


Abstract
Objective To assess the quality of point-of-care ultrasound (POCUS) training in family medicine residency programs and to obtain the opinions of current family medicine residents on the role of ultrasound in primary care.
Design A 23-question online survey conducted using SurveyMonkey between March 15 and June 30, 2017.
Setting Canada.
Participants All family medicine residents of the 17 Canadian family medicine residency programs were included in the study but all enhanced skills residents were excluded.
Main outcome measures The quality and relevance of POCUS to primary care as perceived by residents and reported in the survey.
Results A total of 854 Canadian family medicine residents responded, for a national response rate of 32.3%. Most respondents (94.3%) believe that POCUS training should be included in family medicine residency programs; however, only 18.4% of respondents currently receive formal training within their residency. Among those without POCUS training, 91.7% are interested in receiving formal training and 29.7% resorted to taking external POCUS courses. Most (77.5%) would consider using ultrasound in their future practice if they were competent in POCUS. The most useful applications for family medicine were considered to be the FAST (Focused Assessment with Sonography in Trauma) examination for free fluid and ascites (95.1%), procedural guidance (92.4%), and identifying an intrauterine pregnancy (88.6%).
Conclusion This is the largest survey identifying the perceived needs of family medicine residents for POCUS. Very few Canadian family medicine residents currently receive POCUS training. Consistent with our recent family medicine program director survey, there is overwhelming interest by family medicine residents to begin incorporating POCUS training into the family medicine curriculum.
Point-of-care ultrasound (POCUS) has become an essential clinical tool in numerous medical specialties including emergency medicine, anesthesia, and critical care.1–4 Improved diagnostic accuracy, increased patient satisfaction, and decreased complications from invasive procedures have all been associated with its use.5–12
In family medicine clinics, ultrasound has been used for a multitude of clinical applications such as assessment for abdominal aortic aneurysms (AAAs), confirmation of intrauterine pregnancy, guidance for joint injections, and many more.13–16 Evidence supports that POCUS use by family physicians can lead to a reduced number of hospital scans, emergency department admissions, and hospital visits.17
In the United States, a 2015 survey by Hall et al demonstrated that a small but rapidly increasing number of family medicine residency programs were incorporating POCUS training.18 In 2016, the American Academy of Family Physicians published recommended curriculum guidelines for family medicine residents for POCUS, including specific criteria for family medicine residents to achieve competency in its use.19 Following this, in 2017 the University of South Carolina in Columbia published a paper describing their development of a family medicine POCUS curriculum.20
In Canada, a 2016 survey of family medicine residency program directors and academic leads revealed that there is no broadly accepted POCUS curriculum to train family medicine residents and numerous barriers to its implementation exist. However, almost all program directors (93%) believed that POCUS should be integrated into family medicine residency curricula, and 71% believed that POCUS could be used in family medicine clinics to alter clinical decision making.21
Family medicine residents are an important source of information for curriculum development and understanding the perceived needs of the learner.22–24 We aim to assess the quality of POCUS training in family medicine residency programs across Canada and obtain the opinion of current family medicine residents on the role of ultrasound in primary care.
METHODS
A bilingual (English and French) online survey of Canadian family medicine residents was administered between March and June 2017. The survey was developed by a group of 8 POCUS experts, including ultrasound academic leads with extensive teaching experience and publications related to POCUS, as well as input from family medicine residents and a medical student. Our group included physicians from McGill University in Montreal, Que; the University of Ottawa in Ontario; the University of Manitoba in Winnipeg; Memorial University of Newfoundland in St John’s; the University of Toronto in Ontario; and Western University in London, Ont. This survey was designed to ask similar questions to our survey of family medicine program directors to allow for direct comparison.21 Both of these surveys also had strong influence from previous surveys conducted by Steinmetz et al and Hall et al, which were each independently validated, and so we did not repeat external validation and pilot testing of this survey.18,25 The questions were reviewed internally by our group of POCUS experts and altered multiple times to maximize their clarity and avoid any biased language. The survey and study design were approved by the provincial Health Research Ethics Board of Memorial University. The final survey consisted of 3 sections: current training status, perceived relevance of POCUS to primary care, and demographic characteristics. There are 23 items in the survey, including multiple-choice questions with single or multiple answers, rating-scale questions, and Likert-type scales.
