


Abstract
Objective To determine whether Canadian children aged 4 to 6 received well-child checks; to explore the nature of these checkups in a large family practice; and to examine the merit of using parent questionnaires about child resilience as a means of introducing a discussion about social and emotional development into this checkup.
Design Three-part mixed-methods study, using data derived from the Canadian Primary Care Sentinel Surveillance Network (CPCSSN), chart reviews of a family practice, and semistructured interviews with parents.
Setting Primary care practices associated with CPCSSN, and a large primary care practice in Kingston, Ont.
Participants Patients who were born between 2008 and 2011, and a sample of parents whose children were between the ages of 6 and 9.
Methods International Classification of Diseases, version 9, codes from CPCSSN records were used to identify the prevalence of well-child checks in the 4-to-6 age group. Then 110 randomly selected charts from a large family practice were audited for inclusion of behavioural and social assessments of those aged 4 to 6. Finally, randomly selected parents from the same practice were invited to pilot-test the PERIK (Positive development and resilience in kindergarten) resilience questionnaire, interviewed about its merit, and asked to recall whether the identified areas of child development had been included in previous well-child checkups.
Main findings Data from CPCSSN indicated that 11% of Canadian children aged 4 to 6 had had an explicit well-child check by their family physician. Among the reviewed charts from the one practice, social context was documented for 45% of them, but social and behavioural development was usually not recorded. The 42 parents interviewed found the PERIK questionnaire useful, but not perfect, for opening discussions about aspects of child development that they had not realized were central to the child’s future health.
Conclusion This study offers an initial approach to exploring resilience in children and therefore addressing recognized and alterable predictors of adult well-being. Early social and emotional development predicts resilience that, in turn, foreshadows future health. The PERIK questionnaire facilitated discussions that could add tremendous value to the well-child checks of children aged 4 to 6.
Children’s psychological characteristics such as optimism, self-control, confidence, social connectedness, and flexibility are malleable, build resilience, can be augmented by parenting practices and social environments, and can have a positive effect on both physical and mental health throughout life.1–4
Validated clinical methods for identifying or quantifying the various characteristics that align with child resilience are lacking. Typical checklists used in well-child checkups in North America barely touch on such development.5–7 The Rourke Baby Record (page 183)7 for the 4-to-6 age group, the standard of care throughout most of Canada, includes checklists on physical development, parenting, and school readiness, as well as on the ability to comfort someone and to separate from parents, but, again, does not include many items that check on aspects of social and emotional development.
Existing validated research inventories of child resilience are cumbersome and are neither practical for clinical use nor geared toward parents as respondents.8–10 Most instruments share a common concept of resilience as adapting and thriving in the face of adversity, and explore similar individual behavioural, social, and emotional characteristics such as self-control, optimism, mastery, confidence, and social connectedness. However, for clinical use, a suitable tool needs to be brief, available without cost, parent friendly, and age appropriate. Ideally, such a tool would need to include a scoring system to differentiate wellness from risk, a particular challenge as there is no “criterion standard” for child resilience.11,12
Without a clinical screening test for child resilience available, should primary care providers, nevertheless, try to identify relevant assets and characteristics? Such assessments would fit well with concepts of prevention and developmental monitoring that underpin well-child care,5,7 given the evidence that traits predicting resilience can be fostered in young children via simple, inexpensive interventions.13,14 Alternatively, rather than universal screening, we could offer resilience-building advice to parents of all young children. However, it would be even more efficient to include an assessment that is educational and that links to available resources customized for a particular child.15
The main argument against lengthening well-child examinations is time constraints.15,16 However, identifying key risks that can be ameliorated is the purpose of prevention. To avoid discussing social and emotional development or making an instinctive rather than evidence-based assessment of these to shorten the visit negates the value of well-child checks and of parents’ insights into their child’s development.17–19 Another alternative to universal screening has been to offer “remedial” programs to children assumed to be vulnerable (eg, Head Start program in the United States). Low socioeconomic status, having a single teenaged parent, and parental substance use have been viewed as markers of risk. However, direct study of emotional and behavioural development and of resilience suggests that low socioeconomic status and social adversity in childhood are not associated with diminished resilience.20
Our goal was to determine what preventive child care (of those aged 4 to 6) was being offered by Canadian family physicians, and whether the characteristics of resilience that are central to healthy physical and mental development were being addressed using, or despite using, current well-child check templates. A secondary aim was to test whether a brief parent questionnaire about specific characteristics relevant to resilience might be valuable in clinical settings. We did not wish to develop numeric resilience scores, but rather to identify variability so that parents of children struggling with certain behaviour patterns could be offered resources and community-based interventions.
