


The Self Learning Program is a continuing education initiative developed by the College of Family Physicians of Canada. This program provides family physicians with information curated from peer-reviewed articles and tests knowledge with clinical questions.
Methods
Using participants’ evaluations (up to mid-2018) of 2017 Self Learning modules, we identified the 10 articles rated as most likely to affect practice. A sample article is provided in Figure 1.1 For each of the 10 articles, we have written a bottom line and an article summary, provided other relevant articles, and outlined any limitations. We also identified Self Learning answers that required modification based on review of the broader evidence base.

Top 10 articles
Are blood pressure (BP) measurements taken over clothing equivalent to measurements taken on a bare arm?
Bottom line: Blood pressure measurements should be performed on a bare arm when possible. Measurements done over a sleeved arm in elderly patients might result in readings that are higher and more variable.
Self Learning content: A study of 186 primary care patients in Japan compared BP measured by an automated cuff over bare and sleeved arms.2 Three BP measurements were completed and averaged for each method. Participants were a mean of 75 years old, 61% were female, and 64% were hypertensive. Compared with measurements taken on a bare arm, sleeved-arm BP meas urements were higher by 3.8 mm Hg for systolic BP (SBP) and 5.2 mm Hg for diastolic BP. The authors recommended BP measurements be taken on a bare arm.
Context: The Canadian hypertension guideline suggests that BP should be measured on bare arms.3 Eight earlier studies suggested no clinical differences when measuring BP over sleeved versus bare arms (range −1.7 to 1.0 mm Hg).4–6 However, the most recent study done in long-term care patients found that, compared with bare arms, diastolic BP was 4.6 mm Hg higher compared with that measured over thin shirts and 8 to 10 mm Hg higher when taken over a shirt and sweater.6
Limitations: Studies finding that measurements over sleeved arms resulted in higher BP were in elderly patients (mean age 74 to 87 years), while those finding little effect from sleeves were in middle-aged patients (mean age 44 to 62 years).2,4–6
For the prevention of migraine-type headaches, is 3 mg of melatonin daily as effective as 25 mg of amitriptyline daily?
Bottom line: Melatonin and amitriptyline were generally similarly effective for migraine prevention, and both were better than placebo. While melatonin was superior to amitriptyline for 1 outcome in 1 adult study, a pediatric trial found amitriptyline to be superior overall. At present, it is likely reasonable to consider either as therapy.
Self Learning content: A double-blind randomized controlled trial (RCT) of 178 patients (mean age 37, 75% female) compared melatonin (3 mg), amitriptyline (25 mg), and placebo.7 Melatonin and amitriptyline decreased migraine days per month similarly (−2.7 and −2.2 days, respectively) but more than placebo (−1.1 days). Compared with placebo, both also reduced headache intensity (1.3-point improvement on a 10-point scale) and use of analgesics, as well as mean migraine duration (4- to 5-hour reduction). More people achieved a 50% decrease in headache frequency using melatonin (54%) versus amitriptyline (39%) and placebo (20%).
Context: A systematic review of 7 studies of melatonin (4 RCTs, 3 observational trials) found improved migraine prophylaxis in terms of headache intensity, duration, and proportion of responders (patients with a greater than 50% reduction in the number of headache days) compared with placebo.8 A pediatric RCT found amitriptyline to be more effective than melatonin in reducing headache frequency, severity, duration, and disability.9
Limitations: Considering direct comparisons, 1 outcome (of several) favoured melatonin in 1 RCT,7 but another RCT found amitriptyline to be better.9
Are complementary health products effective for treating and preventing the common cold?
Bottom line: Zinc might reduce the duration of illness and improve cold symptoms, while honey has been found to reduce nighttime coughing in children. Findings on the benefit of saline nasal irrigation are inconsistent, but it might improve symptoms. Probiotics might reduce the number of common colds, but the quality of evidence is low. There is no evidence of benefit for vitamin C, American ginseng, echinacea, or garlic.