All family medicine residents of the 17 Canadian family medicine residency programs were included in the study. Enhanced skills residents were excluded from the study, as many of these programs, such as emergency medicine, already have an integrated POCUS curriculum.
The target population was estimated to be 2645 first- and second-year family medicine residents nationwide based on Canadian Resident Matching Service data and verified by respective site administrators. Survey participants were entered into a random draw for gift cards of $50.
The first survey invitation was sent out via e-mail on March 15, 2017, with reminder e-mails sent 1 and 2 months after the original invitation. The survey was closed on June 30, 2017, at midnight to avoid changes in our survey population associated with the new cohort of residents who started on July 1. The invitation contained a short cover letter, an abstract describing the objectives of the study, and a link to the online consent form and survey. The survey link was sent to the study population through individual e-mail using a private e-mailing list sent by respective resident site coordinators and program administrators; individual e-mail using a private e-mailing list sent by respective resident representatives of the College of Family Physicians of Canada Section of Residents; a survey link included in the e-newsletter of the residency program; a survey link posted on Facebook groups of the residency program; and a private e-mailing list of the Society of Rural Physicians of Canada. To ensure multiple surveys were not completed by the same respondent, only 1 survey submission was accepted from a single IP (Internet protocol) address.
The survey was distributed by SurveyMonkey. Raw data were exported from SurveyMonkey into a Microsoft Excel spreadsheet. A single data abstractor analyzed the survey responses and reported them as percentages in tabular format. Responses were kept anonymous and all data were reported in aggregate.
RESULTS
After removing responses from enhanced skills residents, 854 responses out of a total 2645 first- and second-year Canadian family medicine residents were obtained, for an overall national response rate of 32.3%.
Demographic characteristics
Surveyed population demographic characteristics are summarized in Table 1. We received 672 (78.7%) English responses and 182 (21.3%) French responses. Respondents identified their residency sites as rural (29.6%), urban or community (38.2%), or academic teaching (32.2%). Most residents (91.5%) identified general family practice as their anticipated practice focus, followed by emergency medicine (48.6%), hospitalist medicine (39.0%), and maternal, newborn, and obstetric care (27.2%).
Demographic characteristics of family medicine resident respondents: N = 854 but denominators vary owing to missing data.
Current training status
Most residents (94.3%) believe that POCUS training should be included in family medicine residency programs; however, only 18.4% currently receive formal training. Table 2 summarizes the most commonly reported training experiences among those who have received formal training. Of those who did not receive formal POCUS training, most (91.7%) reported that they are interested in receiving training as part of their residency. Many respondents (29.7%) have sought formal training through external POCUS courses, although most (72.3%) did not receive funding from their residency programs. Most residents (91.6%) believe that funding should be offered to attend an external POCUS course if the residency program does not offer ultrasound training.
Training experiences with POCUS in family medicine residency programs: N = 151. Only the respondents who indicated that they had received formal training in POCUS as part of their family medicine residency were included in this question.
Perceived relevance of POCUS to primary care
Most respondents (77.6%) believe that POCUS can enhance clinical decision making in family medicine clinics. Perceived benefits are summarized in Table 3. Most (65.0%) believed that POCUS does not negatively affect patient safety. Most residents (77.5%) responded affirmatively to the statement, “If I had POCUS training during my residency, was competent to use it, and had access to an ultrasound machine, I would use POCUS regularly in my practice.” Upon being presented with the statement “I am familiar with the literature on POCUS,” 33.2% either agreed or strongly agreed, 27.7% indicated they were neutral, and the remainder (39.0%) either disagreed or strongly disagreed.
Resident perceptions on the benefits of POCUS to primary care: N = 812.
From a list of 10 POCUS applications, residents were asked if they believed specific applications were useful in family medicine; results are summarized in Figure 1. Those believed to be most useful included the Focused Assessment with Sonography in Trauma (FAST) examination for free fluid and ascites (95.1%), procedural guidance (92.4%), and obstetric ultrasound for confirmation of intrauterine pregnancy (88.6%). Point-of-care ultrasound applications most unfamiliar to current residents are identified as the following: musculoskeletal ultrasound (36.2%), assessment for deep vein thrombosis in lower extremities (29.6%), and renal ultrasound (28.6%).