METHODS
Design
This 3-part mixed-methods study included the following: a measure of national rates of well-child assessments for the 4-to-6 age group; chart reviews of the content of such assessments in a large academic family practice; and interviews with parents to gather qualitative information about experiences of well-child care. Ethics approval was received from the Queen’s University Research Ethics Board.
Setting
Prevalence data were from the Canadian Primary Care Sentinel Surveillance Network (CPCSSN), while charts for reviews and parents for interviews were randomly selected from 1 large family practice with 20 family physicians in the medium-sized city of Kingston, Ont.
Participants
The sentinel network CPCSSN is a data set that links the charts of 1180 Canadian family physicians21; the approximately 1.5 million patients in the database represent about 5% of the Canadian population. Only patients seen within the preceding 2 years are considered active in this data set.
From the charts of 20 family physicians in 1 large family practice (about 16 000 patients), every eighth chart (N = 110) of those born between 2008 and 2011 (N = 903) was randomly audited to determine whether the billing code of the well-child check for the 4-to-6 age group had been entered, and to examine the nature of any behavioural or developmental assessment documented on the Rourke record or in the chart itself. Data were entered into an Excel spreadsheet.
A separate, small, randomly selected sample of parents of children aged 6 to 9 from the same practice was contacted by telephone in July 2017 and invited to participate in individual semistructured interviews.
Interventions or exposures
