


Abstract
Objective To assess how often risk communication and values clarification occur in routine family medicine practice and to explore factors associated with their occurrence.
Design Qualitative and quantitative cross-sectional study.
Setting Five university-affiliated family medicine teaching clinics across Quebec.
Participants Seventy-one health professionals (55% physicians, 35% residents, 10% nurses or dietitians) and 238 patients (76% women; age range 16 to 82 years old).
Main outcome measures The presence or absence of risk communication and values clarification during visits in which decisions were made was determined. Factors associated with the primary outcome (both competencies together) were identified. The OPTION5 (observing patient involvement in decision making) instrument was used to validate the dichotomous outcome.
Results The presence of risk communication and values clarification during visits was associated with OPTION5 scores (area under the curve of 0.80, 95% CI 0.75 to 0.86, P < .001). Both core competencies of shared decision making occurred in 150 of 238 (63%) visits (95% CI 54% to 70%). Such an occurrence was more likely when the visit included discussion about beginning something new, treatment options, or postponing a decision, as well as when health professionals preferred a collaborative decision-making style and when the visit included more decisions or was longer. Alone, risk communication occurred in 203 of 238 (85%) visits (95% CI 82% to 96%) and values clarification in 162 of 238 (68%) visits (95% CI 61% to 75%).
Conclusion Health professionals in family medicine are making an effort to engage patients in shared decision making in routine daily practice, especially when there is time to do so. The greatest potential for improvement might lie in values clarification; that is, discussing what matters to patients and families.
Shared decision making is the collaborative process by which health professionals and patients partner to make evidence-informed health decisions that reflect what matters to patients and their families.1 Such collaboration leads to greater patient knowledge, reduced decision conflict, more active patient involvement, greater patient satisfaction with disease management, more realistic patient expectations, and higher levels of treatment adherence.2–8
Shared decision making requires that both the health professional and the patient bring relevant expertise to health decisions. Professionals bring medical expertise, and patients bring expertise about their own lives and what matters to them and their families. Thus, shared decision making requires communicating evidence regarding potential benefits and harms of all available options (risk communication) and clarifying what matters to patients and families regarding those options (values clarification).1,2,9 Shared decision making might occur less frequently than expected.10,11 It can present challenges in family medicine because multiple health decisions might occur in a single clinical encounter12; decisions are likely to be about chronic conditions, preventive care, and lifestyle issues12,13; and the decision-making process might be complicated by issues such as comorbidity and diverse patient populations.14–16
Because little is known about how often the 2 core competencies of shared decision making occur in primary care, we assessed the frequency with which both occur, and explored contextual factors associated with this occurrence or lack thereof.
METHODS
Study design and context
We conducted a cross-sectional study with both qualitative and quantitative methods. We aimed to collect a convenience sample of 250 visits in primary care, approximately 50 visits per site, considering both the need for a range of primary care consultations and the feasibility of the study. We collected data in 2014 to 2015 at 5 university-affiliated family medicine clinics across Quebec. The study was approved by the research ethics committees of the Integrated University Health and Social Services Centre of the National Capital in Gatineau; Centre de recherche de la CHU de Québec–Université Laval in Quebec city; and the Jewish General Hospital in Montreal.
Participants and recruitment
We first invited all health professionals at participating clinics to enrol in the study, including family physicians, residents, nurses, and allied health professionals who were scheduled to provide care (planned visits or walk-in coverage) during each period of data collection. We then invited patients of the health professionals who agreed to participate and were able to complete a questionnaire in English or French. Our participants included parents or guardians accompanying a minor (defined in Quebec as a person of 14 years of age or younger), as they were the legal decision makers. We refer to such parents and guardians as patients in this article. We excluded unaccompanied minors younger than 14 years of age and patients who had been identified by health professionals as having a condition that affected their ability to provide informed consent.
Data collection
At each clinic, we collected data during 4 to 6 days. Participating adults provided written informed consent and accompanied minors provided written assent. Health professionals completed a single self-administered written questionnaire at recruitment, typically days or weeks ahead of data collection, with closed-ended questions about their sociodemographic characteristics and medical decision-making style preferences.17 Patients completed 2 self-administered written questionnaires. The questionnaire before the visit contained closed-ended sociodemographic questions, as well as original English or translated French versions of validated measures of health literacy18 and subjective numeracy.19,20 The second questionnaire, administered after the visit to avoid biasing patient behaviour during the visit, contained a validated measure of medical decision-making style preferences on a 5-point scale.17 We audio-recorded visits.