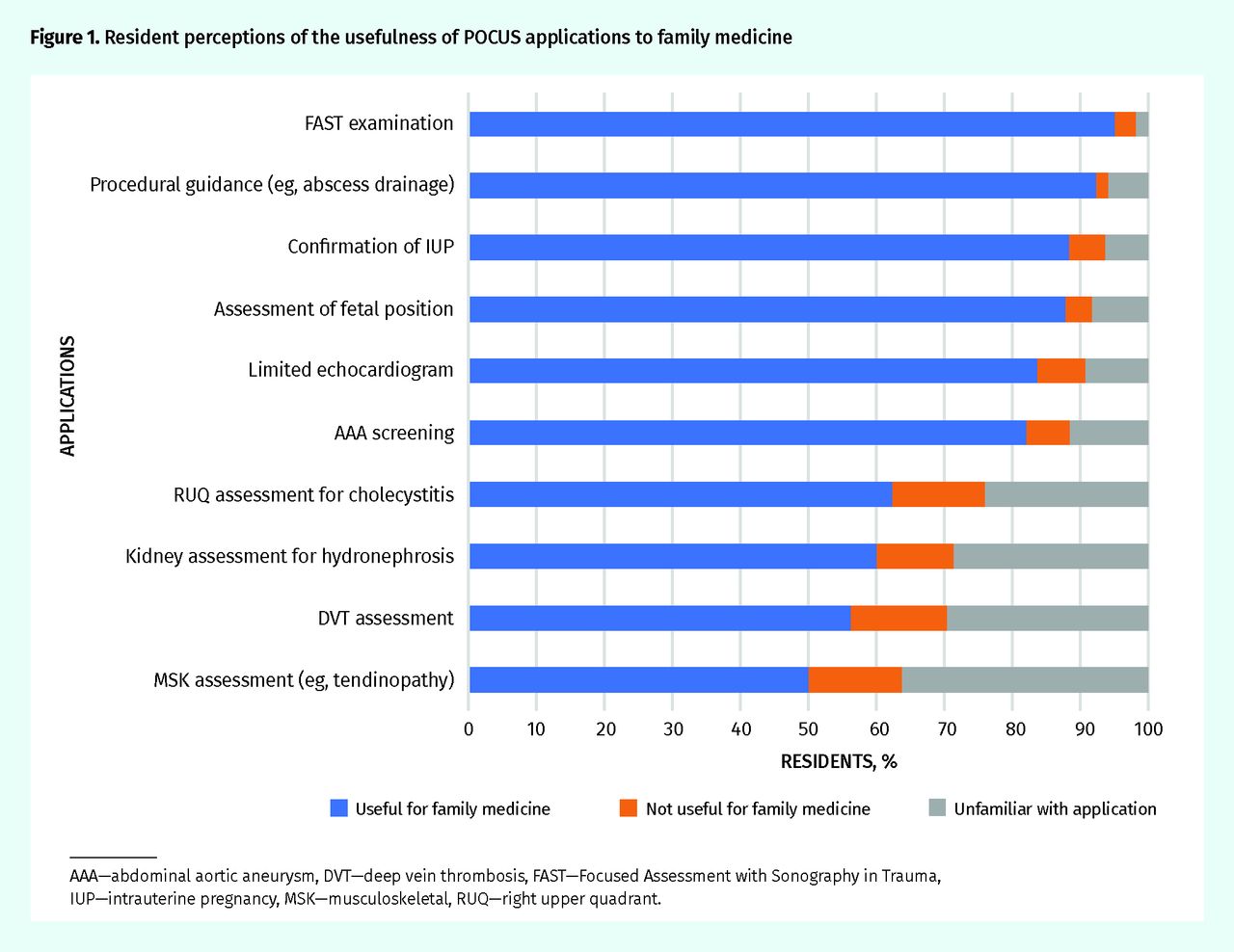
Resident perceptions of the usefulness of POCUS applications to family medicine
AAA—abdominal aortic aneurysm, DVT—deep vein thrombosis, FAST—Focused Assessment with Sonography in Trauma, IUP—intrauterine pregnancy, MSK—musculoskeletal, RUQ—right upper quadrant.
