


Abstract
Objective To define pregnancy-related cardiovascular risk indicators and their association with developing future cardiovascular disease (CVD), and to provide guidance on how primary care providers can help lower future CVD risk through early identification and intervention.
Sources of information Primary research sources, systematic reviews and meta-analyses, and clinical review articles.
Main message Cardiovascular disease is the leading cause of death in women. As underlying CVD risk factors are often present for years before the onset of CVD, it is important to use innovative ways to identify women who should undergo CVD risk screening at a younger age. Pregnancy and the postpartum period afford that opportunity, given that the development of certain pregnancy complications (hypertensive disorders of pregnancy, gestational diabetes mellitus, idiopathic preterm birth, delivery of a baby with intrauterine growth restriction, or placental abruption) can reliably identify women with underlying, often unrecognized, CVD risk factors.
Conclusion Women with 1 or more of these pregnancy complications should be identified at the time of delivery and have formalized postpartum follow-up, including a thorough history, a physical examination, biochemical screening, counseling around lifestyle modification, and possible therapeutic intervention. The link between pregnancy complications and future CVD affords the earliest opportunity for CVD risk assessment for health preservation and disease prevention.
Family physicians endeavour to identify, screen, and counsel patients to prevent future disease. Cardiovascular disease (CVD) is the leading cause of death in women,1 and it is now well established that women who have had certain adverse obstetric outcomes—preeclampsia, gestational hypertension, gestational diabetes mellitus (GDM), idiopathic preterm birth, delivery of a baby with intrauterine growth restriction (IUGR) or low birth weight (< 2500 g at term), or a placental abruption leading to delivery— are at increased risk of developing CVD.2,3 A survey of obstetric care providers in Ontario showed that most were largely unaware of the association between certain pregnancy complications and a woman’s future risk of CVD, and most do not implement any type of follow-up cardiovascular risk screening.4
Pregnancy can be viewed as a cardiovascular stress test in that the development of certain complications has the potential to reveal a woman’s susceptibility to future vascular or metabolic disease.5,6 The term pregnancy-related cardiovascular risk indicator7 has been used to describe pregnancy complications that identify a woman with a greater chance of having underlying cardiovascular risk factors. For example, women who experience a hypertensive disorder of pregnancy (preeclampsia or gestational hypertension) are 4 times more likely to have or develop hypertension after pregnancy and have double the risk of developing CVD.2,4–6 In fact, the American Heart Association guidelines and the Canadian Cardiovascular Society guidelines for the management of dyslipidemia now include hypertensive disorders of pregnancy as an independent risk factor in the evaluation of CVD risk.8,9 Placental abruption is also associated with double the risk of future CVD, and those with GDM have more than 7 times the risk of developing type 2 diabetes.6,10 For preeclampsia, which is the most studied of these outcomes, there is an increased risk of overall CVD (relative risk [RR] = 2.15; 95% CI 1.76 to 2.61), hypertension (RR = 4.46; 95% CI 3.14 to 6.33), ischemic heart disease (RR = 2.06; 95% CI 1.68 to 2.52), stroke (RR = 1.53; 95% CI 1.21 to 1.92), diabetes (RR = 2.27; 95% CI 1.55 to 3.32), and premature cardiovascular death (RR = 1.49; 95% CI 1.05 to 2.14) compared with women with uncomplicated pregnancies.11–15 For women who deliver a baby with IUGR prematurely in conjunction with severe preeclampsia, the risks are significantly greater, especially for premature CVD (RR = 8.12; 95% CI 4.31 to 15.33).12,13,16,17 Given that approximately 20% of women will have 1 or more of the above-mentioned pregnancy complications,7 intervention could result in substantial downstream benefits for a large number of women.
Numerous retrospective database and prospective cohort studies comparing women who had 1 or more of these adverse obstetric outcomes with healthy-pregnancy controls have demonstrated differences in cardiovascular risk factors including increased blood pressure (BP), increased lipid levels, increased body mass index (BMI), insulin resistance, residual microalbuminuria, and criteria for the metabolic syndrome at various times in the postpartum period.13,14,18,19 Excess weight gain in pregnancy or postpartum weight retention or weight gain also put women at increased risk of future disease.20–22 In long-term follow-up studies, gestational weight gain is statistically significantly associated with weight change from early pregnancy to 1 year,21,23 10 years,24 and 15 years postpartum.25–28
Pregnancy offers a unique window to a woman’s future health, and the link between pregnancy complications and future CVD affords us with perhaps the earliest opportunity for CVD risk assessment for health preservation and disease prevention.29 Family physicians, who deal with preventive medicine and motivational interviewing on a daily basis, are well positioned to identify and counsel women who are at increased risk. It is our aim to reduce future CVD in women by
increasing primary care providers’ and patients’ awareness of pregnancy-related CVD risk indicators, and
giving primary care providers a resource to guide them on how to identify and manage these patients postpartum.
