


Abstract
Objective To demonstrate how family physicians can contribute to a piece of the journey of improving quality-of-life outcomes for people with intellectual and developmental disabilities (IDD) when they undergo the transition from adolescence to adulthood.
Sources of information The “Primary care of adults with intellectual and developmental disabilities. 2018 Canadian consensus guidelines” literature review and interdisciplinary input.
Main message Family physicians should be proactive in anticipating and supporting the transition of people with IDD from adolescence to adulthood. Interventions should be guided by a developmental perspective regarding the person with IDD and a life-cycle approach to supporting families. Family physicians also have a role in helping people with IDD and their families to navigate successfully through changing community-based support systems in their province, especially health care and social services systems. Therefore, family physicians should be aware of current services available in their regions.
Conclusion Community and team-based family physicians can optimize the quality of life of people with IDD and their families by adopting a proactive developmental and systems approach to preparing youth with IDD for adulthood. In doing so, they exemplify the 4 principles of family medicine.
Case description
Sarah, an 18-year-old, single woman with an intellectual and developmental disability (IDD), and her family are facing a daunting transition to adult life. Sarah is currently in school and is receiving primary care from her pediatrician and associated pediatric rehabilitation services. Sarah has an IDD in the moderate range (corresponding to an age equivalence of 6 to 9 years).1 She also has several health challenges associated with cerebral palsy. These include impaired swallowing, difficulties articulating words, scoliosis, hip dislocations, constipation, and epilepsy. To reduce her risk of aspiration, Sarah has been receiving nutrition and hydration through a gastrojejunal tube since the age of 6 years. Sarah’s family is feeling overwhelmed as they grapple with her impending transition from their familiar pediatrician and pediatric specialists to you, her new family physician.
Sarah and her parents come to see you in your office. Sarah’s parents express their appreciation of your wheelchair-accessible office and your staff bringing them directly from the busy waiting room area into a quiet examination room. Sarah’s parents explain that she lives with them and her 3 siblings, including her younger sister with whom she is closest. They also explain that Sarah communicates nonverbally with vocalizations, gestures, and signs, and by using a tablet-based communication system. Sarah’s mother and father seek your advice regarding new premenstrual symptoms Sarah is experiencing and the recent onset of seizures following 3 years of being seizure-free. A pediatric neurologist assessed Sarah 6 months ago, and her parents brought a copy of this consultation report along with a thick binder of medical records. They ask you whether you are willing to be Sarah’s family physician and to help them get connected with an adult neurologist and other specialized services.
Sources of information
The 2018 Canadian consensus guidelines for primary care of adults with IDD were informed by a literature review and interdisciplinary input. Guideline 12 of the Canadian consensus guidelines for primary care of adults with IDD recommends 3 actions related to transitions.2 The first is to participate in and promote early preparations for transitions using a person-centred, integrated model of care that includes the person with IDD, family, caregivers, and other members of the care team. These preparations should be guided by the perspective that such life-cycle transitions raise developmental challenges for individuals and families for which they will need emotional, behavioural, social, and spiritual supports, and the second recommendation is to proactively engage such supports to enhance resilience and coping skills.
The third recommended action is to develop and regularly review and update a transition plan. A transition plan typically includes arrangements to transfer the person with IDD to appropriate health and social services, exchange health information with adult primary care providers, and develop a strategy for managing crises. This plan should be guided by the perspective that such transitions for a person with IDD and his or her family involve systems issues as well as personal growth and development.
This review expands on the developmental and systems issues that inform guideline 12 and discusses the roles of family physicians in helping people with IDD and their families to address them. We refer to a transitions tool kit3 that provides “how to” advice and resources for implementing guideline 12. Family physicians can make an important and unique contribution to enhancing the health and quality of life of people like Sarah and her family who are undergoing a transition to adult life. These individuals and families can teach us invaluable lessons about what the principles of family medicine mean in practice.2
Main message
Transitions as a developmental issue.
