1 of the PHCPs (Figure 1). Similar percentages were found among the inactive (n = 244) and more active (n = 195) patients. Of the inactive patients, 48.8% had their PA level assessed during the past 18 months, and 23.4% received PAC by at least 1 of the PHCPs; there was no significant difference with active patients.
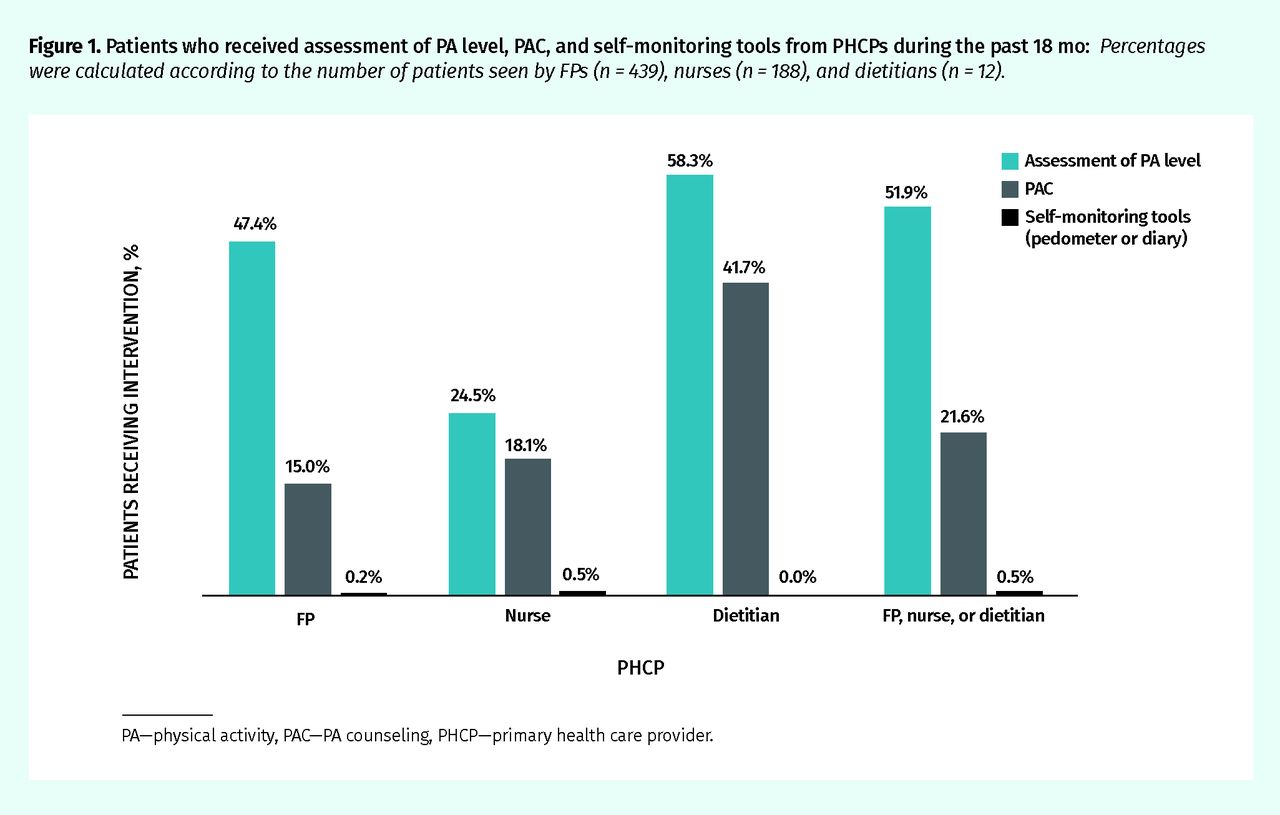
Patients who received assessment of PA level, PAC, and self-monitoring tools from PHCPs during the past 18 mo: Percentages were calculated according to the number of patients seen by FPs (n = 439), nurses (n = 188), and dietitians (n = 12).