Most residents observed staff physicians using ultrasound in the emergency department (79.3%) or in the context of prenatal, labour, and delivery care (50.8%). A minority of residents had observed staff physicians using ultrasound in family medicine clinics to evaluate patients (17.7%) and perform procedures (36.6%). A small proportion of residents (13.2%) reported that they had never observed a family physician using ultrasound.
DISCUSSION
Our survey results demonstrate that most residents express a strong interest in POCUS training and support the use of POCUS in primary care practice. However, a formal POCUS curriculum has not yet been incorporated into most Canadian family medicine residency programs. This reiterates the results of our recent study of family medicine program directors, who also expressed an interest in establishing a POCUS curriculum. Despite this desire for training, currently only 3 family medicine residency programs in Canada offer an established ultrasound curriculum.21
Implementing POCUS training in family medicine residency programs has several potential barriers, including limited access to ultrasound machines and qualified instructors.21 Aside from a mandatory POCUS curriculum in residency programs, our results suggest a POCUS elective or funding to take external POCUS training are potential solutions. However, this can pose a substantial financial burden to residents, as these electives and courses can cost between $1000 and $5000. Most residents (91.6%) believed funding should come from residency programs to take these courses if formal ultrasound training is unavailable. Increasingly, residency training programs are facing budgetary constraints. Developing in-house training programs or local POCUS electives would help mitigate these costs.
Most residents supported the inclusion of POCUS in primary care practice and identified its main benefits as being a useful adjunct to the physical examination and a rapid diagnostic tool, as well as having the potential to reduce health care spending. Most residents would also consider using POCUS regularly in their clinical practice if both the appropriate training and access to an ultrasound machine were provided. These views are similar to those in the previous study of family medicine program directors, who also expressed favourable views of POCUS in primary care.21 Although most evidence supporting POCUS use comes from emergency medicine, the movement toward the inclusion of ultrasound in family medicine is supported by the growing body of literature highlighting that POCUS use in primary care is accurate, is safe, and has numerous applications for family practice.26–34
In conjunction with the results from our previous survey, both residents and program directors believe ultrasound is useful in clinical practice for AAA screening, obstetric indications, and procedural guidance.21 The use of ultrasound for these applications in primary care is well supported by evidence. Research has demonstrated long-term mortality benefits associated with ultrasound screening of asymptomatic patients for AAA. A recent Canadian prospective study showed that office-based scans for AAA screening had a high degree of correlation with hospital-based scans.13 The use of ultrasound in primary care obstetrics is well documented, and the American Academy of Family Physicians endorsed obstetric ultrasound as a core skill for maternity care.35 A plethora of literature supports the use of ultrasound by clinicians to guide a variety of procedures commonly performed in primary care such as drainage of subcutaneous abscesses, joint aspiration, intra-articular injection, confirmation of intrauterine device placement, and paracentesis.15,36–39
Contrary to the results of the survey of program directors, residents also considered the FAST examination and limited echocardiography as useful applications. Although the FAST examination is well established in the context of abdominal trauma to identify free fluid, it can also be used in the primary care clinic to identify ascites.9 Residents might consider it to be a useful POCUS application owing to their familiarity with its use, as it is often the first application taught as an introduction to bedside ultrasound. Evidence supporting the use of limited echocardiography in primary practice is currently lacking. A study from Norway has demonstrated that after undergoing an 8-hour training program, general practitioners were able to assess left ventricular function using pocket-sized ultrasound with a sensitivity and specificity of 78% and 83%, respectively.29 This skill could be useful for family physicians to help determine the cause of patients presenting with dyspnea including heart failure and pleural effusions.
Many primary care physicians work in a variety of practice settings, including in community emergency departments, in palliative care settings, and as hospitalists. This is also reflected in the residents’ responses (Table 1). The use of POCUS is helpful in the many different practice settings in which family physicians work.