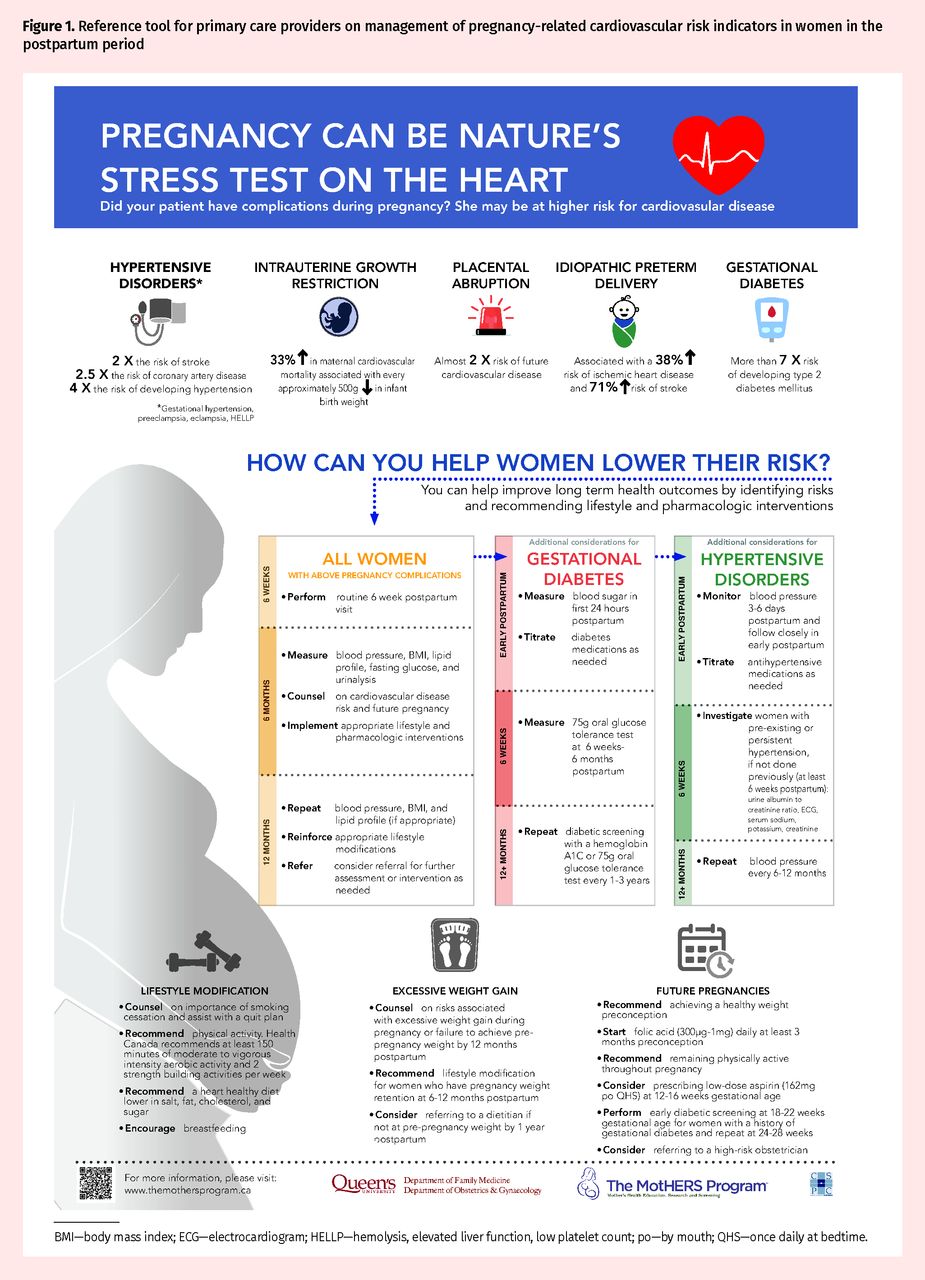
Poster tools were developed to promote knowledge translation of this subject for both patients and primary care providers. In addition, the primary care provider poster can be used as a quick reference tool for management of these women in the postpartum period (Figures 1 and 2).* When considering different platforms for knowledge distribution, we chose a poster tool because it is capable of reaching a wide audience. In addition, posters are simple, cost effective, and capable of being interactive with the use of QR (quick response) codes. When displayed in the office they can also serve as a visual reminder to physicians to address this issue.