Data analysis
Audiorecordings were transcribed verbatim by a professional transcriptionist. Two researchers (G.D., R.R.) independently coded all transcripts in NVivo 10, resolving disagreements by discussion until reaching consensus and reviewing all questions at regular meetings held with 2 other researchers (S.C.D., H.O.W.). We used a combination of inductive and deductive thematic analysis approaches21 to develop a structured coding form.
Coding of visits
We coded 6 aspects of each visit. First, we coded the visit’s purpose (ie, checkup or preventive health care, or another medical reason). Second, we coded how many, if any, decisions were made during the visit. Third, we coded structural characteristics of each decision (ie, was the decision about doing nothing; beginning, stopping, or continuing something; postponing a decision; or taking action later). Fourth, we coded clinical characteristics of decisions (eg, deciding about a screening test or a medical treatment). Fifth and sixth, we coded instances of risk communication and values clarification according to established definitions and taxonomies, using relatively easy-to-attain thresholds. Specifically, we determined risk communication to have occurred during the visit if there was any discussion about potential benefits and harms of health interventions.22–25 We defined values clarification according to a systematic review of values clarification methods,26,27 which specifies that preferences are inclinations toward or away from a medical option and values are the underlying feelings and emotions that help determine preferences. We accordingly defined values broadly as concepts relevant to the decision that matter to patients or families.28,29 Table 1 provides examples for each category. We validated our risk communication and values clarification coding structure by comparing it to OPTION5 (observing patient involvement in decision making) scores; OPTION5 is an established 5-item scale used to measure shared decision making.30,31 We used OPTION5 rather than the original OPTION12 because OPTION5 contains 2 items about values and preferences that were lacking in OPTION12 and because OPTION5 has been shown to be more sensitive.32,33
Coding scheme
Two team members (P.J., S.M.) entered questionnaire data into a spreadsheet. A senior research associate (S.C.D.) verified and corrected any discrepancies in data. We combined these data with codes from the transcripts to create a complete data set about each visit, including aspects of the visit itself and characteristics of the health professional and patient, categorizing variables as needed according to their distribution.34,35
Final coding reflected consensus judgments among 2 (G.D. and R.R. for most codes; R.R. and S.C.D. for OPTION5 scores) or 4 (G.D., R.R., S.C.D., H.O.W.) researchers. We assessed the reliability of coding between each pair of independent analysts with the Cohen κ.36
Statistical analyses
Our main outcome of interest was dichotomous: whether or not risk communication and values clarification both occurred. Our unit of analysis was the visit as a whole, not individual decisions within it, for 3 reasons. First, a single decision in primary care might be discussed during multiple visits,1,37 meaning that analyzing the extent of risk communication and values clarification for a given decision within a single visit might underestimate the extent of these practices. Second, primary care visits are complex and move from one topic to another and then back again,38 meaning that for visits in which multiple topics are addressed, it might be neither possible nor desirable to disentangle values clarification discussions that are relevant to multiple decisions. Third, patient impressions of shared decision making in family medicine visits appear to be formed from the visit as a whole, suggesting that a more global assessment likely better reflects what matters to patients.39,40 We compared our dichotomous outcome to OPTION5 scores by examining the receiver operating curve and assessed the extent to which OPTION5 scores predicted values of our dichotomous outcome.
We identified factors associated with our primary outcome (both competencies together). We also examined the presence or absence of each competency alone within a visit and identified whether health professionals or patients initiated these discussions.
As our data were hierarchical at 3 levels (visit and patient, health professional, and clinic), we examined intraclass correlation coefficients. To account for potential clustering effects among study sites and health professionals, we performed a bivariate analysis and then a multivariable logistic regression analysis using a generalized linear mixed model to estimate the proportion of the presence of both competencies and to identify factors associated with their presence or absence. We conducted statistical analyses in SAS, version 9.4.