Well-child checks were identified in CPCSSN by the ICD-9 (International Classification of Diseases, version 9) codes V20 (health supervision of a child) and V20.2 (routine child health check).22
Data extracted from the 110 full charts included age, evidence of a well-child check for the 4-to-6 age group, and documentation of 4- to 6-year immunizations, physical illnesses, behavioural or speech concerns, or any resources, advice, or follow-up offered.
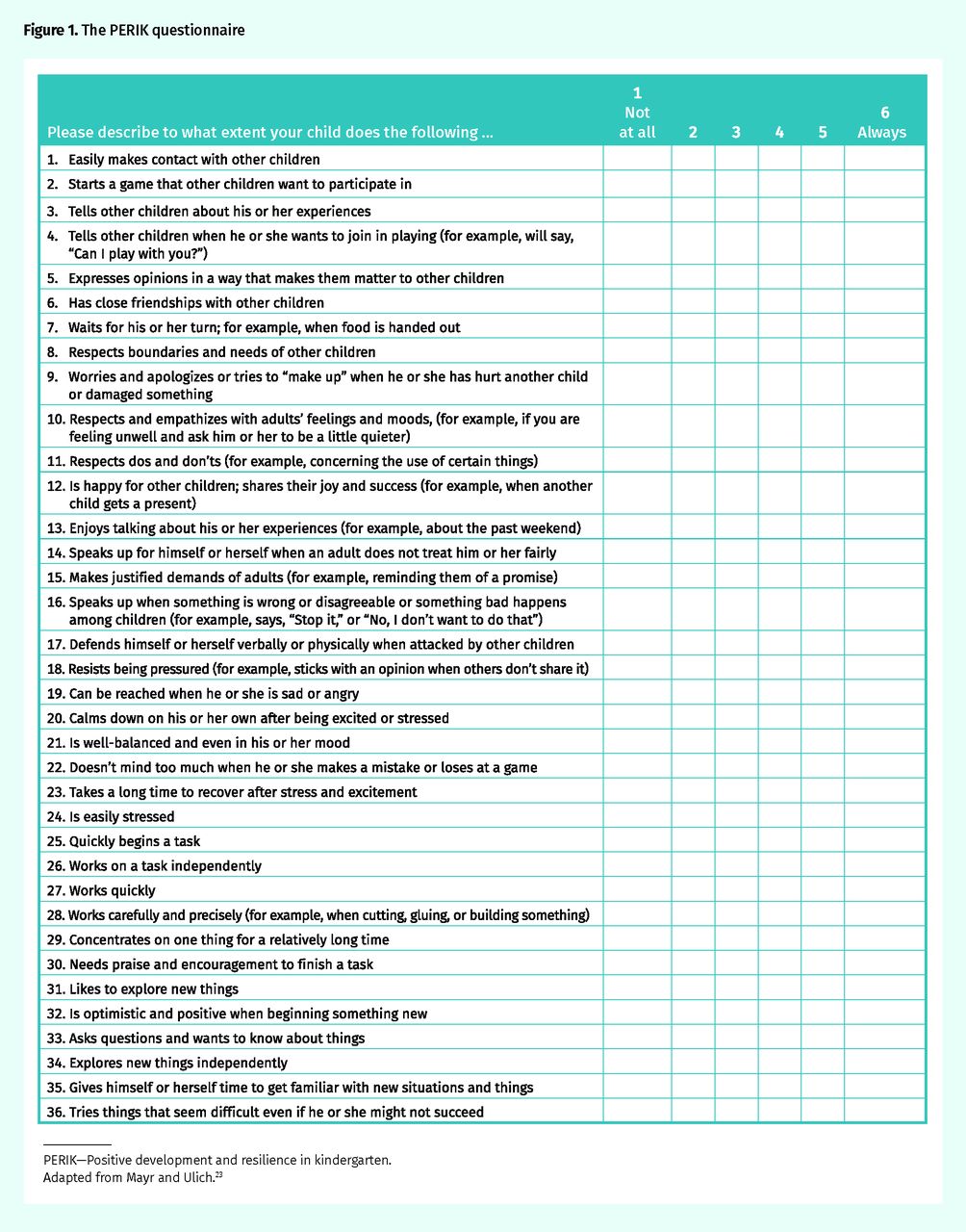
The qualitative portion of the study included in-person or telephone parent interviews conducted by 2 authors (M.J., R.L.), with each interview being conducted by only 1 of the 2 authors, to examine the phenomenon of social or behavioural developmental assessments of children. We standardized this process, then reviewed it after every 2 to 4 interviews. Parents completed the 36-item PERIK social and emotional development assessment just before the interview (Figure 1).23 This previously validated scale was developed for teachers to record the behaviour and well-being factors aligned with resilience of children aged 4 to 6. It has 6 questions about each of social performance, self-control or thoughtfulness, assertiveness, emotional stability or coping with stress, task orientation, and pleasure in exploration; these characteristics that are aligned with resilience are further described in Box 1.23 Parents were then asked questions (Box 2), shown how the PERIK would be interpreted, and offered relevant resources. Responses were not audiorecorded. Interviewers (M.J., R.L.) made extensive and often verbatim notes during the interview. These were coded, then analyzed for common themes by 3 authors (S.P.P., M.J., and R.L.), first independently and then together. What emerged was the essence of parents’ experiences, that is, what they experienced and how they experienced it.