Reference tool for primary care providers on management of pregnancy-related cardiovascular risk indicators in women in the postpartum period
BMI—body mass index; ECG—electrocardiogram; HELLP—hemolysis, elevated liver function, low platelet count; po—by mouth; QHS—once daily at bedtime.
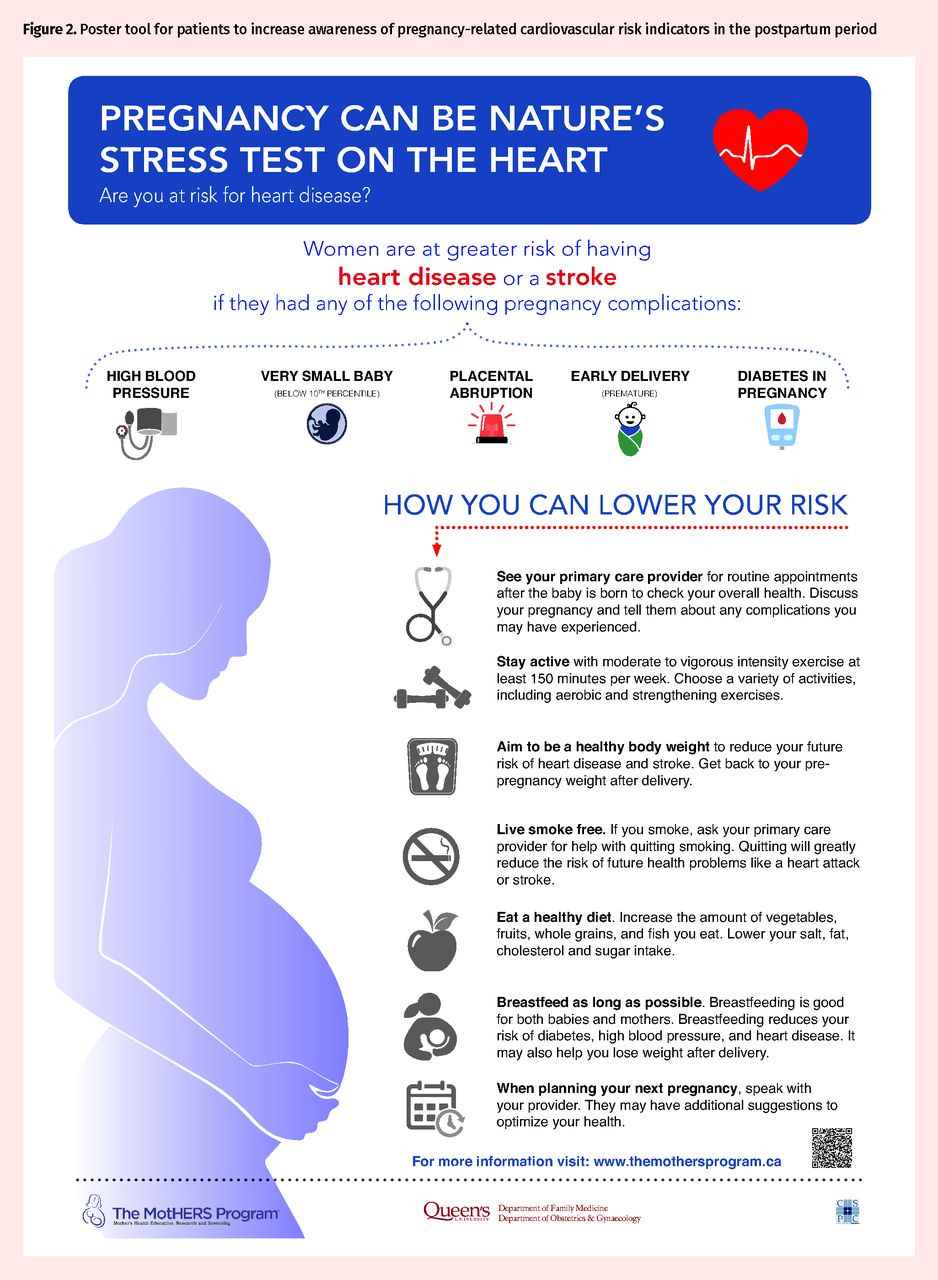
Poster tool for patients to increase awareness of pregnancy-related cardiovascular risk indicators in the postpartum period
Case description
S.C. is a 25-year-old previously healthy woman (1 pregnancy, 1 birth) who lives with her husband in an apartment and works as a cashier at a local store. She does not smoke, drink alcohol, or use drugs. During her first pregnancy, she developed preeclampsia at 36 weeks’ gestation for which she received antihypertensive medication. Because of worsening hypertension and biochemistry results, labour was induced and she delivered a healthy 3-kg baby at 39 weeks’ gestation. Her BP was mildly elevated (145/95 mm Hg) in the immediate postpartum period, requiring treatment with labetalol. She was discharged home on day 2 while taking labetalol, which was stopped 2 weeks postpartum because of normalization of her BP.