Transitions often represent changes in expectations regarding an individual’s cognitive and adaptive functioning and the social roles they undertake as they age. This is why people with IDD and their families typically identify times of transition as among the most challenging times of life.4
Physicians working with youth with IDD (eg, family physicians, pediatricians, developmental pediatricians) should draw on frameworks that are informed by developmental psychology as guides to thinking about appropriate health care interventions.5–9 Child psychologists such as Piaget, Erikson, and Gesell contributed to understanding development as an evolutionary process that occurs over a predictable sequence of stages, and each stage is associated with particular skills, roles, and competencies. Their work fostered the creation of developmental scales and checklists from which children could be measured and compared in relation to physical and cognitive norms at standardized stages.10,11
Key milestones of “successful” adult life generally include independent living, employment, and interpersonal and intimate relationships. Preparing youth for achieving developmental tasks and meeting expectations of certain future contexts and social roles will ease their transition to adult life. For example, adults are expected to develop independence and self-reliance in fulfilling roles and responsibilities associated with managing their daily life and employment. By contrast, it is acceptable for children to be dependent on their parents until they develop the skills and competencies they need to fulfil these roles and responsibilities by themselves.
When providing care for people with IDD, a challenge for family physicians is to understand how markers of typical development in the general population might not apply to people with IDD. Research shows that people with IDD experience considerable physical and mental health problems during life-stage and service transitions, which are often associated with changes to familiar environments, social circles, and the nature and level of supports.12–14 Many people with IDD, for example, stay in publicly funded school until they are about 21 years of age. But they must transfer from child to adult health services at 18 years of age when they also become eligible for social services in the adult developmental sector. Family physicians need to think about the emotional, behavioural, social, and spiritual challenges that accompany these changes for people with IDD, as they play an important role in preventing and addressing these associated health and social problems.
When an adolescent with IDD is in transition to adult life, his or her family will also need to adjust and adapt to the needs of the person with IDD. While times of transition present opportunities and risks to the quality of life of people with IDD, similar opportunities and risks arise for families with 1 or more members with IDD. The success of an adolescent with IDD’s transition to adult life will have a considerable effect on the well-being of his or her family, including the health of family members, often mothers, who take on caregiving roles. Family caregivers also experience difficult dilemmas and decisions in continuing to provide high levels of care to adult children, but also regarding “letting go” of their caregiving roles and responsibilities as they also age.15,16 Family physicians can play an important role in supporting families of youth with IDD who are in transition to adult life, particularly family caregivers.17
Transitions as a systems issue.
In addition to addressing developmental issues during transitions to adult life for youth with IDD and their families, a related task is to address the continuity and appropriateness of the systems of support for them. One role for family physicians is to engage and work proactively with colleagues in health care and other systems (eg, education, social supports, leisure and recreation, legal) to identify needs early, before the transition, and to designate responsibilities for coordinating, navigating, and integrating health care.