PA—physical activity, PAC—PA counseling, PHCP—primary health care provider.
The median PAC self-efficacy score of PHCPs was 70.2% (IQR 52.0% to 84.7%) and the median PA knowledge score was 45.8% (IQR 41.7% to 54.2%), with no significant differences between nurses and FPs.
According to the medical charts, FPs had referred 0.2% of their patients to an exercise professional during the previous 18 months; however, 8.0% of patients reported having met an exercise professional during the past 24 months (5.6% in a private office, 1.9% in a community health centre, and 0.5% in an FMG).
Assessment of PA level was performed by FPs during annual visits (60.1%), follow-up visits (37.5%), and unplanned visits (2.4%). Physical activity counseling was provided by FPs during annual visits (52.2%), follow-up visits (46.3%), and unplanned visits (1.5%).
Median (IQR) patient satisfaction with PA management was 77.8% (58.6% to 90.9%) for FPs (n = 439 patients), 77.3% (52.5% to 93.1%) for nurses (n = 112 patients), and 84.7% (67.7% to 94.7%) for dietitians (n = 84 patients). Patients who reported an assessment of PA level by FPs were significantly more satisfied compared with those who reported no assessment by FPs (77.3% vs 68.8%, P < .001), as did those who had PAC provided by FPs compared with those who reported no PAC by FPs (80.0% vs 71.5%, P = .002). No significant difference between groups was observed for analyses of nurse and dietitian data.
According to FMG managers, 90% of FMGs had leaflets on PA, 10% had self-monitoring tools such as pedometers, and 50% had Canadian PA guidelines in the offices but not in the waiting rooms.
In multivariate analysis, 34% of the variance in PAC provided was explained by assessment of PA level, overweight or obese status, type 2 diabetes or prediabetes, less FP experience, lower patient annual family income, more nurse encounters, and a higher patient physical component summary of quality of life. Univariate and multivariate analyses are presented in Tables 1 to 4.
Patient characteristics and assessment of PA level and PAC provided by FPs, nurses, or dietitians during the past 18 mo: Variables in bold were included in the multivariate analysis as independent variables.
Associations between FP and FMG characteristics and the assessment of PA level and PAC provided by FPs, nurses, or dietitians during the past 18 mo: PAC performed by at least 1 PHCP was significantly associated with the assessment of PA level performed by at least 1 PHCP (OR [95% CI] 5.05 [2.93 to 8.72], P < .01). Variables in bold were included in the multivariate analysis as independent variables.
Multivariate analysis to explain the assessment of PA provided by FPs, nurses, or dietitians during the past 18 mo: Nagelkerke R2 = 0.20; N = 339 patients.
Multivariate analysis to explain provision of PAC by FPs, nurses, or dietitians during the past 18 mo: In model 2, the no. of comorbidities was replaced by the comorbidities significantly associated with the dependent variables. Nagelkerke R2 = 0.31 for model 1; Nagelkerke R2 = 0.34 for model 2; N = 418 patients.
DISCUSSION
Our results highlight that rates of assessment of PA level and provision of PAC in Quebec FMGs are low, although more than half of the patients were inactive and 78.8% were overweight or obese. Patient satisfaction with PA management was high irrespective of the PHCP they saw; however, the satisfaction rate was higher in patients who had PA management by FPs. Overweight or obese individuals, those with type 2 diabetes, and those who had a PA level assessment, more nurse encounters, and a higher physical component summary of quality of life were more likely to receive PAC by PHCPs. We also showed that less FP experience and lower annual family income were associated with additional PAC.