Sources of information
We consulted primary research sources, systematic reviews and meta-analyses, and clinical review articles to create the poster tools.
Main message
Postpartum recommendations for women with pregnancy-related cardiovascular risk indicators include lifestyle modifications such as improving diet, increasing physical activity, and breastfeeding; recommendations for the management of specific risk factors such as gestational hypertension or GDM; and recommendations for management of risk factors during future pregnancies.
Lifestyle modification
Diet and activity levels: Even modest modifications of various lifestyle parameters have been shown to reduce risk factors for CVD. In particular, regular (at least 150 minutes per week) physical activity of moderate to vigorous intensity might ameliorate the adverse systemic effects of obesity.30 A 5% to 10% weight loss when accompanied by physical activity is shown to beneficially affect lipid and cholesterol levels and various hemostatic and inflammatory factors.23,24 Ideally, a discussion with a registered dietitian about dietary changes to align with the national guidelines should occur. An example would be to discuss the DASH (Dietary Approach to Stop Hypertension) diet.25 Strategies to increase physical activity levels to align with national guidelines (such as the Canadian Society for Exercise Physiology or the Heart and Stroke Foundation of Canada) should also be discussed.30,31 Physical activity programs involving this group of women postpartum in a research setting have been shown to improve cardiovascular risk indicators.26,27 However, lifestyle programs that are affordable and adaptable to each woman’s individual needs must be developed.28
Breastfeeding: The maternal benefits of breastfeeding have been well documented. In an analysis of women in the CARDIA (Coronary Artery Risk Development in Young Adults) cohort, the protective association between breastfeeding and metabolic disease appeared to persist after weaning. Longer lifetime benefits of lactation include a lower incidence of type 2 diabetes and hypertension.32,33 In an analysis of participants in the Nurses’ Health Study, the benefits of breastfeeding appeared to also extend to CVD. Women who breastfed for a cumulative 2 years (following all pregnancies) were 37% less likely to have coronary artery disease than parous women who did not breastfeed were.34 Taken together, it would appear that breastfeeding would be beneficial for women who are at risk of future CVD, and counseling and support for these women immediately following delivery with a pregnancy complication should include this information.35
Management of specific risk factors
All women with pregnancy-related cardiovascular risk indicators: In addition to the routine 6-week postpartum visit, we recommend additional postpartum followup visits with a focus on identifying and reducing future CVD risk.29 At 6 months postpartum, we suggest measuring BP, measuring BMI, obtaining a lipid profile, and testing urine to determine the albumin-to-creatinine ratio. It is also important to counsel women on their increased CVD risk, discuss how to optimize their health during future pregnancies, and recommend lifestyle and pharmacologic interventions where appropriate. At 12 months postpartum, we suggest repeating measurements of BP, BMI, and lipid levels (if abnormal at 6 months), reinforcing appropriate lifestyle modifications (increasing physical activity, eating a healthy diet, etc), and considering referral (eg, to a cardiologist, a registered dietitian, or a maternal-fetal medicine specialist) for further assessment or intervention if necessary.