Self Learning content: A review article summarized the effectiveness and safety of complementary health approaches for the common cold.10
Zinc: Compared with placebo, zinc might reduce the mean duration of colds by around 1.5 days.11 Zinc can cause taste disturbances and nausea. Intranasal zinc is not recommended (risk of hyposmia).
Honey: A systematic review of 6 RCTs (primarily examining nighttime cough in children) found that on a 7 point-scale (0 to 6), cough improved from a score of 4 to a score of 3 with placebo and by 1.5 points with honey.12 Honey is not recommended in children younger than 1 year old (risk of botulism).
Saline irrigation: Saline irrigation might relieve upper respiratory tract infection symptoms; however, this is based on evidence with a risk of bias.
Probiotics: Probiotics might reduce episodes of upper respiratory tract infection and the duration of episodes by about 2 days compared with placebo.13
Other: There is no evidence of benefit for supplemental vitamin C,14 American ginseng, echinacea, or garlic.
Limitations: Several meta-analyses reporting outcomes for probiotics15,16 and zinc11,17 had heterogeneity among the trials, suggesting inconsistency.
Is 10 days of bismuth quadruple therapy more effective than triple therapy for eradicating Helicobacter pylori?
Bottom line: For eradicating H pylori, bismuth quadruple therapy was 6% more effective than triple therapy but not better than non-bismuth quadruple therapy. Bismuth quadruple therapy was accompanied by slightly poorer tolerability and lower adherence rates.
Self Learning content: In an open-label RCT,18 1620 patients with positive results for H pylori received 30 mg of lansoprazole twice daily and were randomized to 10-day bismuth quadruple therapy (300 mg of bismuth 4 times daily, 500 mg of tetracycline 4 times daily, and 500 mg of metronidazole 3 times daily); to 10-day non-bismuth quadruple therapy (1000 mg of amoxicillin, 500 mg of clarithromycin, and 500 mg of metronidazole, all twice daily); or to 14-day triple therapy (1000 mg of amoxicillin and 500 mg of clarithromycin, both twice daily).18
Bismuth quadruple therapy led to higher H pylori eradication rates than 14 days of triple therapy (90% vs 84%, respectively; number needed to treat [NNT] of 15). The eradication rate for non-bismuth quadruple therapy was not different from that of either of the other groups. Bismuth quadruple therapy was associated with the highest rates of discontinuation due to side effects (10% vs 7% with non-bismuth quadruple therapy and 4% with triple therapy). More patients taking bismuth quadruple therapy had poor adherence (took ≤ 80% of pills): 9% versus 5% with non-bismuth quadruple therapy and 3% with triple therapy.18
Context: The Toronto Consensus guideline recommends a 14-day regimen of bismuth quadruple therapy or non-bismuth quadruple therapy as first-line treatment for H pylori infections.19 Quadruple therapy (10 to 14 days) has been previously shown to be better than 7-day triple therapy.20 While few studies have been published about the relative effectiveness of 14-day non-bismuth quadruple therapy, 1 non-randomized study suggested its superiority over 14-day triple therapy.20
In an uncomplicated urinary tract infection (UTI), does a urine culture negative for bacteria accurately rule out infection?
Bottom line: Symptoms of UTI in women are a strong indicator of infection, and treatment initiation can be considered. Negative urine culture results might not fully rule out UTI.
Self Learning content: An observational survey analyzed bacterial culture data from 220 women with complaints of dysuria, urinary urgency, or increased urinary frequency, and from 86 women without UTI symptoms.21 Urine culture and quantitative polymerase chain reaction (PCR) assays were used to test for bacteria. A quantitative PCR assay accurately determines bacterial presence. In women with UTI symptoms, 81% had positive urine culture results and 96% had positive quantitative PCR findings. In women without symptoms, 11% had positive urine culture results and 12% had positive PCR findings. Of the urine cultures positive for bacteria, 68% were positive for Escherichia coli.