Limitations
A limitation of this study was the overall response rate of only 32.3% of Canadian family medicine residents. Previous research on large population survey studies reported an average response rate of 30% to e-mail surveys and our results are comparable.40,41 Similarly, the 2007 National Physician Survey of Canadian physicians and residents achieved an e-mail response rate of 29.9%.42 In a meta-analysis of Web- and Internet-based surveys, Cook et al suggested that response representativeness is more important than response rate.43 Representativeness refers to how well the sample drawn for the questionnaire reflects the greater population attributes. Overall, responses were fairly evenly distributed across rural, urban or community, and academic teaching units, with 29.6%, 38.2%, and 32.2% response rates, respectively. Another limitation to our survey study is the lack of flexibility in response format. In our study of this large population, multiple-choice responses, binary responses, and Likert scales better quantify the predominant opinions of the surveyed population, but in doing so, we lose certain nuances in the opinions expressed. When possible, we allowed for an “other (please specify)” option for individual responses. However, a qualitative study on the views of family medicine residents and physicians would help to further our understanding of the role of POCUS in primary care.
Finally, it is important to note that most of our resident respondents do not have any formal training in POCUS. Only 33.2% agreed or strongly agreed that they were familiar with the literature on POCUS use. This is higher than family medicine program directors and academic leads, of whom only 21% either agreed or strongly agreed.21 Thus, most family medicine residents and program directors are not entirely familiar with the current literature available on POCUS use, and so opinions on POCUS being used to alter clinical decision making or having no negative effect on patient care might not be evidence based. A future goal will be educating both residents and program directors on the emerging evidence for POCUS use in family medicine.
Conclusion
This is the largest survey identifying the perceived need of family medicine residents for POCUS training. There is overwhelming support for and interest in POCUS by family medicine residents across Canada. Despite this, only 18.4% of residents currently receive formal POCUS training through their residency programs. Consistent with our recent family medicine program directors’ survey on POCUS, most believe training should be incorporated into their residency curricula. Most residents believe that POCUS would positively affect primary care and would consider using ultrasound regularly in their clinical practice if they had the proper training.
Notes
Editor’s key points
▸ In this study, most residents expressed a strong interest in point-of-care ultrasound (POCUS) training and supported the use of POCUS in primary care practice. However, a formal POCUS curriculum has not yet been incorporated into most Canadian family medicine residency programs; only 18.4% of residents currently receive formal POCUS training through their residency programs.
▸ Most residents supported the inclusion of POCUS in primary care practice and identified its main benefits as being a useful adjunct to the physical examination and a rapid diagnostic tool, as well as having the potential to reduce health care spending.
▸ Potential solutions to the lack of training, aside from a mandatory POCUS curriculum, include a POCUS elective or funding to take external POCUS training. Most residents believed funding should come from residency programs if formal ultrasound training is unavailable.
Points de repère du rédacteur
▸ Dans cette étude, la majorité des résidents ont dit souhaiter fortement suivre une formation en échographie au point de service (FEPS), et étaient en faveur de l’utilisation de l’échographie au point de service dans les cliniques de soins primaires. Par ailleurs, un cursus officiel pour la FEPS n’a pas encore été intégré dans la plupart des programmes de résidence en médecine familiale au Canada; seulement 18,4 % des résidents reçoivent actuellement de la formation formelle en échographie au point de service durant leur résidence.
▸ La majorité des résidents étaient favorables à l’inclusion de l’échographie au point de service dans la pratique des soins primaires, et ont indiqué que ses principaux avantages résidaient dans son utilité comme auxiliaire à l’examen physique et dans sa rapidité en tant qu’outil diagnostique, sans compter les possibilités qu’elle offre de réduire les dépenses en santé.
▸ Comme solutions possibles au manque de formation, exception faite d’un cursus obligatoire en échographie au point de service, les résidents ont mentionné un stage optionnel dans ce domaine ou du financement pour suivre une FEPS à l’extérieur. La plupart des résidents croyaient que le financement devrait être assuré par les programmes de résidence si une formation formelle en échographie n’était pas accessible.
Footnotes
Contributors
The survey was mainly developed and the manuscript was mainly written by Drs Peng, Braganza, and Micks. Drs Sue, Woo, Rogers, Freedman, Lewis, Hu, Varner, Patel, Hameed, and Steinmetz were all instrumental in survey design, pilot testing, and distribution. They also provided substantial contributions to manuscript review and editing. Dr Steinmetz was the overall project lead.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada





{kind=link}