Data suggest that general awareness of CVD risk among women is associated with initiation of preventive actions,36 thereby highlighting the need for targeted cardiovascular risk indicator and CVD educational interventions. A study of the effectiveness of postpartum lifestyle interventions (educational, nutritional, and physical activity programs) in high-risk populations has demonstrated the value of risk reduction in this population of women.37 Furthermore, analysis of survey data identified women with preeclampsia to be highly motivated to lower their risk of CVD, although focus group participants identified the need for professional counseling.28 Despite potential barriers, a recent evidence-based review of postpartum cardiovascular risk indicator management has called for the development of structured postpartum cardiovascular risk screening programs after complicated pregnancies.38,39 Such programs have been initiated at the Maternal Health Clinic in Kingston, Ont.7,40,41
Gestational diabetes mellitus: Women with GDM require close follow-up and titration of their diabetes medications as needed in the early postpartum period. Diabetes Canada guidelines for women who had a pregnancy complicated by GDM recommend a 75-g oral glucose tolerance test (OGTT) between 6 weeks and 6 months postpartum.42,43 Given that women with GDM are at a statistically significantly higher risk of developing type 2 diabetes, diabetes screening with a 75-g OGTT or hemoglobin A1c level should be repeated every 1 to 3 years.44 Although determining the hemoglobin A1c level takes less time and is likely preferred by patients, the OGTT is more sensitive in this high-risk population if the hemoglobin A1c level is between 5.5% and 6.4%.44
Hypertensive disorders: Women with hypertensive disorders of pregnancy, including gestational hypertension, preeclampsia, eclampsia, and HELLP (hemolysis, elevated liver enzyme levels, and low platelet count) syndrome should have close follow-up with their primary care providers immediately postpartum (BP assessment 3 to 6 days after delivery) and BP monitoring every 1 to 2 weeks thereafter in the early postpartum period.45 Those who are taking antihypertensive medications in pregnancy might require titration of their medications as indicated early in the postpartum period. Family physicians should consider continuing antihypertensive therapy postpartum, particularly in women with antenatal preeclampsia and those who delivered preterm, as suggested in the Society of Obstetricians and Gynaecologists of Canada guidelines for hypertensive disorders of pregnancy, with a target BP of less than 140/90 mm Hg (< 130/80 mm Hg in those with pregestational diabetes).45 Antihypertensive agents generally acceptable for use while breastfeeding include labetalol, extended-release nifedipine, methyldopa, captopril, and enalapril.45
If BP is persistently elevated at 6 weeks postpartum, consider further workup with a urinalysis; measurement of serum sodium and potassium, creatinine, and fasting glucose levels; and an electrocardiogram (if not done previously).45 After the postpartum period, screening for hypertension should occur at least every 6 to 12 months, as these patients are at a statistically significantly higher risk of developing essential hypertension later in life. The 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult9 recommend that any woman who has had a hypertensive disorder of pregnancy should have postpartum cardiovascular risk screening, including a lipid profile at 6 months postpartum. Postpartum hypertension that is difficult to control and women who have ongoing proteinuria (increased albumin-to-creatinine ratio at 6 months) might benefit from a referral to a nephrologist.45
The Society of Obstetricians and Gynaecologists of Canada guidelines recommend lifestyle modifications (smoking cessation, DASH-like diet, regular physical activity, and weight management) as first-line therapy for those with hypertensive disorders of pregnancy postpartum, with a target low-density lipoprotein (LDL) level of less than 2.6 mmol/L.45 These women should be classified as high risk (ie, statins are indicated), with a target LDL level of less than 3.5 mmol/L, which aligns with the Canadian lipid guidelines.9
Future pregnancies.
Postpartum follow-up also provides the opportunity for counseling, planning, and intervention to improve future pregnancy outcomes. In addition to routine preconception advice, such as preconception folic acid usage, there are a number of other pregnancy complication–specific topics that should be addressed. For example, it is clear that not returning to prepregnancy weight increases the risk of future pregnancy complications.46 Health Canada recommends a multidisciplinary approach for women who have not lost their pregnancy weight (or who have actually gained weight) at 12 months postpartum. This would include involving a registered dietitian, peer support, or improved access to opportunities for physical activity, such as programs that provide child care at no or low cost.20 Given the benefits of breastfeeding to the baby and the metabolic benefits of breastfeeding to the mother,47 it might also be worth starting the discussion and identifying community supports to increase breastfeeding success early in pregnancy.
For those with a history of hypertensive disorders of pregnancy, IUGR, or preterm birth, consideration might be given to the use of low-dose acetylsalicylic acid (ASA) (162 mg orally once daily at bedtime) starting at 12 to 16 weeks’ gestation in a subsequent pregnancy.45,48,49 Acetylsalicylic acid has been shown to reduce the risk of preeclampsia, IUGR, and preterm birth by 10% to 25% in subsequent pregnancies.50,51 For those who have previously had GDM, early screening in the next pregnancy with a 75-g OGTT is recommended to start at 18 to 22 weeks’ gestation, with a repeat screen at 24 to 28 weeks if results are negative.52 For a patient with a history of idiopathic preterm labour, in addition to the ASA recommendation for subsequent pregnancies, the patient might be a candidate for vaginal progesterone (200 mg vaginally once daily at bedtime) starting at 18 to 22 weeks’ gestation to reduce their future risk of preterm labour.53,54 As pregnant women are often not seen by an obstetric provider until later in their pregnancy, these recommendations are particularly important for primary care providers.