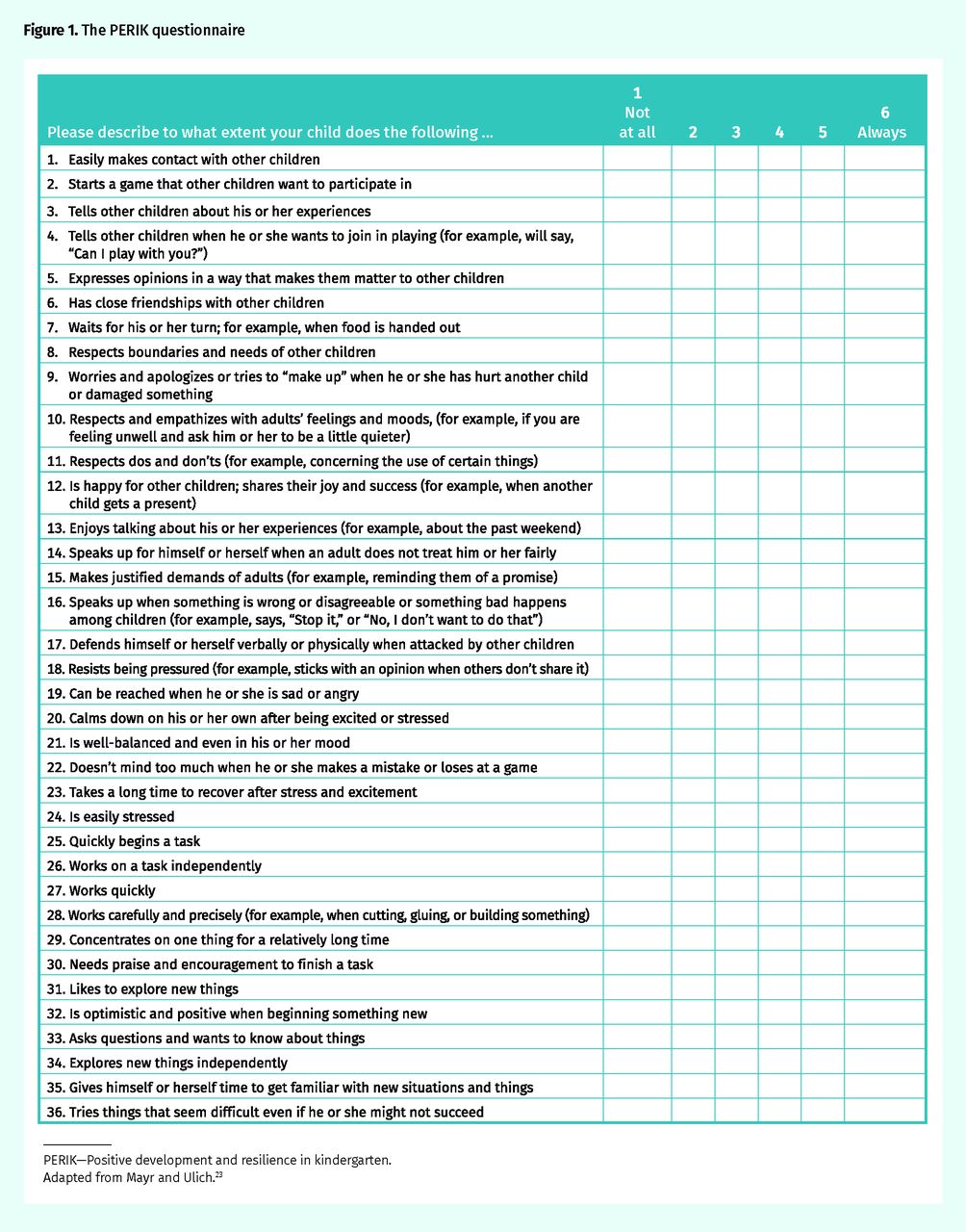
The PERIK questionnaire
PERIK—Positive development and resilience in kindergarten.