Context: An RCT found that a 3-day course of trimethoprim in women with UTI symptoms and negative urine dipstick results improved symptoms.22 An RCT study of women with UTI symptoms found that targeting antibiotics based on urine dipstick results or midstream urine analysis findings might be more costly than treating with immediate antibiotics or delayed antibiotics (delayed by 48 hours).23
Limitations: Quantitative PCR is not used in practice. Results only apply to uncomplicated UTIs.
Should proton pump inhibitors (PPIs) be deprescribed?
Bottom line: The presented guideline recommends PPIs be decreased, stopped, or changed to “as needed” in adults with resolved reflux symptoms after 4 weeks of PPI treatment. This might result in symptom relapse and reduced satisfaction for 1 in 14 patients. Weekly pill burden could be reduced by about 4 pills.
Self Learning content: The guideline focused on outcomes important to patients, including change in upper gastrointestinal symptoms and pill burden.24 The systematic review found 5 studies comparing abrupt discontinuation of PPIs followed by on-demand use versus continuous PPI use.25 Abrupt discontinuation followed by on-demand PPI use increased both symptom relapse (risk ratio of 1.71, 95% CI 1.31–2.21; number needed to harm [NNH] of 14) and patient dissatisfaction (risk ratio of 1.82, 95% CI 1.26–2.56; NNH = 14) compared with continuous PPI use. Weekly pill burden was reduced by about 4 pills.
Context: An RCT of patients completing an 8-week course of PPI therapy who were then randomized to 40 mg of esomeprazole as needed or 20 mg of esomeprazole once daily found symptoms and satisfaction were not significantly different (P > .05).26 Patients consumed the same average number of milligrams per day of esomeprazole.
Limitations: Clinicians might have a difficult time deprescribing a long-standing PPI owing to relapse symptoms.
Does an SBP target of 120 mm Hg for elderly patients decrease cardiovascular events?
Bottom line: In older adults with elevated cardiovascular disease (CVD) risk, an SBP target of less than 120 mm Hg reduced CVD for 1 in 27 patients and all-cause mortality for 1 in 41, compared with an SBP target of less than 140 mm Hg over 3 years. Clinicians must balance benefits against the potential harms like hypotension, syncope, and acute kidney injury.
Self Learning content: An RCT of 2636 patients at high CVD risk aged 75 or older compared managing hypertension with an SBP target of less than 120 mm Hg (intensive) versus an SBP target of less than 140 mm Hg (stand ard).27 After 3 years, the intensive group achieved a mean SBP of 123 mm Hg versus the standard group at 135 mm Hg. The intensive group had reduced CVD (hazard ratio [HR] of 0.66, 95% CI 0.51–0.85; NNT = 27) and all-cause mortality (HR = 0.67, 95% CI 0.49–0.91; NNT = 41). However, there was a trend toward increased hypotension, syncope, and acute kidney injury (HR = 1.41, 95% CI 0.98–2.04).