Many authors recommend that planning for the transition to adult life should begin as early as age 12 to 16 years.18–20 This allows sufficient time to develop a transition plan and to implement aspects of this plan, such as the development of relevant skills for adulthood. Such planning is best done during the relatively stable phase of adolescent school life. The transition to adult life can be regarded as successful to the extent that the individual with IDD and his or her family’s wishes and hopes for the adult phase of life that have been incorporated into the transition plan are being realized in a manner that they envisioned.
As shown in Figure 1, Sarah’s health care transition plan (adapted from the Developmental Disabilities Primary Care Initiative)3 is comprehensive in scope and identifies skills and supports that Sarah and her family will need during the early adult phase of life. It is mandatory in schools for people with IDD in a special education program to create a transition plan, which family physicians can refer to as a starting point. In addition to addressing the health care needs of the person with IDD and his or her family, transition plans also address vocational and social issues such as inclusive postsecondary education, supported employment, supported living, and social-leisure-community engagement.21 Such aspects of a transition plan are outlined in detail in a transition readiness tool,3,18 which will not be described here but which is available online (surreyplace.ca/ddprimarycare/tools/general-health/transitions).3 What is important to highlight here, is the role family physicians can play in developing, implementing, reviewing, and updating transition plans in accord with the principles of family medicine.18
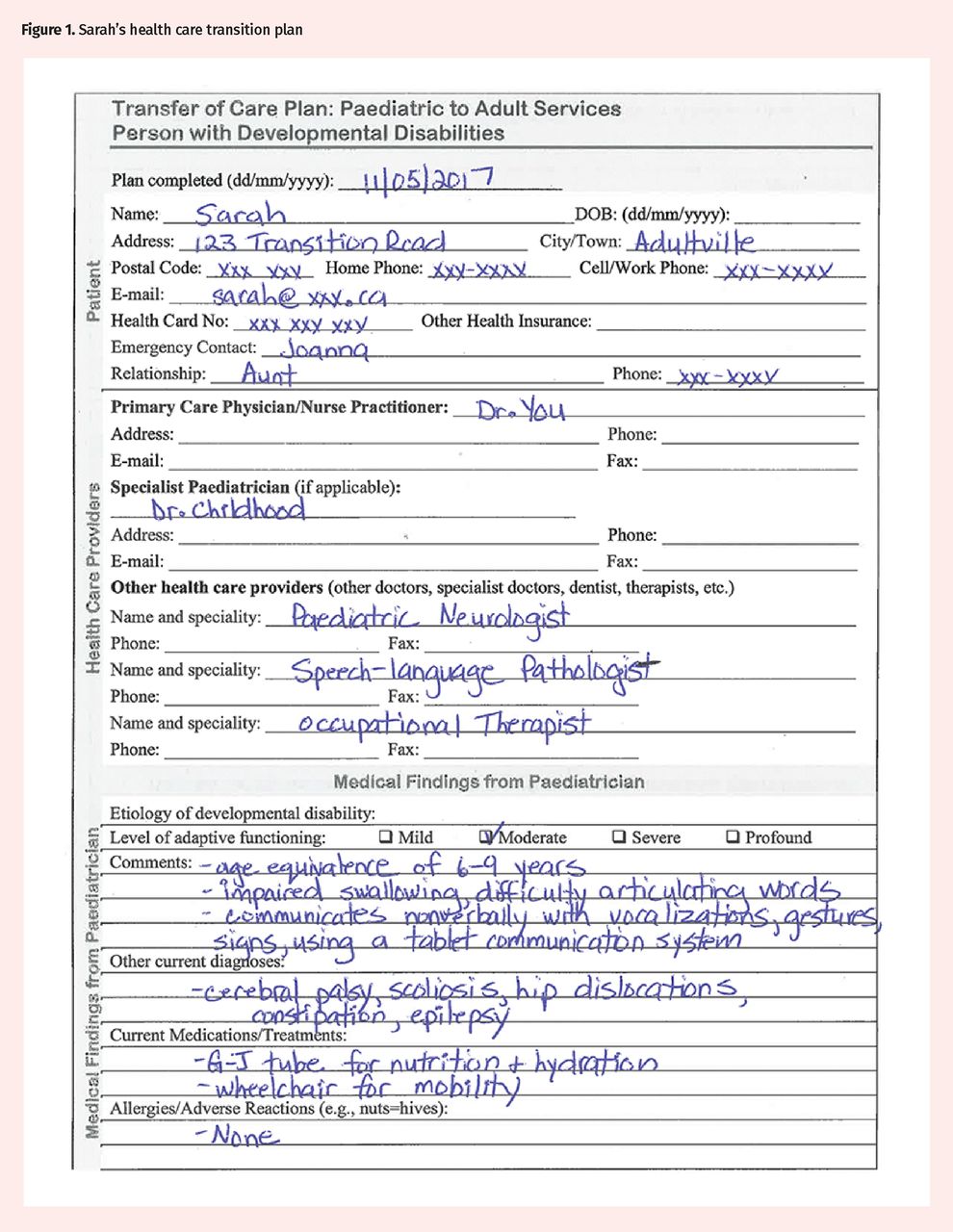

Sarah’s health care transition plan
AAP—American Academy of Pediatrics, ACFP—American Academy of Family Physicians, ACOP—American College of Physicians, DD—developmental disabilities, G-J— gastrojejunal, OT—occupational therapist, SLP—speech-language pathologist.
Adapted from the Developmental Disabilities Primary Care Initiative.3
Role of family physicians.
The various roles that family physicians and other primary care providers can and should play in supporting people with IDD and their families during the transition to adult life can be framed using the 4 principles of family medicine.22
First, the relationship between the family physician and the person with IDD and his or her family is central to health care. The family physician should ensure that the person with IDD and his or her family participate in the planning and implementing of the transition plan. This might entail encouraging and supporting the young person with IDD in decision making. In Sarah’s case, her family physician will need to distinguish between her expressive and receptive communication skills, and employ specific supports to assist with her communication. Sarah’s family physician might also consider each family member’s life stage and provide supportive counseling to each person regarding his or her relationship with Sarah and the various roles he or she is attempting to manage as a family member or caregiver (eg, benefits and risks of a parent also assuming the role of an educator or advocate). In developing and implementing plans, both the well-being of Sarah and that of her family should be kept in mind.
Second, the family physician, as a skilled clinician, should be able to identify health and developmental needs of people with IDD in transition to adult life and those of their families—what involves ongoing care and what can be anticipated to change, requiring preventive care or additional health care interventions and supports.