RESULTS
Study participants
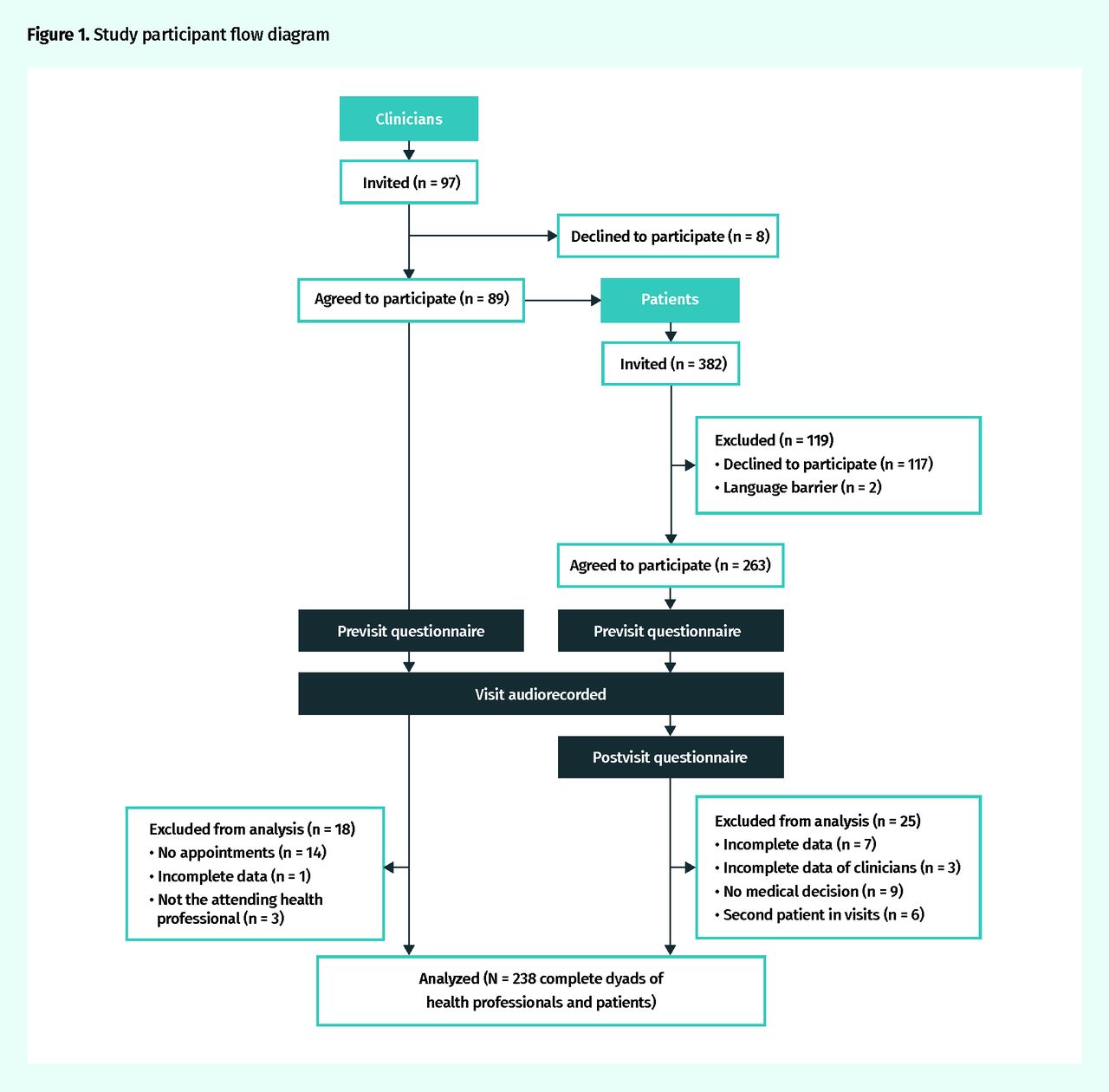
Of the 96 health professionals invited, 89 agreed to participate (93%) and 71 were included in the analysis. We excluded consenting health professionals who had incomplete questionnaire data (n = 1), who were in the room but were not the attending health professional (eg, a resident observing a preceptor) (n = 3), or who had no appointments scheduled during data collection (n = 14). We analyzed 238 complete clinical visits between health professionals and patients. Figure 1 shows study flow and Table 241 details participant characteristics.