Adapted from Mayr and Ulich.23
Characteristics that align with resilience in the PERIK questionnaire
The 6 characteristics addressed in the PERIK questionnaire that are considered to be part of resilience are as follows:
Making contact or being social: how the child makes contact with and gets along with other children
Self-control or being thoughtful: how the child waits and respects rules, and respects the feelings and needs of others
Assertiveness or sticking up for yourself: how the child shares his or her experiences and feelings, and speaks up for himself or herself
Dealing with emotions or coping with stress: how the child stays calm or handles exciting or stressful situations
Doing tasks: how the child starts a task, works through it, and works on his or her own
Pleasure in exploring: how the child approaches new things
PERIK—Positive development and resilience in kindergarten.
Data from Mayr and Ulich.23
Post-PERIK discussion questions
Were there any questions that were hard to understand or didn’t make sense to you?
Were there any questions that were asked in the questionnaire that you think would be useful or valuable for a doctor to ask during a well-child visit?
Are there any other questions that were not asked in the questionnaire that you think would be useful or valuable for a doctor to ask during a well-child visit?
Do you think that this questionnaire helped bring up information about your child that you have not discussed before with your doctor?
Have these ideas been discussed by anyone else with you before? Has your doctor ever asked you about any of these behaviours as they relate to your child?*
Do you think it would be valuable for your doctor to ask these questions during a well-child visit?
The 6 categories we listed before were characteristics that have been linked to resilience.† Is there anything else you think makes children better at bouncing back and thriving when they face life’s ups and downs?
PERIK—Positive development and resilience in kindergarten.
*This question was introduced with the following: As you may have noticed, some of the questions you answered were related to each other. The questions were about 6 key characteristics that research has shown help kids respond with resilience to life’s ups and downs. Resilience is the ability to steer through life challenges and find ways to bounce back and thrive. Helping to improve a child’s resilience is very important, and research has shown that kids who are more resilient are healthier adults.
†These characteristics are found in Box 1.
Outcomes
Our population-level outcome was the proportion of children aged 4 to 6 in the CPCSSN data set who received a well-child check. The nature of that check was determined via the random chart reviews of 20 physicians in an academic family practice. Finally, individual-level assessments of parents’ recollections of whether their child’s behaviour patterns and social and emotional development were explored in well-child checks was ascertained using the PERIK as the “door opener” to further discussion.
Findings
Our findings on the prevalence and the nature of well-child checks in Canadian family practices, as well as the themes that emerged from our interviews with parents and their opinions about using the PERIK questionnaire to introduce discussions on the child’s social and emotional development, were as follows.
Prevalence of well-child checks in Canadian family practices.
Of the 21 876 children aged 4 to 6 in CPCSSN (2015 to 2016), 24% had had a visit coded as health supervision of a child, and 11% (n = 2 475) (95% CI 10.89% to 11.73%) of them had been seen specifically for a well-child check. This proportion was similar for boys and girls and for the time frame 2014 to 2015.
Nature of audited well-child checks.
As detailed in the methods section, randomly selected charts for 12% (N = 110) of those born between 2008 and 2011 and patients of 20 different physicians in one teaching practice were selected for review. Most of these patients had had the well-child check for children aged 4 to 6 (83 of 110; 75%), and it was performed by family physicians, residents, or nurse practitioners. Of the remaining 27, 16 had received age-specific immunizations, 2 had refused these, and 9 had no record of this vaccination.
Among the 83 children who had had the well-child check, there was documentation of the following concerns: physical (30%), speech (8%), or behaviour (11%). Social and family context issues, whether positive (parent reads to child) or negative (child protection services involved), were recorded for 37 (45%) children.
At least 1 of the PERIK’s 6 dimensions of social and emotional well-being was charted for 34 of 83 (41%) children. This documentation was sometimes minimal (“in school”) but occasionally detailed (“does not speak up in class”; “perfectionistic tendencies”; “has friends”; “teacher concerns about speaking out of turn”). Some chart entries spoke to aspects of resilience not addressed by the PERIK tool, such as “perfectionist tendencies” or “talkative, constantly walking around room, climbing on chair during interview, but very cooperative for exam.”
Parent interviews.