Third, the family physician, as a resource to a defined population (in this case, persons with IDD in transition to adult life and their families), should be aware of best practices for successful transitions and the supports that adolescents with IDD and their families might need as they face the challenges of changing roles and responsibilities, and of assuming others.5,6,8,18,23
Fourth, the family physician, as a community-based practitioner, should be an advocate for a comprehensive case management approach to developing and implementing a successful transition plan. In addition to addressing health care needs, such a plan needs to engage the range of crucial community agencies and services, such as education, college and university, employment, housing, and funding supports. While it is typically beyond the scope of the family physician to lead such planning, he or she can play a role in ensuring that such planning is taking place, that someone, perhaps a member of the family health team, has been identified to take responsibility for implementing aspects of the health plan, and that progress regarding this plan is reviewed and updated on a regular basis, such as annually.
Case resolution
Sarah’s initial presentation illustrates issues related to the transition to adult life. Ideally, transition planning, which in Sarah’s case includes the transfer from her pediatrician to you, should have begun when she was relatively young, such as age 12. If Sarah had begun to see you as her family physician during her adolescent years, you would have established a relationship with her and her family by the time she turned 18 years old. In assuming your role as Sarah’s family physician now, you will need to identify health, allied, and developmental specialists who can continue various aspects of her care, such as an adult neurologist, speech-language pathologist, and occupational therapist.
In developing a transition plan with Sarah, you need to develop and learn a method of communicating with her and supporting her decisions about herself, such as where and how she wishes to live, work, learn, and play. In Sarah’s case, although she does not speak, you learn she understands many things and has, in fact, very clear ideas about how she would like to live, which will be used to shape the transition plans.
Conclusion
Family physicians are in an important position to be involved in personalized transition plans for patients with IDD that will improve the quality of life of people with IDD and their families during key life transitions—such as the transition to adult life. They can do so by adopting developmental and systems perspectives to primary care. They should be cognizant of specific developmental challenges that both people with IDD and their families experience during this life transition and proactively address them to promote resiliency, wellness, and health. They should also collaborate with youth with IDD, their families, and various community systems of support that are available in their regions well in advance of the transition in order to promote continuity of care and the marshaling of new supports that will be necessary. By accepting responsibility for the roles elucidated and implementing those roles with enthusiasm and competence, family physicians exemplify the 4 principles of family medicine. They can become important catalysts for protecting and promoting the health and quality of life of youth with IDD and their families as those youth enter adult life.
Notes
Editor’s key points
▸ Family physicians should be proactive in anticipating and supporting the transition of people with intellectual and developmental disabilities (IDD) from adolescence to adulthood. Be willing to provide primary care to youth with IDD as young as 12 years of age to participate in early transition planning to early adult life.
▸ Understand the emotional, behavioural, social, and spiritual challenges associated with the transition of youths with IDD to adult life, as well as challenges faced by their families, and be prepared to proactively address these challenges by engaging with interprofessional supports.
▸ Develop transition plans that ensure continuity and appropriateness of health care and social supports. There are tools that can help with this. A key role and responsibility of the family physician is to oversee and support the effective implementation of these transition plans and to review and update them regularly.
▸ Be sure to engage the youth with IDD and his or her family in developing this transition plan.
Points de repère du rédacteur
▸ Les médecins de famille devraient agir de façon proactive en prévoyant et en appuyant la transition entre l’adolescence et l’âge adulte chez les personnes ayant des déficiences intellectuelles et développementales (DID). Ils doivent être disposés à dispenser des soins de première ligne à des jeunes ayant des DID âgés d’aussi peu que 12 ans pour qu’ils puissent participer à la planification précoce de la transition vers l’âge adulte.
▸ Ils devraient comprendre les difficultés émotionnelles, comportementales, sociales et spirituelles associées à la transition des jeunes ayant des DID vers l’âge adulte, de même que les défis auxquels font face leur famille, et être disposés à s’attaquer proactivement à ces difficultés en s’entourant d’un soutien interprofessionnel.
▸ Ils devraient élaborer des plans de transition qui assurent la continuité et la nature appropriée des soins de santé et des mesures de soutien social. Il existe des outils à cet effet. Superviser et appuyer la mise en œuvre efficace de ces plans de transition, et les revoir et les actualiser régulièrement, font partie du rôle et des responsabilités clés du médecin de famille.
▸ Ils devraient mobiliser les jeunes ayant des DID et leur famille afin qu’ils participent à l’élaboration du plan de transition.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
All authors contributed to the literature review and interpretation, and to preparing the manuscript for submission.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.