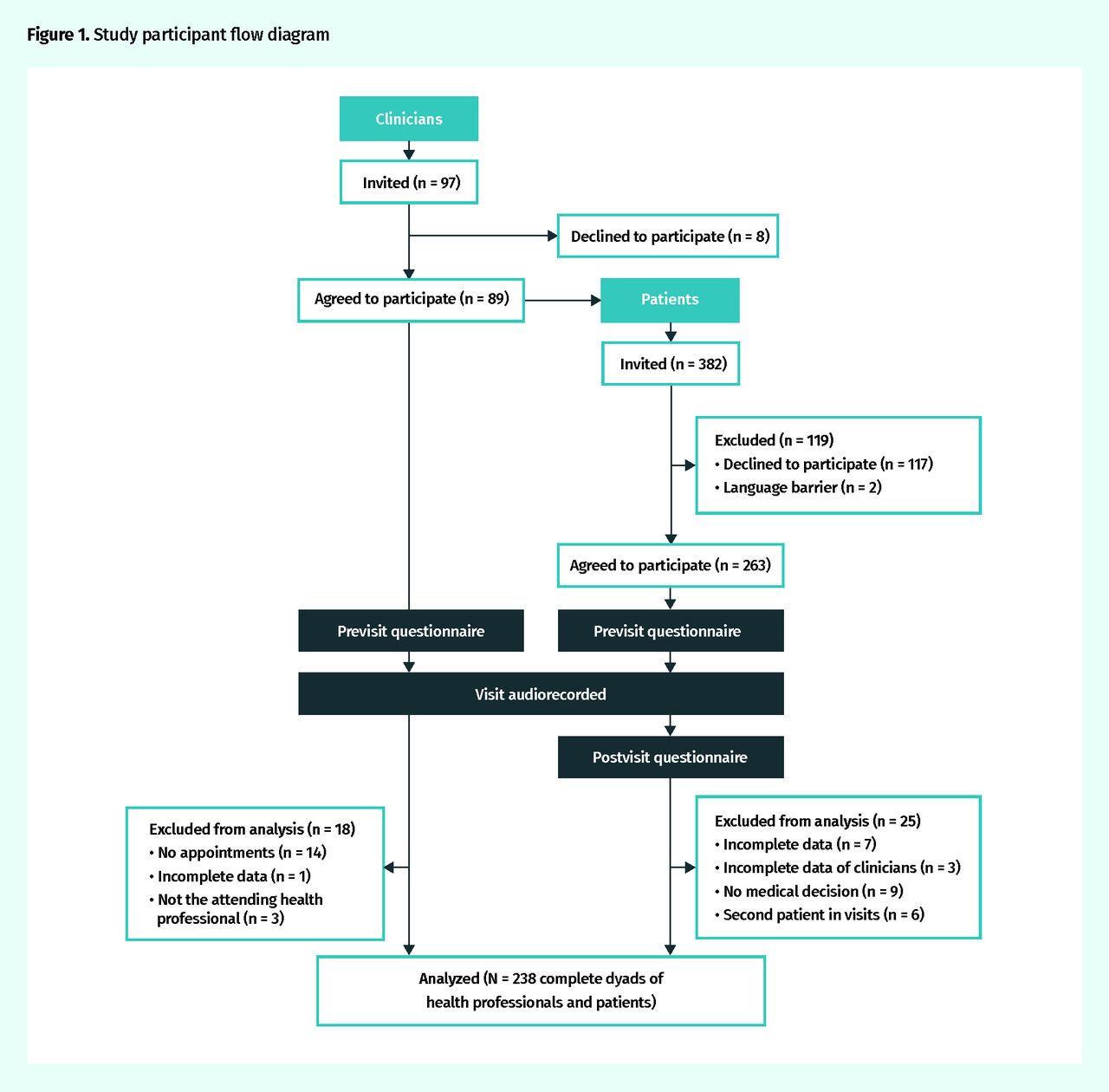
Study participant flow diagram
Participant characteristics: We report the mean and SD if the distribution is normal, and median and IQR if the distribution is not normal.
Characteristics of visits
Reliability of qualitative coding.
Interobserver reliability for primary coding as assessed by the Cohen κ was 0.85. For OPTION5 coding, the Cohen κ ranged from 0.82 to 0.89 across the 5 items. Internal reliability for the OPTION5 measure (Cronbach α) was 0.76.
Risk communication and values clarification.
Risk communication occurred in 203 of 238 (85%) visits. Values clarification occurred in 162 of 238 (68%) visits. Risk communication and values clarification both occurred in 150 of 238 (63%) visits (Table 3), with a 95% CI of 54% to 70%. The presence of both risk communication and values clarification within a visit was related to OPTION5 scores, with an area under the curve of 0.80 (95% CI 0.75 to 0.86, P < .001). Using a cutoff of 5, sensitivity was 0.72 and specificity was 0.76.
Frequencies of risk communication and values clarification in primary care visits: N = 238. We analyzed both objectives with GLMM to account for the potential clustering effect of health professionals, but assumed observations within each clinic to be similar owing to the low ICC at the clinic level.