Context: The original RCT looked at patients at high CVD risk without an age restriction. The SBP target of less than 120 mm Hg resulted in reduced CVD and all-cause mortality (NNT of 61 and 90, respectively). However, statistically significant increases were seen in hypotension (NNH = 72), syncope (NNH = 91), and acute kidney injury (NNH = 56).28
Limitations: Although differences in adverse events were not statistically significant in the elderly, a low sample size reduced statistical power.27
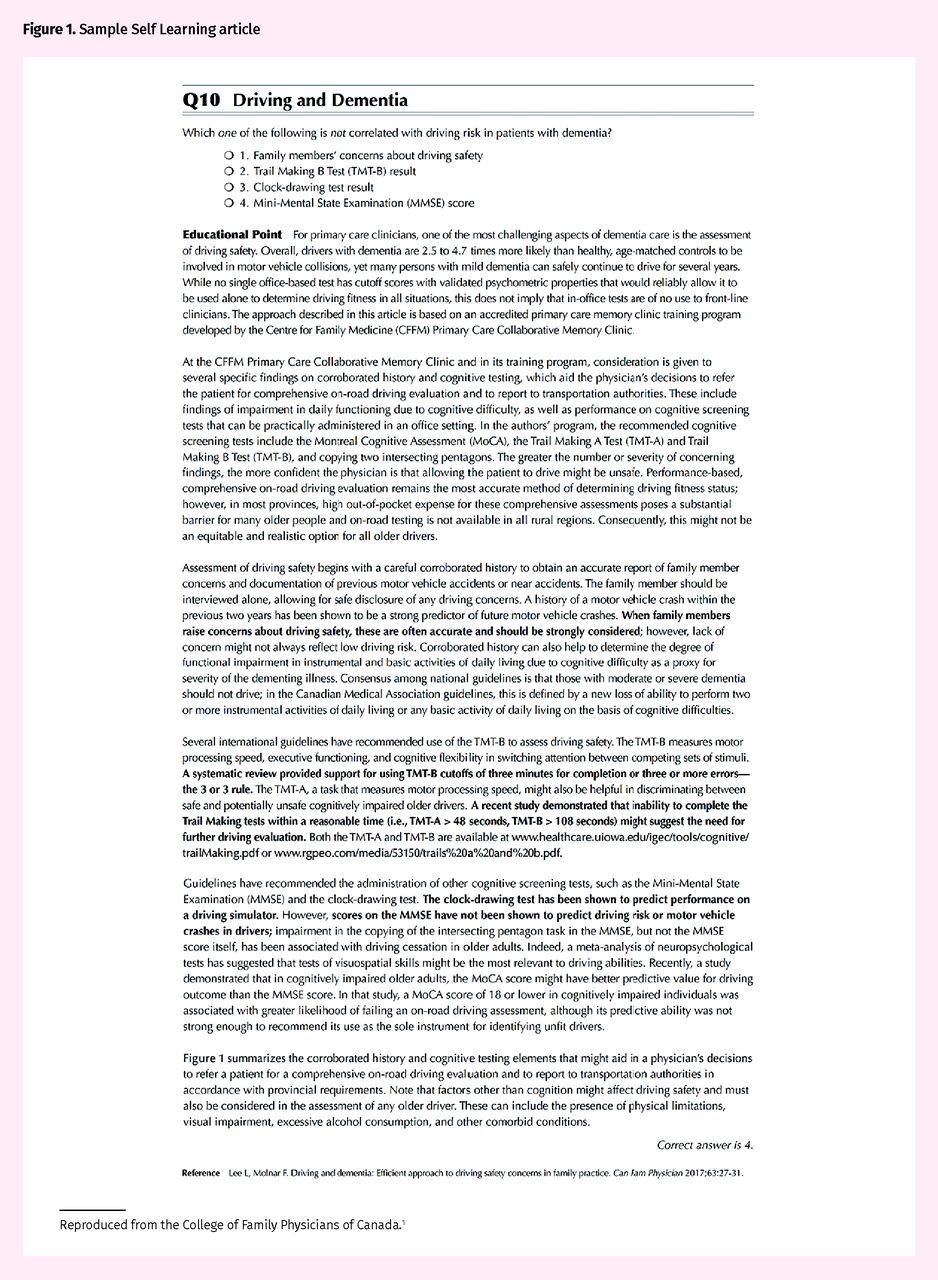
Does the Mini-Mental State Examination (MMSE) predict driving risk in patients with dementia?
Bottom line: The MMSE does not predict driving risk or motor vehicle collision (MVC). However, factors like family concerns, past or near MVC, Montreal Cognitive Assessment (MoCA) findings, the clock-drawing test, and the Trail Making tests (TMTs) A and B can help discern which drivers are at risk. None is definitive and referral for performance-based, comprehensive, on-road driving evaluation provides the best assessment.