Telephone invitations to parents of 83 children resulted in 65 (78%) agreeing to participate in the semistructured interview, to complete the PERIK questionnaire before the interview, and to discuss the questionnaire and their previous experiences with well-child care. After 20 interviews we did an initial thematic analysis. Although themes were generally being repeated, we proceeded with another 22 interviews to guarantee saturation.
Themes: The 3 themes that emerged from these qualitative interviews were as follows: well-child care’s focus is physical health and growth; social, behavioural, and emotional development are not presented as medical or health matters by family physicians; and parents are keen to talk about development and resilience. In general, parents reported that their recollection of well-child checks was that they had focused on physical development. None of the parents recalled discussing aspects of child resilience with a primary care provider, and few recalled being questioned about their child’s behaviour, interactions, or social and emotional development.
Parents’ opinions about the PERIK questionnaire: Parents found the PERIK questionnaire useful for starting discussions about their child’s development. They appreciated questions about social interaction, emotional stability, coping with stress, attention span, and self-assertiveness, but had difficulty generalizing about something as context-dependent as task orientation. Questions requiring a teacher’s familiarity with their child’s group interactions (eg, assertiveness) were also challenging. Parents noted that the PERIK missed some important domains such as family stability and communication skills. Nevertheless, using the questionnaire as a door opener signaled that behaviour, social, and emotional development, as well as interactions with others, were relevant to health and, therefore, part of a well-child assessment. Whether the outcome of such a discussion was receiving reassurance or validation of, as well as referral for, concerns, or direction to resources to foster healthy development, parents welcomed such conversations.
DISCUSSION
In keeping with American evidence, it would appear that the proportion of Canadian children aged 4 to 6 receiving preventive well-child checks within family practices is less than optimal.24 Ours is the first study to not only quantify the prevalence of such checks, but to also delve into their content and examine methods for introducing the concept of resilience. Although templates used in North America include checklists about social development, school readiness, and obedience,5–7 in reality the medical assessment of the 4-to-6 age group prioritizes physical health. Based on documentation or parents’ recollections, we have found that even at explicit well-child checks, social performance, self-control, assertiveness, emotional stability, task orientation, and pleasure in exploration, all elements of resilience, might be rarely explored. In the face of limited questions about development, parents assume that such matters are not relevant to the encounter, even though these traits and behaviour patterns are key drivers of adult mental and physical well-being.3,4,25,26 Further, because resilience can be augmented, often by simple interventions and resources that are readily available, it is worth exploring.13,14 Perhaps it is no surprise that current well-child care, with its emphasis on physical rather than emotional or behavioural function, has minimal effect on subsequent health.25
The PERIK questionnaire was easily understood, efficient—taking less than 5 minutes to complete—and useful in triggering discussions about children’s social and emotional development. Participants noted limitations of this questionnaire as well, but believed it could open up conversations they had not had with primary care providers. Using such a parent questionnaire might circumvent the tendency for some providers to skip components of check-up templates or to check them off without discussion, based only on the caregiver’s impressions of the child. Others have demonstrated that despite health professionals’ education, parents are far more accurate in identifying children who would benefit from developmental interventions.17–19 The PERIK questionnaire is neither the only8 nor the perfect set of questions, but until a better, brief questionnaire is developed and validated, it appears to be adequate.
Some primary care providers did discuss social and emotional development and offered resources to parents; however, a questionnaire might precipitate a more systematic and consistent approach. Conversely, a few of the family physicians’ charts included deeper information about social and behavioural function and resilience than would arise from the superficiality of the questionnaire used alone.
Limitations
The actual proportion of children receiving the well-child check for the 4-to-6 age group in Canada might deviate from what we report. As CPCSSN excludes patients who were not seen in the preceding 2 years, this could underestimate the denominator in our calculations. The ICD-9 codes capture visits beyond well-child checks and therefore might have distorted estimates. The difference in proportions receiving this checkup nationally and locally suggests an inability to identify all such visits in CPCSSN, a possible lack of documentation by the family physician when a child receives care elsewhere, or a higher standard of care in the audited practice than nationally. In some parts of Canada and among some providers, the Rourke record might not be the standard. Further, CPCSSN data only track care by family physicians and therefore miss well-child visits provided by pediatricians or public health nurses.