Health professionals initiated risk communication discussions 96% of the time (194 of 203 visits containing risk communication) and values clarification discussions 60% of the time (98 of 162 of visits containing values clarification).
Factors associated with risk communication and values clarification.
Among the diversity of visits (Table 4), we observed 6 factors associated with the presence of risk communication and values clarification together. The visit was more likely to contain both core competencies of shared decision making when health professionals and patients discussed beginning something new (odds ratio [OR] of 3.54, 95% CI 1.32 to 9.48); discussed a treatment option (OR = 3.56, 95% CI 1.52 to 8.36); discussed more than 5 health decisions (OR = 5.00, 95% CI 1.50 to 16.90); discussed postponing a decision (OR = 4.92, 95% CI 1.35 to 17.87); and when visits were with health professionals who indicated that they preferred a collaborative decision-making style (OR = 8.78, 95% CI 1.62 to 47.71). Longer visits were also more likely to contain both competencies (OR = 1.03, 95% CI 1.00 to 1.07) (Table 5). Sensitivity analyses demonstrated that our results were robust.
Visit characteristics: N = 238. Median (IQR) visit length in minutes was 29.2 (5.2 to 97.3).
Factors associated with risk communication and values clarification (multivariable analysis)
DISCUSSION
Our study aimed to assess how often 2 core competencies of shared decision making occur in routine family medicine practice together or alone and to explore factors associated with their occurrence. We found that risk communication and values clarification occurred together in nearly two-thirds of visits in routine daily family practice but that risk communication occurs more frequently than values clarification. In addition, clinicians had some commonalities regarding their use of both competencies.42 These results led us to make 3 main observations.
First, our findings show that the core elements of shared decision making occurred together in nearly two-thirds of visits without any active intervention. This might be a more positive outcome than in other studies,10 a difference that might be explained by the nature of our clinical sites as teaching clinics,43 the fact that clinicians knew they were being observed, or that our outcome measure was more encompassing than other measures. However, our findings also suggest some room for improvement, particularly in the context of a health decision in primary care, where discussion of risks, benefits, and patients’ values should be a relatively easy threshold to attain.42 Other studies have similarly concluded that shared decision making competencies could be improved in primary care.11,40,43–49
Second, we observed that risk communication was more prevalent than values clarification during primary care visits. This is consistent with previous work in the past 10 to 15 years showing that as evidence-based medicine has moved into practice, it might not always be bringing its intended discussions of values and preferences along to complement the evidence.50 More work is needed to correct the misdiagnosis of patient values and preferences.26,51
Third, we observed that certain factors were associated with the occurrence of both competencies. Visits that included discussions about beginning something new, treatment options, or postponing a decision were more likely to demonstrate both elements. We suggest that other decisions might benefit from an increased focus on discussions of harms, benefits, values, and preferences. For example, given the increased focus on overdiagnosis52 and evidence that patients might overestimate the benefits of screening,53 screening discussions might offer room for meaningful improvement. Visits that were longer were also more likely to contain both competencies, even when controlling for the number of decisions made. These findings align with those of previous studies showing that perceived time constraints are a barrier to shared decision making54 and longer visits are associated with higher scores of communication skills.10,55 When health professionals preferred a less collaborative decision-making style, the core competencies of shared decision making were less likely to occur. Although this finding is not surprising, when combined with our findings of a substantial cluster effect at the level of health professionals and few patients initiating values clarification or risk communication discussions, it emphasizes that a health professional’s individual communication style is a key factor in whether or not a patient will experience shared decision making.
Limitations
Our study has 4 main limitations. First, the generalizability of our study is limited by the fact that we collected data in family medicine teaching clinics, meaning that our results might be less applicable to other primary care settings. Specifically, a relatively high proportion of patients had postsecondary degrees (41% compared with the provincial statistic of 31%56) and, as expected for teaching settings, physicians were younger on average and the median (interquartile range) visit length (29.2 [5.2 to 97.3] minutes) might reflect longer visits compared with previously published mean visit lengths (21 minutes).57 Second, although we used rigorous dual independent analysis to code transcripts and validated our coding strategy with an established, validated measure, our analyses used a newly created outcome measure. Third, we assessed medical decision-making style preferences at different times for patients and physicians. Specifically, for health professionals, we asked for their preferences at recruitment, which was typically days or weeks in advance of the recorded consultations. For patients, we asked immediately after the visit. This was because we believed that the greater threat to data quality for physicians would be missing data owing to difficulty in ensuring they completed a questionnaire after their last participating patient, whereas for patients, we believed that the greater threat to data quality would be that they might change their behaviour owing to answering the question immediately before their visit. It is possible that answering this question reminded physicians about the desirability of shared decision making in advance of recording visits and thus increased the occurrence of both competencies. Finally, this study simply addressed whether risk communication and values clarification occurred, and did not assess the quality of each discussion nor delve deeply into how discussions occurred. Further research will explore these questions to better unpack the intricacies of supporting shared decision making in family medicine.