Self Learning content: The presented guidance document recommended that clinicians strongly consider that patients with dementia might be unsafe to drive if family members are concerned about driving safety; if the TMT-B takes 3 minutes or longer to complete or patients make 3 or more errors; and if the TMT-A takes longer than 48 seconds.29 These findings suggest a need for driving evaluation. Other factors that might be helpful include findings of the clock-drawing test or drawing intersecting pentagrams; a history of MVC or near collisions; or a MoCA score of 18 or less. The MMSE does not predict driving risk or MVC.
Context: If the TMT-B takes 2 to 3 minutes to complete or the patient makes 2 errors, safety is unclear. Patients are likely safe to drive if the TMT-B takes less than 2 minutes and the patient makes fewer than 2 errors. While not perfect,30 the TMTs (both A and B) are recommended as part of a driving assessment,31,32 with the TMT-B likely being more helpful.31 A MoCA score of 18 or less and clock drawing are also helpful.32 Other studies suggest the importance of family members’ concerns and past or near MVC.33
Limitations: There is no RCT evidence.34 None of the tests is reliable by itself.
Is chronic PPI use associated with any or all of vitamin B12 deficiency, fractures, dementia, or Clostridium difficile infections?
Bottom line: Relatively consistent evidence finds associations between prolonged PPI use and vitamin B12 deficiency, fracture risk, dementia, and C difficile infection. All evidence is from observational studies, leaving these associations at high risk of bias. Regardless, prolonged use of PPIs should be reevaluated and use minimized when feasible.
Self Learning content: A review article of adverse events associated with PPI use was presented.35
Vitamin B12 deficiency: Chronic PPI use was associated with an increased HR of 1.83 (95% CI 1.36–2.46), possibly through lowering intragastric pH and therefore B12 absorption.
Fracture risk: Risk of fracture is increased in men and women.
Dementia: There is a possible increased risk, with an adjusted HR of 1.38 (95% CI 1.04–1.83).
Clostridium difficile: There is an increased relative risk of 1.69 (95% CI 1.40–1.97). The highest risk occurs in patients taking antibiotics in-hospital (NNH = 50 at 14 days).
Context: Findings from other articles add the following.
Vitamin B12 deficiency: A newer systematic review included similar studies but does not provide numbers to estimate risk.36 In a cohort study, vitamin B12 treatment was needed for 4.6% of those not taking antiulcer medications and for 11% of those taking antiulcer medications (including a mix of PPIs and histamine-2–blocking medications).37
Fractures: Risk was approximately 16% for those not taking PPIs and about 22% for those taking PPIs over about 6 years.38 A hip fracture study also found increased risk.39
Dementia: Of 4 studies, 3 found PPI use was associated with higher risk (perhaps about 1.4 times) of dementia.40
Clostridium difficile: Two new meta-analyses found PPI use was associated with C difficile infection, (odds ratio [OR] of approximately 2).41,42 Event (infection) rates vary considerably, likely driven by the presence of outbreaks, with high rates of 38% for those not taking PPIs and 52% for those taking PPIs41 to as little as 1.7% for those not taking PPIs and 3.3% for those who were taking them.42
Limitations: All data are observational and at high risk of confounding bias.
Is cannabis use associated with an increased risk of schizophrenia?
Bottom line: Cannabis use is associated with an increased risk of schizophrenia. Over approximately 30 years, people who never used cannabis had a 0.7% chance of developing schizophrenia versus 4.2% for regular users.
Self Learning content: A review article of 12 cohort studies followed 591 to 50 053 patients for 1 to 35 years.43 All found positive ORs for schizophrenia, 9 out of 12 of which were statistically significant. The largest study (1.7 million patient-years)44 found an adjusted OR of 1.8. The absolute unadjusted schizophrenia risks were 0.7% for those who had never used cannabis, 1.5% for those having ever used cannabis, and 4.2% for those who had used cannabis more than 50 times.