Although there is no evidence that those studied differ from the Canadian population, we are cautious about generalizing findings. Despite a high response rate, we cannot rule out selection bias in our parental survey and are particularly reluctant to claim external validity for the qualitative component of this study.
Relying on charting to determine what occurred during encounters might miss the depth of discussions. Conversely auditing Rourke Baby Record check boxes for behavioural assessment might overestimate whether topics were discussed. Although it is one of the more feasible screening tests available for resilience, the PERIK questionnaire was developed for use by teachers and not parents, includes some questions parents can only speculate about, and excludes others of relevance. Finally, parents’ reports of care experienced might be subject to recall bias in either direction.
Conclusion
Much of early primary care is preventive and aptly referred to as well-child checks. There appears to be inconsistency in family medicine’s provision of well-child checks among the 4-to-6 age group. We might be missing an opportunity to assess social and emotional development and to offer available and evidence-based resources that foster resilience. Incorporating this domain into well-child care seems logical and essential to augmenting preventive value. A questionnaire like the PERIK, although not perfect, could facilitate discussions of precursors to long-term physical and mental well-being, that is, social and emotional development and resilience, until such time as a much-needed clinical screening tool is developed and validated.
Notes
Editor’s key points
▸ The well-child check for the 4-to-6 age group is a standard of preventive care in Canada; however, social and emotional traits that are malleable and augment long-term health are not explicitly evaluated. Clinicians might be missing an opportunity to assess children’s social and emotional development and to offer parents available evidence-based resources that foster resilience.
▸ Incorporating a questionnaire like PERIK (Positive development and resilience in kindergarten) into the well-check domain can facilitate discussions of precursors to long-term physical and mental well-being—that is, social and emotional development and resilience—until a clinical screening tool is developed and validated.
▸ This study found that even at explicit well-child checks, the elements of resilience—social performance, self-control, assertiveness, emotional stability, task orientation, and pleasure in exploration—are rarely explored. In the face of limited questions about development, parents assume that such matters are not relevant to the well-check encounter, even though these traits and behaviour patterns are key drivers of future health.
Points de repère du rédacteur
▸ L’examen périodique pour enfants en santé de 4 à 6 ans est une mesure préventive au Canada; toutefois, cet examen ne couvre pas nécessairement les aspects sociaux et émotionnels, lesquels sont malléables et qui, à long terme, peuvent améliorer la santé. Les médecins pourraient donc manquer une occasion de vérifier le développement social et émotionnel des enfants, et de fournir aux parents des outils fondés sur des preuves qui favorisent la résilience.
▸ Si on ajoutait à l’examen périodique pour enfants en santé un questionnaire comme le PERIK (Positive development and resilience in kindergarten), on pourrait plus facilement discuter des facteurs qui, avec le temps, favorisent le bien-être physique et émotionnel – c’est-à-dire le développement social et émotionnel et la résilience – par exemple en créant et en validant un outil de dépistage clinique.
▸ Cette étude a observé que même avec des examens pour enfants en santé bien formulés, les éléments de résilience – performance sociale, contrôle de soi, confiance en soi, stabilité émotionnelle, adaptation aux tâches spécifiques et plaisir d’explorer – sont rarement abordés. Comme il y a trop peu de questions sur le développement, les parents assument que ces sujets ne sont pas importants dans l’examen périodique de l’enfant en santé, malgré le fait que les divers types de caractères et de comportements sont des éléments clés de la santé future.
Footnotes
Contributors
All authors contributed to the concept and design of the study; data gathering, analysis, and interpretation; and preparing the manuscript for submission.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada





{kind=link}