Conclusion
Health professionals in family medicine teaching clinics demonstrated a minimum level of the 2 core competencies of shared decision making in routine daily practice; progress remains to be made. The greatest area for improvement might have to do with clarifying patients’ values and preferences rather than expecting patients to bring these into the discussion. Providing training in this competency, supportive tools, and time for discussion might facilitate progress.
Acknowledgments
We thank Ms Gisele Bouchard for her work in transcribing visits, Drs Michel Labrecque and Ruth Ndjaboue for their comments on versions of this paper, and Dr Jean-Sébastien Renaud for providing his measurement and evaluation expertise. We gratefully acknowledge the participation of health professionals, patients, and family members at the participating family medicine clinics, and the staff at clinics for accommodating us. The study was funded by Fonds de recherche du Québec – Santé (Réseau-1 Québec), Fonds Gilles-Cormier (Laval University), and the Institut universitaire de première ligne en santé et services sociaux. The funders had no role in the study design, data collection, analysis, and preparation of this manuscript. Dr Légaré is supported by a Tier 1 Canada Research Chair in Shared Decision Making. Dr Witteman is supported by a career development award from the Fonds de recherche du Québec – Santé, Research Scholar Junior 2.
Notes
Editor’s key points
▸ Shared decision making requires 2 key competencies: explaining potential benefits and harms (risk communication) and clarifying what matters to patients and families (values clarification).
▸ Risk communication and values clarification occurred together in nearly two-thirds of visits in routine daily family practice, but risk communication occurred more frequently than values clarification.
▸ Certain factors were associated with the occurrence of both competencies. Visits with health care professionals who preferred a collaborative decision-making style and visits that included discussions about beginning something new, treatment options, or postponing a decision were more likely to demonstrate both elements. Visits that were longer were also more likely to contain both competencies, even when controlling for the number of decisions made. Other decisions might benefit from an increased focus on discussions of harms, benefits, values, and preferences.
Points de repère du rédacteur
▸ Une décision partagée requiert deux compétences principales : l’explication des avantages et des risques éventuels (la communication des risques) et la mise au clair de ce qui est important pour les parents et les familles (la clarification des valeurs).
▸ Dans près des deux tiers des consultations dans les cliniques de santé familiale, la communication des risques et la clarification des valeurs ont été présentées ensemble, mais la communication des risques a été abordée plus souvent que la clarification des valeurs.
▸ On associait certains facteurs à la présence de ces 2 compétences. Les consultations auprès de professionnels de la santé qui préféraient la prise de décision en commun et celles où on discutait de la possibilité d’entreprendre quelque chose de nouveau, des traitements possibles ou du report d’une décision étaient plus susceptibles de comporter les deux éléments. Les discussions plus longues étaient aussi plus susceptibles de comprendre les deux types de compétences, même après un contrôle du nombre de décisions prises. En insistant pour que les discussions portent davantage sur les risques, les avantages, les valeurs et les préférences, on pourrait améliorer d’autres types de décisions.
Footnotes
Contributors
Dr Diendéré, Dr Chipenda Dansokho, Ms Rocque, Ms Julien, and Drs Légaré, Côté, Pilote, Grad, Giguère, and Witteman designed the study. Dr Diendéré, Ms Mahmoudi, Dr Jacob, Dr Casais, and Dr Chipenda Dansokho collected data. Dr Diendéré, Dr Chipenda Dansokho, Ms Julien, Ms Rocque, and Dr Witteman conducted data analysis. Drs Diendéré and Witteman drafted the first version of the article. Dr Diendéré, Dr Chipenda Dansokho, Ms Rocque, Ms Julien, Dr Légaré, Dr Côté, Ms Mahmoudi, and Drs Jacob, Casais, Pilote, Grad, Giguère, and Witteman critically revised the article and approved the final version for submission for publication.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada





{kind=link}