Case resolution
S.C. was seen for follow-up at 6 months postpartum. On history she identified that she has a first-degree relative (her mother) who was diagnosed and treated for hypertension in her 50s. S.C. does not breastfeed and is not physically active. The average of 5 BP readings was 135/84 mm Hg, her BMI was 30.6 kg/m2, and she remained 4.4 kg heavier than her prepregnancy weight. Her waist circumference was 101.8 cm. Bloodwork demonstrated substantially elevated LDL cholesterol (4.49 mmol/L), total cholesterol (6.49 mmol/L), triglyceride (2.24 mmol/L), and fasting glucose (5.7 mmol/L) levels, with a reduced high-density lipoprotein cholesterol level (0.98 mmol/L). Her urine albumin-to-creatinine ratio was normal. She met all criteria (elevated BP, abdominal obesity, elevated triglyceride levels, decreased high-density lipoprotein level, elevated fasting glucose level) for the diagnosis of metabolic syndrome. She was counseled in terms of lifestyle modification and physical activity. She returned 6 months later (now 12 months postpartum) for further follow-up. With increased physical activity and dietary monitoring, she had managed to attain her prepregnancy weight and BMI (28.8 kg/m2). Her BP was 125/80 mm Hg and a repeat lipid profile showed an LDL level of 4.2 mmol/L. Upon review on the Canadian lipid guidelines,9 you had a conversation with her about the potential risks and benefits of statin therapy to reduce her cardiovascular risk. She chose to lower her risk with a moderate-intensity statin (20 mg of oral, once-daily atorvastatin) and you recommended stopping it at the time of her next pregnancy. You recommended she have her BP checked every 6 to 12 months, and during her next pregnancy, she should take low-dose ASA (162 mg orally once daily at bedtime) starting between 12 and 16 weeks’ gestation.
Conclusion
Future research should evaluate the effectiveness of the poster tools in accomplishing the aims of this work. Research is required to determine the long-term effectiveness of initiating pharmacotherapy such as statins in this population. Development of risk calculators that specifically include these women is also necessary.
For most women of reproductive age, pregnancy and the postpartum period provide an early window of opportunity to identify underlying, often undiagnosed cardiovascular risk indicators that increase the risk of future CVD. Preventive medicine is a cornerstone of primary care. Primary care providers have a unique opportunity to make a difference in this patient population through earlier identification and management of these well-documented risk factors for CVD to preserve and improve long-term health. Through knowledge distribution and management recommendations for this patient population in the postpartum period and beyond, it is our hope that primary care providers can better address pregnancy-related cardiovascular risk indicators and prevent future disease.
Acknowledgments
We thank Nathan Merrithew for his graphic design contribution.
Notes
Editor’s key points
▸ For most women of reproductive age, pregnancy and the postpartum period provide an early window of opportunity to identify underlying, often undiagnosed, cardiovascular risk indicators that increase the risk of future cardiovascular disease.
▸ Postpartum recommendations for women with pregnancy-related cardiovascular risk indicators include lifestyle modifications such as diet counseling, increasing physical activity, and breastfeeding.
▸ For those with specific risk factors such as gestational hypertension or gestational diabetes mellitus, postpartum follow-up visits with a focus on identifying and reducing future cardiovascular disease risk are recommended in addition to the routine 6-week postpartum visit.
▸ Recommendations for management during future pregnancies include weight counseling and low-dose acetylsalicylic acid for prevention if indicated.
Footnotes
↵* The poster tools on pregnancy-related cardiovascular disease risk indicators for physicians (Figure 1) and patients (Figure 2) are available at www.cfp.ca. Go to the full text of the article online and click on the CFPlus tab.
Contributors
All authors have made substantial contributions to the design and interpretation of the work. Dr Graves drafted the work and all authors revised it critically for important intellectual content. All authors have approved the final version to be published and agreed to be accountable for all aspects of the work by ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests
None declared
This article is eligible for Mainpro+ certified Self-Learning credits. To earn credits, go to www.cfp.ca and click on the Mainpro+ link.
This article has been peer reviewed.
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro de décembre 2019 à la page e505.
- Copyright© the College of Family Physicians of Canada





{kind=link}
{kind=link}