In this study, the percentage of participants receiving PAC by FPs is lower (15.0%) than in previous studies of Canadian FPs. Petrella et al18,19 reported that 70% of surveyed FPs provided PAC. In a study of residents of Halifax, NS, about 42% of 1607 participants reported frequently receiving advice on exercise from their FPs.23 On the other hand, Kennedy and Meeuwisse34 found that only 12% of 330 Canadian FPs reported providing exercise counseling in 76% to 100% of their patients. Geographic coverage, wording of questions, period of reference, and data collection (self-reported vs medical charts) might explain this discrepancy. The low rate of PAC reported is probably explained by several barriers faced by PHCPs (lack of time, skills, tools, and reimbursement),34 but it is also possible that we have underestimated the frequency of PAC, as it might be performed but not systematically recorded in the medical charts.
In contrast with our results, some studies found that older and more experienced FPs reported more PAC.18,35 The lower provision of PAC among most FPs in our study could be explained by the fact that older FPs might report less information in medical charts or by recent changes in FPs’ training related to recommendations.36–38
Numerous studies also reported that individuals with obesity received more PAC by FPs.15,39,40 Teoh et al41 also showed that Canadians with type 2 diabetes were more often advised to increase their PA compared with individuals who did not have diabetes. Physical activity counseling seems to be provided more often by FPs to manage these chronic diseases, thus missing the opportunity to perform primary prevention. The number of visits with FPs is associated with provision of PAC in several studies.16,36,37 Our results showed that nurse encounters are an independent factor associated with PAC. Nurses in Quebec FMGs often share follow-up of patients with chronic diseases, which probably explains this association.
Strengths and limitations
The important strengths of this study were considering PAC in an interdisciplinary context, and using patient measurements and longitudinal chart audit data. However, several limitations should be considered when interpreting our results. The recruitment procedure relied on volunteer participation and specific inclusion criteria designed for an interventional study, which might have resulted in selection bias. However, this bias probably induces an overrepresentation of patients who should be targeted for PA intervention. In addition, the PHCP sample size is small, and information about the quality of PAC is missing. Finally, as in all studies using chart audits, results should be interpreted with caution, as it is possible that PHCPs did not always record their interventions.
Conclusion
Rates of assessment of PA and provision of PAC, as reported in medical charts, are insufficient in Quebec FMGs, despite PHCPs being key to addressing inactivity in the population. Initiatives to support PHCPs in PA assessment and PAC should be studied.
Notes
Editor’s key points
▸ This study found that rates of assessment of physical activity (PA) level and provision of PA counseling (PAC) in Quebec family medicine groups are low, although more than half of the patients were inactive and 78.8% were overweight or obese.
▸ Patient satisfaction with PA management was high irrespective of the primary health care provider they saw; however, the satisfaction rate was higher in patients who had PA management by FPs.
▸ Overweight or obese individuals, those with type 2 diabetes, and those who had a PA level assessment, more nurse encounters, and a higher physical component summary of quality of life were more likely to receive PAC by primary health care providers. As well, less FP experience and lower annual family income were associated with additional PAC.
Points de repère du rédacteur
▸ Cette étude a observé que dans les groupes de médecine de famille du Québec, on faisait peu d’évaluation et de counseling relativement à l’activité (AP) pratiquée par les patients, malgré le fait que plus de la moitié des patients étaient sédentaires et que 78,8 % d’entre eux présentaient un surpoids ou une obésité.
▸ Les patients appréciaient beaucoup qu’on aborde le sujet de l’AP, quel que soit le soignant de première ligne qui le faisait; cependant, ils étaient davantage satisfaits si c’était un MF qui le faisait.
▸ Les personnes obèses ou avec surpoids, celles qui avaient un diabète de type 2, et celles dont le niveau d’AP avait été évalué, qui avaient eu plus de rencontres avec un infirmier ou qui voyaient l’AP comme une composante importante de la qualité de vie étaient plus susceptibles d’avoir reçu des conseils d’un soignant de première ligne. De même, les patients qui avaient rencontré moins de MF et qui avaient un revenu familial annuel moins élevé avaient tendance à recevoir plus de conseils sur l’AP.
Footnotes
Contributors
All authors contributed to the concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada





{kind=link}