Context: Another systematic review of cohorts found an adjusted OR of 1.41 (95% CI 1.20–1.65) for any use and 2.09 (95% CI 1.54–2.84) for regular use.45 A second systematic review and meta-analysis found similar elevated risk (unadjusted OR = 3.90, 95% CI 2.84–5.34) for higher users.46 In patients with past psychosis, continued cannabis use predicts higher relapse rates and longer hospital admissions.47
Limitations: Studies are observational and confounding likely affects results.48
Last thoughts
One concern about the Self Learning Program is that each question and answer is based on a single article. Our review of the top 10 articles included careful evaluation of related studies, including the highest-level evidence available. For 2 of the 10 questions, the answer needed minor qualification (melatonin for headaches and BP measurement over clothes); however, for 8 of 10 questions the message was fully supported by related literature.
Acknowledgments
This article was reviewed by Ms Laura Cox, Assistant Manager of the Self Learning Program, and 3 family physicians on the Self Learning Committee: Drs Michael Rondilla, Nicholas Vanderkamp, and Morris Rotbard.
Notes
Editor’s key points
▸ This article summarizes the 10 articles highlighted in the College of Family Physicians of Canada’s Self Learning Program in 2017 that participants rated as most likely to affect practice.
▸ Topics include blood pressure (BP) measurement over clothing, melatonin versus amitriptyline for migraine prevention, complementary health products for treating and preventing the common cold, bismuth quadruple therapy versus triple therapy for Helicobacter pylori, urine culture results in uncomplicated urinary tract infection, deprescribing of proton pump inhibitors and the effects of their long-term use, lower BP targets in elderly patients, the usefulness of the Mini-Mental State Examination for predicting driving risk in patients with dementia, and the association of cannabis use with increased risk of schizophrenia.
▸ Each question in the Self Learning Program is based on a single article. The authors also performed a careful review of the related literature for each question. For 2 of the Self Learning questions (melatonin for headaches and BP measurement over clothing), the answer needed only minor qualification after this review; in 8 of 10 questions the message was fully supported by the related literature.
Points de repère du rédacteur
▸ Cet article résume les 10 articles du programme Autoapprentissage du Collège des médecins de famille du Canada que les participants en 2017 ont cotés comme étant les plus susceptibles d’influer sur la pratique.
▸ Parmi les sujets couverts figuraient la mesure de la pression artérielle (PA) par-dessus les vêtements, l’utilisation de la mélatonine au lieu de l’amitriptyline pour prévenir la migraine, les produits de santé complémentaires pour le traitement et la prévention du rhume, la thérapie quadruple au bismuth plutôt qu’une triple thérapie pour l’Helicobacter pylori, les résultats de la culture d’urine dans les infections des voies urinaires sans complication, la déprescription des inhibiteurs de la pompe à protons et les effets de leur usage à long terme, les cibles plus basses de la PA chez les personnes plus âgées, l’utilité du mini-examen de l’état mental pour prédire les risques de la conduite automobile chez les patients atteints de démence, et l’association établie entre la consommation de cannabis et les risques accrus de schizophrénie.
▸ Dans le programme Autoapprentissage, chaque question se fonde sur un seul article. Les auteurs ont aussi effectué un examen rigoureux de la documentation scientifique sous-jacente pour chaque question. Pour 2 des questions d’Autoapprentissage (la mélatonine pour les céphalées et la mesure de la PA par-dessus les vêtements), la réponse ne nécessitait que des réserves mineures après cet examen; dans 8 questions sur 10, le message était entièrement étayé par la littérature scientifique correspondante.
Footnotes
Contributors
All authors contributed to the review of participant evaluations, the literature review and analysis, and preparing the manuscript for submission.
Competing interests
All the authors are employees of the College of Family Physicians of Canada, which develops the Self Learning Program. The authors have no other relevant conflicts of interest.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.